Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
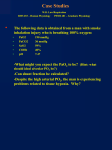
) Given the following arterial blood gas values: pH: 7.56 PaCO2: 31 mm Hg HCO3: 27 mEq/l PaO2: 56 mm Hg What is(are) the most likely acid-base state(s) in the patient? a) acute respiratory alkalosis b) chronic respiratory alkalosis c) respiratory alkalosis and metabolic alkalosis d) respiratory acidosis and metabolic acidosis e) respiratory alkalosis and metabolic acidosis Answer: c The subject is hyperventilating with an elevated pH, indicating respriratory alkalosis. However, with hyperventilation bicarbonate goes down from the simple excretion of CO2 in the hydration equation; CO2 + H2O <----> HCO3- + H+. As CO2 is excreted both bicarbonate and hydrogen ion fall. With simple hyperventilation and no other acid base disorder the HCO3- should fall slightly from the normal value of 24 mEq/L, and be about 22-23 mEq/L. In this example it is 27 mEq/L, indicating a comcomitant mild metabolic alkalosis. 2) A healthy young woman, toward the end of a mile run in the gym, has increased her heart rate by 50% over baseline. At that point, which one of the following statements is least likely to be true. a) She is tachypneic and/or hyperpneic. b) She is hyperventilating. c) Her alveolar ventilation is increased above its resting baseline value. d) Her CO2 production is increased above its resting baseline value. e) Her PaO2 is normal. Answer: b Hyperventilation is defined excess alveolar ventilation for CO2 production, which always leads to a low PaCO2 (if the subject starts from normal value of @40 mm Hg). It is NOT the same as tachypnea or hyperpnea. Since this healthy young woman has increased her heart rate with exercise, she has surely increased her CO2 production as well, and as a result her respiratory rate to blow it off. Thus she is tachypneic and or hyperpneic in order to increase her alveolar ventilation, which is necessary to excrete her excess metabolic CO2 production. She should NOT be hyperventilating though, as her increase in CO2 production will be balanced by increased alveolar ventilation, leaving PaCO2 unchanged. All of this is explained in the 4 Most Important Equations in Clinical Medicine (PaCO2 Equation). 3) Which of the following changes will most increase arterial oxygen delivery? a) PaO2 from 60 to 95 mm Hg b) cardiac output from 4 to 5 L/min c) hemoglobin from 9 to 10 grams% d) atmospheric pressure from 1 to 2 atmospheres e) arterial pH from 7.30 to 7.50 Answer: b Oxygen delivery is oxygen content x cardiac output. a) This change in PaO2 will increase SaO2 from about 90% to 98%, in effect increasing CaO2 about 9% and O2 delivery about the same. b) This is a 25% increase in cardiac output, which will increase oxygen delivery 25%. c) This is an 11% increase in oxygen content, which will increase O2 delivery the same percentage, 11%. d) This change will increase PaO2 from about 100 to 200 mm Hg, for a neglible increase in SaO2 and oxygen content. e) This change will shift the O2 dissociation curve to the left and increase SaO2 slightly, perhaps by 2-3%. 4) Given the following arterial blood gas values: pH: 7.40 PaCO2: 20 mm Hg HCO3: 12 mEq/l What is(are) the most likely acid-base state(s) in the patient? a) metabolic acidosis with full compensation b) respiratory alkalosis with full compensation c) metabolic acidosis and respiratory alkalosis d) metabolic acidosis and metabolic alkalosis e) normal acid-base state Answer: c A normal pH with abnormal PaCO2 or HCO3 indicates two or more acid base disorders. Full compensation (back to baseline) is never achieved with a single acid-base disorder. 