Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
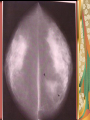
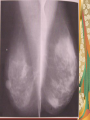
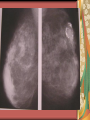
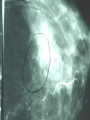
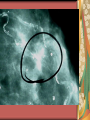
HISTORY OF MAMMOGRAPHY First proposed in 1924 Article published in 1930 1960’s Robert Egan considered the “Father of Mammography” Also 1960’s Charles Gros developed 1st dedicated Mammo unit (Dose 8-12 rads) 1971 Xeroradiography (Dose 2-4rads) IMPORTANT FACTS ABOUT MAMMOGRAPHY Mammography is the most sensitive and accurate screening modality available for detecting early breast cancer. It is not always diagnostically specific. It complements but cannot replace regular physical exams and BSE. STATISTICS: Breast Cancer Most common cancer among women Second leading cause of cancer deaths ACS projects 212,920 new cases for women in 2006 Of these, 40,970 expected to die. STATISTICS One of eight women in the U.S. will develop breast cancer. Approximately 50% of cancers detected at a screening are impalpable 9% of breast cancers are not detected by Mammography. WHAT ABOUT MEN? An estimated 1720 cases expected in men for 2006. Approximately 460 men will die. FREQUENCY Age 35 for baseline National Institutes of Health (NIH) states screening ages 40-49 every 12 years; every year over 50 ACS recommends every year after age 40 Patients with strong family histories should start 10 years prior to age of family member with cancer. LUMP SIZE Average size lump found by occasional BSE is 2.5cm (1”) Ave lump found by Mammography is .5 cm (1/4”)(5yr survival 95%) On average, lesions detected by mammography are 8 years old. By 2 cm nodes are involved in 5060% of the cases. 5 year survival rate is 60% RISK FACTORS MAJOR RISK FACTORS Gender, Age Personal History of Breast or other CA Family History MINOR RISK FACTORS Hormonal Factors Child-bearing Body Shape/Type Breast Structure Ethinic Origin DOSE 1969 1971 Patient dose 8-12 rads Xeroradiography introduced Dose 2-4 rads 1986 ACR recommends <300mrad per single view with grid 1994 4 view =.15 rads or 150mrads Dental = 400 mrad CA Therapy =500 rads COMPARISON OF DOSE TO DAILY LIFE The risk of death from developing breast cancer due to radiation received from a single mammographic examination is equal to the risk of: Traveling 80 miles by air Traveling 10 miles by car Smoking 1/8 of one cigarette 11/2 minutes of mountain climbing 3 minutes of being a man age 60 Eating 40 TBSP peanut butter EXPERIENCE INITIAL Certification or 40 hours of Mammography training. 25 supervised exams CONTINUING 15 CE every triennium 100 exams every year REWARD Relaxed environment One on one patient contact Saving lives No call or weekends Collapsed Envelope 11.5 Palpable Giant Fibroadenoma LYMPHOMA ARCHITECTURAL DISTORTION LATE STAGE PALPABLE CA INSPISSATED DEBRIS AND DUCT ECTASIA POST SURGICAL