Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
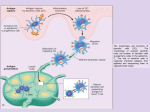
There are four types of hypersensitivity reaction mediated by immunological mechanisms that cause tissue damage Types I, II and III are antibody-mediated and are distinguished by the different types of antigens recognized and the different classes of antibody involved. Type I responses are mediated by IgE, which induces mast-cell activation, whereas types II and III are mediated by IgG, which can engage Fcreceptor and complement-mediated effector mechanisms to varying degrees, depending on the subclass of IgG and the nature of the antigen involved. Type II responses are directed against cell-surface or matrix antigens, whereas type III responses are directed against soluble antigens, and the tissue damage involved is caused by responses triggered by immune complexes. Type IV hypersensitivity reactions are T cell-mediated and can be subdivided into three groups. In the first group, tissue damage is caused by the activation of macrophages by TH1 cells, which results in an inflammatory response. In the second, damage is caused by the activation by TH2 cells of inflammatory responses in which eosinophils predominate; in the third, damage is caused directly by cytotoxic T cells (CTL). IPERSENSIBILITA’ DI TIPO II • È MEDIATADA ANTICORPI DIRETTI VERSO ANTIGENI PRESENTI SULLA SUPERFICIE CELLULARE O SULLA MATRICE EXTRACELLULARE • Antigene intrinseco della membrana cellulare oppure della matrice • Antigene esogeno (metabolita di farmaci adsorbito sulle superfici cellulari o sulla matrice IPERSENSIBILITA’ TIPO II Schematic illustration of the three major mechanisms of antibody-mediated injury. A, Opsonization of cells by antibodies and complement components and ingestion by phagocytes. Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier B, Inflammation induced by antibody binding to Fc receptors of leukocytes and by complement breakdown products. Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier C, Antireceptor antibodies disturb the normal function of receptors. In these examples, antibodies against the thyroid stimulating hormone (TSH) receptor activate thyroid cells in Graves disease, and acetylcholine (ACh) receptor antibodies impair neuromuscular transmission in myasthenia gravis. Stimolazione Inibizione Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier Effector mechanisms of antibodymediated disease. A. Antibodies opsonize cells and may activate complement, generating complement products that also opsonize cells, leading to phagocytosis of the cells through phagocyte Fc receptors or C3 receptors. B. Antibodies recruit leukocytes by binding to Fc receptors or by activating complement and thereby releasing by-products that are chemotactic for leukocytes. C. Antibodies specific for cell surface receptors for hormones or neurotransmitters may stimulate the activity of the receptors even in the absence of the hormone (left panel) or may inhibit binding of the neurotransmitter to its receptor (right panel). TSH, thyroid-stimulating hormone. Downloaded from: StudentConsult (on 17 November 2008 06:03 PM) © 2005 Elsevier MALATTIA EMOLITICA DEL NEONATO Downloaded from: StudentConsult (on 19 November 2008 09:17 PM) © 2005 Elsevier Downloaded from: StudentConsult (on 19 November 2008 09:17 PM) © 2005 Elsevier Test di Coombs Usato per rilevare la presenza di Ab sugli eritrociti dei pazienti Se ci sono anticorpi gli eritrociti sono agglutinati dall’aggiunta di anti-immunoglobuline umane Reazioni verso antigeni dei gruppi sanguigni si verificano nelle anemie emolitiche autoimmuni Il Test di Cooms può dare informazioni utili e può darle anche nei casi di Ab sui globuli rossi indotti in trasfusioni non compatibili e nella malattia emolitica del neonato Downloaded from: StudentConsult (on 19 November 2008 09:17 PM) © 2005 Elsevier Downloaded from: StudentConsult (on 19 November 2008 09:17 PM) © 2005 Elsevier IPERSENSIBILTA’ TIPO III • I COMPLESSI ANTIGENE-ANTICORPO PRODUCONO DANNI TISSUTALI SOPRATTUTTO PROVOCANDO INFIAMMAZIONE NEI SITI DI DEPOSITO • La presenza di complessi Ag-Ab in circolo non implica la presenza di malattia; • Due tipi di Ag provocano lesioni da Immunocomplessi: – Ag esogeno (batterio, virus) – Ag endogeni (self) • Malattie da immunocomplessi possono essere – Generalizzate o localizzate IPERSENSIBILITA’ DI TIPO III Schematic illustration of the three sequential phases in the induction of systemic immune complex-mediated disease (type III hypersensitivity). •I grandi complessi formati da importante