5) All of the following are true about SpO2 as measured by pulse oximeters that utilize two wavelengths of light (i.e., most pulse oximeters in use today) except: a) Can can be normal even when PaCO2 is >200 mm Hg. b) Is not affected by anemia. c) Does not differentiate oxyhemoglobin from carboxyhemoglobin. d) Is not affected by excess methemoglobin. e) Requires a detectable pulse. Answer: d SpO2 falls in the presence of excess methemoglobin, approimately 1/2 percent for every percent of MetHb. Thus 10% MetHb will give about a 5% decline in SpO2. All the other statements are true. 6) All of the following are true about non-arterial assessment of oxygenation and acid-base balance except: a) if venous CO2 (measured as part of standard electrolyte panel) is truly abnormal, the patient has some type of acid-base disorder. b) in a hemodynamically stable patient, venous blood gases measured from central venous blood can be used to assess acid-base status. c) venous blood can be used in lieu of arterial blood to measure blood carboxyhemoglobin. d) the bicarbonate gap, which is (Na+ - Cl- - 39), can diagnose a metabolic alkalosis even when there is increased anion gap. e) in a stable patient with normal lungs, the difference between PaCO2 and endtidal PCO2 is 10 to 15 mm Hg. Answer: e In a normal person end tidal PCO2 is equal to PaCO2. All other statements are true. 7) One or more of the following statements (A, B, C) about PaO2 may be correct. Choose the single letter answer (a - e) that reflects which statement(s) is(are) correct. A) If the lungs and heart are normal, then PaO2 is affected only by factors that affect alveolar PO2. B) In a person with normal heart and lungs, anemia should not affect PaO2. C) The reason PaO2 falls with increasing altitude is because barometric pressure falls. a) only A) is correct. b) A) and B) are correct. c) A) and C) are correct. d) B) and C) are correct e) A), B) and C) are correct. Answer: e All 3 statements are correct. 8) A patient presents with the following arterial blood gases, drawn on room air (FIO2 = .21). pH: 7.40 PCO2: 40 mm Hg PO2: 82 mm Hg HCO3: 24 mEq/L Which of the following statements is most accurate? a) The patient does not have an acid-base disorder. b) To determine if there is an acid base disorder you need to know the measured serum bicarbonate, since the HCO3 from blood gases is only a calculation. c) Need to know patient's respiratory rate, as PaCO2 may be inappropriately "normal" and signify a respiratory acidosis. d) A patient can have normal blood gases if two metabolic acid-base disorders oppose to give normal bicarbonate. e) The PaO2 is lower than predicted for a patient breathing room air. Answer: d Metabolic acidosis and metabolic alkalosis can co-exist, so the patient ends up with a normal HCO3 and PaCO2. Serum electrolytes can make the diagnosis by showing increased anion gap; in the presence of normal HCO3, increased AG would indicate the two disorders. See also Question 14. 9) A patient with respiratory failure has the following arterial blood gases (FIO2 = .21, sea level): pH: 7.20 PCO2: 70 mm Hg PO2: 60 mm Hg SaO2: 86% Which of the following is the least likely cause of these abnormal blood gases? a) congestive heart failure b) narcotic overdose c) myasthenia gravis d) flail chest e) Guillain Barre' Syndrome Answer: a All of these conditions can lead to respiratory acidosis, but congestive heart failure would be least likely to do so without increasing the A-a O2 difference. Alveolar PO2 in this example is .21(760-43) - 1.2(PaCO2) = 150-84 = 66. Thus the (PAO2 - PaO2), or so-called 'A-a gradient' is normal at about 6 mm Hg. Since the other conditions can cause respiratory acidosis without involving the lung parenchyma, and thus without raising (PAO2 - PaO2), CHF is the correct answer. 10) A 42-year-old man is admitted to the hospital with dehydration and hypotension. Electrolytes show: Na+ 165 mEq/L K+ 4.0 mEq/L CO2 32 mEq/L Cl- 112 mEq/L No arterial blood gas is obtained. Which statement best applies about this patient's acid-base status? a) Electrolytes indicate the presence of metabolic acidosis. b) Electrolytes indicate the presence of metabolic alkalosis. c) Electrolytes indicate the presence of both metabolic acidosis and metabolic alkalosis. d) Need serum albumin to make any clinically useful assessment of his metabolic acid-base disorders. e) Need serum lactate to make any clinically useful assessment of his metabolic acid-base disorders. Answer: c His anion gap is Na - (CO2 + Cl) = 165 - (32+112) = 21, indicating a metabolic acidosis. His bicarbonate gap is (Na - Cl - 39) = 165 - 112 - 39 = 14, which indicates a metabolic alkalosis. Note that it is not necessary to actually calculate a bicarbonate gap, since the elevated serum CO2 (32 mEq/L) in the presence of anion gap acidosis is enought to signify concomitant metabolic alkalosis. Of course without blood gas measurements you don't know which process is predominant, but it is clear from the electrolytes that both metabolic disorders are present. You don't need to measure albumin nor lactate to make this determination. 11) A 30-year-old man, previously healthy, is brought to the ED after suffering smoke inhalation. Measured carboxyhemoglobin is 20% and hemoglobin content = 15 gm%. He has following blood gas values: PaO2: 80 mm Hg (on room air at sea level) PaCO2: 32 mm Hg pH: 7.34 SaO2: 96% (calculated) Exam shows clear lungs to auscultation and his chest x-ray is normal. From this information alone, you can determine that: a) His actual SaO2 is much lower than the calculated value. b) There is no lung abnormality present, though pulmonary disease could develop in the ensuing 24 hours. c) He has a mild metabolic acidosis associated with an increased anion gap. d) His arterial oxygen content is in the normal range. e) None of the above. Answer: a Given 20% carboxyhemoglobin, his actual SaO2 (which is the % of hemoglobin bound to oxygen) cannot be more than 80%. As to: b), a lung abnormality could be present, especially since his (PAO2-PaO2) is somewhat increased; c) no electrolyte information is given, so you don't know if he has an increased anion gap; d) no hemoglobin content is given, so you don't know his oxygen content; e) is incorrect, since a) is the answer. 12) Below are two sets of blood gases: Patient A: pH 7.48, PaCO2 34 mm Hg, PaO2 85 mm Hg, SaO2 95%, Hemoglobin 7 gm% Patient B: pH 7.32, PaCO2 74 mm Hg, PaO2 55 mm Hg, SaO2 85%, Hemoglobin 15 gm% Which is the most correct statement? a) B is more hypoxemic because PaO2 is lower than A. b) B is more hypoxemic because SaO2 is lower than A. c) A is more hypoxemic because A-a gradient is higher than B. d) A is more hypoxemic because O2 content is lower than B. e) The differences balance out and neither A nor B is more hypoxemic than the other. Answer: d Hypoxemia means low oxygen content in the blood. If you don't have oxygen content, then you might use PaO2 and/or SaO2 as a surrogate for assessing hypoxemia, but here you do have oxygen content information. The oxygen contents are (excluding contribution of dissolved O2): Patient A: 1.34 x 7 x .95 = 8.91 ml O2/dl Patient B: 1.34 x 15 x .85 = 17.09 ml O2/dl Clearly, Patient A is more hypoxemic despite having a higher PaO2 and SaO2 than Patient B. 13) State which one of the following situations would be expected to lower a patient's arterial PO2. a) anemia b) carbon monoxide poisoning c) an abnormal hemoglobin that holds oxygen with half the affinity of normal hemoglobin d) an abnormal hemoglobin that holds oxygen with twice the affinity of normal hemoglobin e) lung disease with more than a normal amount of ventilation-perfusion imbalance Answer: e PaO2 is unaffected by anemia or anything to do with hemoglobin binding. PaO2 is a function of what's inhaled (Alveolar PO2) and the state of lung architecture; the latter is defined by ventilation-perfusion abnormality (which includes right to left shunting) and diffusion barrier to oxygen transfer. By far the most common cause of low PaO2 is ventilation-perfusion imbalance -- the mechanism in virtually all acute and chronic lung diseases. 