eccesso di Ag sono rapidamente rimossi •Dalla circolazione da parte dei fagociti mononucleati e quindi sono relativamente innocui I complessi più “pericolosi” sono di piccole e medie dimensioni, formati da lieve eccesso di Ag, che legano meno avidamente le cellule fagocitarie e quindi circolano più a lungo. FATTORI CHE INFLUENZANO IL DEPOSITO DEGLI IMMUNOCOMPLESSINEI TESSUTI Carica degli immunocomplessi, valenza dell’antigene, avidità dell’Ab affinità dell’Ag per le varie Componenti tissutali, struttura tridimensionale dei complessi e fattori emodinamici Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier Pathogenesis of immune complex-mediated tissue injury. The morphologic consequences are depicted as boxed areas. Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier MALATTIA DA SIERO ACUTA Prototipo della malattia sistemica da immunocomplessi Serum sickness is a classic example of a transient immune complex-mediated syndrome. An injection of a foreign protein or proteins leads to an antibody response. These antibodies form immune complexes with the circulating foreign proteins. The complexes are deposited in small vessels and activate complement and phagocytes, inducing fever and the symptoms of vasculitis, nephritis, and arthritis. All these effects are transient and resolve when the foreign protein is cleared. Figure 6-17 Immune complex vasculitis. The necrotic vessel wall is replaced by smudgy, pink "fibrinoid" material. (Courtesy of Dr. Trace Worrell, Department of Pathology, University of Texas Southwestern Medical School, Dallas, TX.) Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier Il tempo di reazione è quello che distingue il fenomeno di Arthus dalla reazione di tipo I Sequence of immunological responses in experimental acute serum sickness. Injection of bovine serum albumin into a rabbit leads to the production of specific antibody and the formation of immune complexes. These complexes are deposited in multiple tissues, activate complement (leading to a fall in serum complement levels), and cause inflammatory lesions, which resolve as the complexes and the remaining antigen are removed. (Adapted from Cochrane CG. Immune complex-mediated tissue injury. In Cohen S, PA Ward, and RT McCluskey [eds]. Mechanisms of Immunopathology. Werbel & Peck, New York, 1979, pp 29-48. Copyright 1979, Wiley-Liss, Inc.) Downloaded from: StudentConsult (on 17 November 2008 06:03 PM) © 2005 Elsevier Types of antibody-mediated diseases. Antibodies may bind specifically to tissue antigens (A), or they may be deposited as immune complexes that are formed in the circulation (B). In both cases, the deposited antibodies induce inflammation, leading to tissue injury. Downloaded from: StudentConsult (on 17 November 2008 06:03 PM) © 2005 Elsevier Pathologic features of antibody-mediated glomerulonephritis. A. Glomerulonephritis induced by an antibody against the glomerular basement membrane (Goodpasture's syndrome): the light micrograph shows glomerular inflammation and severe damage, and immunofluorescence shows smooth (linear) deposits of antibody along the basement membrane. B. Glomerulonephritis induced by the deposition of immune complexes (SLE): the light micrograph shows neutrophilic inflammation, and the immunofluorescence and electron micrograph show coarse (granular) deposits of antigen-antibody complexes along the basement membrane. (Immunofluorescence micrographs are courtesy of Dr. Jean Olson, Department of Pathology, University of California San Francisco, and the electron micrograph is courtesy of Dr. Helmut Rennke, Department of Pathology, Brigham and Women's Hospital, Boston.) Tipo II Tipo III (Immunofluorescence micrographs are courtesy of Dr. Jean Olson, Department of Pathology, University of California San Francisco, and the electron micrograph is courtesy of Dr. Helmut Rennke, Department of Pathology, Brigham and Women's Hospital, Boston.) Downloaded from: StudentConsult (on 17 November 2008 06:03 PM) © 2005 Elsevier IPERSENSIBILITA’ DI TIPO IV Cellulo-mediata Mechanisms of T cell-mediated (type IV) hypersensitivity reactions. A, In delayed type hypersensitivity reactions, CD4+ T cells (and sometimes CD8+ cells) respond to tissue antigens by secreting cytokines that stimulate inflammation and activate phagocytes, leading to tissue injury. B, In some diseases, CD8+ cytolytic T lymphocytes (CTLs) directly kill tissue cells. APC, antigen-presenting cell. Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier Schematic illustration of the events that give rise to the formation of granulomas in cell-mediated (type IV) hypersensitivity reactions. Note the role played by T cell-derived cytokines. Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier The stages of a delayed-type hypersensitivity reaction. The first phase involves uptake, processing, and presentation of the antigen by local antigen-presenting cells. In the second phase, TH1 cells that were primed by a previous exposure to the antigen migrate into the site of injection and become activated. Because these specific cells are rare, and because there is little inflammation to attract cells into the site, it can take several hours for a T cell of the correct specificity to arrive. These cells release mediators that activate local endothelial cells, recruiting an inflammatory cell infiltrate dominated by macrophages and causing the accumulation of fluid and protein. At this point, the lesion becomes apparent. The delayed-type (type IV) hypersensitivity response is directed by chemokines and cytokines released by TH1 cells stimulated by antigen. Antigen in the local tissues is processed by antigen-presenting cells and presented on MHC class II molecules. Antigen-specific TH1 cells that recognize the antigen locally at the site of injection release chemokines and cytokines that recruit macrophages to the site of antigen deposition. Antigen presentation by the newly recruited macrophages then amplifies the response. T cells can also affect local blood vessels through the release of TNF-a and TNF-b, and stimulate the production of macrophages through the release of IL-3 and GM-CSF. Finally, TH1 cells activate macrophages through the release of IFN-g and TNFa, and kill macrophages and other sensitive cells through the cell-surface expression of the Fas ligand. • Type IV hypersensitivity responses. These reactions are mediated by T cells and all take some time to develop. They can be grouped into three syndromes, according to the route by which antigen passes into the body. In delayed-type hypersensitivity the antigen is injected into the skin; in contact hypersensitivity it is absorbed into the skin; and in gluten-sensitive enteropathy it is absorbed by the gut Mechanisms of T cell-mediated diseases. A. In delayed-type hypersensitivity reactions, CD4+ T cells (and sometimes CD8+ cells) respond to tissue antigens by secreting cytokines that stimulate inflammation and activate phagocytes, leading to tissue injury. APC, antigen-presenting cell. B. In some diseases, CD8+ CTLs directly kill tissue cells. Downloaded from: StudentConsult (on 17 November 2008 06:03 PM) © 2005 Elsevier Delayed hypersensitivity in the skin. A, Perivascular infiltration by T cells and mononuclear phagocytes. B, Immunoperoxidase staining reveals a predominantly perivascular cellular infiltrate that marks positively with antiCD4 antibodies. (Courtesy of Dr. Louis Picker, Department of Pathology, University of Texas Southwestern Medical School, Dallas, TX.) Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier A section of a lymph node shows several granulomas, each made up of an aggregate of epithelioid cells and surrounded by lymphocytes. The granuloma in the center shows several multinucleate giant cells. (Courtesy of Dr. Trace Worrell, Department of Pathology, University of Texas Southwestern Medical School, Dallas, TX.) Downloaded from: StudentConsult (on 20 March 2010 03:32 PM) © 2005 Elsevier Skin tests are carried out by introducing 0.02 ml of extract intradermally. With allergens such as pollen, cat, or dust mite, the positive reaction is an immediate (i.e. within 20 min) wheal, which in some cases is followed by an indurated response occurring late (i.e. at 4-12 hours). Non-allergic individuals make no discernible reaction to testing with these allergens. A delayed skin response is the commonest form of positive response to tuberculin, tetanus, and mumps, or to fungi such as Trichophyton and Candida spp. The skin typically shows no reaction up to 12 hours and then gradually develops an erythematous, indurated, delayed hypersensitivity response, which is maximal at 24-48 hours. Patch tests are performed by applying a gauze pad with allergen to a patch of skin that has been mildly abraded. This procedure may give an immediate wheal response, but this is followed at 24-48 hours by an indurated, erythematous response, which has many of the features of eczema. The patch test is not a diagnostic test, but has provided extensive information about the role of allergens in atopic dermatitis. Downloaded from: StudentConsult (on 16 March 2010 11:42 AM) © 2005 Elsevier