14) A 40 year-old patient is admitted to the ICU with the following lab values: BLOOD GASES pH: 7.40 PCO2: 38 mm Hg HCO3: 24 mEq/L PO2: 88 mm Hg (on room air) ELECTROLYTES, BUN & CREATININE Na: 149 mEq/L K: 3.8 mEq/L Cl: 100 mEq/L CO2: 24 mEq/L BUN: 110 mg% Creatinine: 8.7 mg% Which statement best describes the disorder(s)? a) Normal electrolytes, normal blood gases b) Abnormal electrolytes and abnormal blood gases c) Metabolic acidosis d) Metabolic alkalosis e) Metabolic acidosis and metabolic alkalosis Answer: e Electrolytes are not normal, since the anion gap is increased: AG = 149 - (100+24) = 25. Thus, there is at least a metabolic acidosis. Furthermore, since CO2 is "normal" at 24, desite an increased anion gap, there must also be a metabolic alkalosis. See also Question 8. 15) All of the following are true about cyanosis except: a) For cyanosis to manifest there needs to be 5 gm% of deoxygenated hemoglobin in the capillaries. b) Patients with normal hemoglobin manifest cyanosis at higher SaO2 values than patients with anemia. c) Cyanosis can be caused by excess methemoglobin, which is HbFe+3. d) For methemoglobin to cause cyanosis, the PaO2 generally has to be <80 mm Hg. e) Some drugs may cause cyanosis without causing vasoconstriction, or any impairment in PaO2, SaO2, or oxygen content. Answer: d Methemoglobin can cause cyanosis with a normal PaO2. All the other statements are true. See e-medicine topic on cyanosis 16) Since the early 1980s, climbers have summited Mt. Everest without supplemental oxygen. Since the barometric pressure on the summit is only 253 mm Hg, summiting (without extra O2) has only been possible due to prolonged acclimitization at altitude and profound hyperventilation. Indeed, if a a climber maintained PaCO2 of 40 mm Hg and an alveolar-arterial PO2 difference of 5 mm Hg, what would be his/her theoretical PaO2? a) 25 mm Hg b) 15 mm Hg c) 5 mm Hg d) -5 mm Hg e) -10 mm Hg Answer: e Here you use the alveolar gas equation: PAO2 = .21 (253-47) - 1.2 (40) = 43 - 48 = - 5 mm Hg Since the alveolar-arterial PO2 difference is 5 mm Hg, that would make the arterial PO2 (PaO2) = -10 mm Hg! Climbers have summited without supplemental O2 by virtue of profound, sustained hyperventilation, to level of @ 7 mm Hg. Thus PAO2 = .21 (253-47) - 1.2 (7) = 43 - 8 = 35 mm Hg Again, since the alveolar-arterial PO2 difference is 5 mm Hg, that would gives a PaO2 on the summit of @ 30 mm Hg - extremely low but survivable. 17) All are true about excess carbon monoxide except: a) shifts the oxygen dissociation curve to the left b) lowers the PaO2 c) lowers the oxygen saturation d) lowers the arterial oxygen content e) is not accounted for when SaO2 is calculated from arterial blood gas measurements Answer: b CO shifts the O2 dissociation curve left-ward, lowers SaO2 and oxygen content, and is not accounted for in the calcuation of SaO2 from PaO2 measurement. CO does not affect PaO2. 18) A mountain climber ascends from sea level to 18,000 feet over a two day period, without supplemental oxygen. With ascent all of the following factors will decrease except: a) Fraction of inspired oxygen (FIO2) b) Barometric pressure c) PaO2 d) PaCO2 e) Arterial hydrogen ion concentration Answer: a FIO2 is the same at all breathable altitudes. The barometric pressure falls with altitude, and as a consequence PaO2 falls and the climber hyperventilates. Hyperventilation results in low PaCO2 and increased pH (reduced hydrogen ion concentration). 19) You are scuba diving to a depth of 99 feet in the ocean, breathing compressed air from a tank. At this depth, compared to the surface, your arterial PO2 will be approximately: a) the same b) 2x the surface value c) 3x the surface value d) 4x the surface value e) dependent on amount of air pressure in the tank Answer: d Each 33 feet of depth in sea water doubles the ambient pressure; thus at 99 feet of depth the ambient pressure is 4x the surface pressure, and PaO2 will be about 4x that at sea level. 20) While all of the following conditions could possibly be managed without measuring arterial blood gases, in which one would blood gases be most helpful? a) A 40-year-old woman suffering an asthma exacerbation. Her peak expiratory flow rate is 65% of predicted and SpO2 is 95% on room air. b) A 17-year-old-high school student who presents to the ED with hyperpnea and tachypnea; history reveals he became "excited" during a church service. He has some tetanic contractions of his hands, his lungs are clear and pulse oxygen saturation is 98% on room air. c) A 68-year-old hypertensive patient has been feeling "weak" for a few days. She has been taking her anti-hypertensive medications. Electrolyte measurements show: Na+ 148 mEq/L K+ 4.0 mEq/L CO2 24 mEq/L Cl- 102 mEq/L d) A 24-year-old insulin-dependent diabetic comes to the ED, complaining of lethargy; she has not used insulin in several days. Her pulse oximeter oxygen saturation on room air is 98%. Lab values show: Glucose 750 mg% Na+ 135 mEq/L K+ 4.5 mEq/L CO2 10 mEq/L Cl- 100 mEq/L Urine 4+ ketones e) A 25 year old woman comes to the ED with chest pain. She does not smoke. SaO2 is 96% on room air and V/Q scan is read as low probability for pulmonary embolism. EKG is normal. Answer: c The patient has an anion gap metabolic acidosis and a metabolic alkalosis (see also Questions 8 and 14). Blood gases will be helpful to determine which disorder is predominant. Patients a, b, d and e can be treated without measuring blood gases. Patient d, in particular, reflects a typical case of diabetic ketoacidosis, with anion gap of 25 mEq/L. It is not necessary to measure or follow blood gases in such a patient, as long as there is response to insulin along with a rise in AG and fall in serum CO2. 21) The factor 0.863 in the PCO2 equation: a) equates dissimilar units for CO2 production and alveolar ventilation into mm Hg used for PCO2. b) accounts for the difference between alveolar ventilation and total or minute ventilation. c) accounts for the dissolved fraction of carbon dioxide. d) factors in base excess. e) is not explained by any of the above. Answer: a The PaCO2 equation, PaCO2=VCO2/VA, results in units of mm Hg. The factor 0.863 converts CO2 production units (ml/min) and alveolar ventilation units (L/min) into mm Hg. 22) The limit of human hyperventilation is a PaCO2 of about 8 mm Hg. What is the highest PaO2 (mm Hg) a patient with normal lungs could achieve breathing room air (FIO2=.21) at sea level? a) 100 b) 122 c) 135 d) 142 e) 150 Answer: c The abbreviated alveolar gas equation gas be used to answer this question: PAO2 = FIO2 (BP - 47) - 1.2 (PaCO2) PAO2 = .21 (760-47) - 1.2 (8) PAO2 = 149.7 - 9.6 = 140.1. Thus the alveolar PO2 is 140, but arterial PO2 will be somewhat lower due to the normal PAO2 - PaO2 difference. Assuming a normal PAO2PaO2 of 5 mm Hg, the highest value would be about 135 mm Hg. 23) A 45 year-old-man is treated in a hyperbaric chamber for severe carbon monoxide toxicity. Assume he is breathing 100% oxygen at 3 atmospheres of pressure, that he has normal lungs, and that hemoglobin=15 gm%, carboxyhemoglobin=40%. What is his approximate arterial oxygen content in ml/dl? a) 10 b) 13 c) 15 d) 20 e) 21 Answer: c or d Here you use the oxygen content equation. In this situation you need to include the contribution by PaO2, since it is considerably higher in a hyperbaric environment. Since the subject has normal lungs, PaO2 should be 3x normal PaO2 while breathing 100% oxygen. PaO2 on 100% oxygen with normal lungs should be around 600 mm Hg. Therefore at 3 atmospheres, PaO2 should be around 1800 mm Hg. Also, with 3 atmospheres of pressure at 100% oxygen, all the available hemoglobin binding sites will be fully saturated. However, since 40% of the sites are bound with CO (COHb = 40%), the actual SaO2 will only be 60%. Thus: CaO2 = 1.34 x Hgb x SaO2 + (.003 x PaO2) CaO2 = 1.34 x 15 x .60 + (.003 x 1800) CaO2 = 12.06 + 5.4 = 17.46 ml O2/dl Because this is between 15 and 20, either answer is accepted as correct. 24) Which one of the following statements is not true? a) If nothing else changes, as PaCO2 goes up alveolar PO2 and arterial PO2 go down. b) PaO2 is inversely related to blood pH: as pH goes up PaO2 also increases. c) If PaCO2 increases while HCO3- remains unchanged, pH always goes down. d) A high bicarbonate could reflect metabolic alkalosis or respiratory acidosis or metabolic acidosis+metabolic alkalosis. e) The SaO2 is related to hemoglobin-bound arterial oxygen content on a linear scale (i.e., a straight-line relationship). Answer: b While all the other relationships are physiologic, there is no such physiologic relationship between PaO2 and pH. True, if pH went up because of hyperventilation and the subject has normal lungs, then you would expect PaO2 to also increase. However, pH could go up because of metabolic alkalosis, which might lead to increased PaCO2 and a decreased PaO2. Or, the patient could hyperventilate and PaO2 could go down because of lung disease. There is simply no physiologic relationship that can predict direction of PaO2 when pH changes. 25) Which one of the following sets of blood gas values most likely represents a lab or transcription error? (PaCO2 and PaO2 in mm Hg, HCO3 in mEq/L, SaO2 in %. Assume all blood gases drawn at sea level.) pH PaCO2 HCO3 PaO2 SaO2 FIO 2 a) 7.40 75 45 70 75 0.21 b) 7.22 20 8 160 98 0.50 c) 7.59 25 23 60 90 0.28 d) 6.65 265 28 200 96 1.00 e) 7.48 33 24 90 60 0.21 Answer: a* A lab or transcription error is evident when the values do not fit known physiology. a) doesn't fit because the PaO2 is too high for this degree of hypoventilation: Alveolar PO2 = .21 (760 - 47) - 1.2 (75) = 150-90 = 60 mm Hg. In a clinical situation you would never have a PaO2 of 70 mm Hg when alveolar PO2 is only 60 mm Hg. (This could theoretically happen in a sudden decompression at altitude, in which case oxygen would be leaving the blood to enter the atmosphere. In that situation you wouldn't be checking blood gases!). b) reflects severe metabolic acidosis with increased PaO2 on a high FIO2. c) reflects hyperventilation with some hypoxemia. d) has been reported as an extreme example of hypercapnic oxygenation. e) shows a much lower SaO2 than expected from the PaO2, and suggests carbon monoxide toxicity. *When the quiz was first posted I had my own transcription error! The PaCO2 in blood gas set 'a' was incorrectly given as 40 mm Hg, invalidating the answer. (When scored for prizes all answers to this question were accepted.) Tie Breaker 26) A 54-year-old man with chronic obstructive pulmonary disease is seen in the Emergency Department for respiratory distress. Arterial blood gases show: pH 7.38, PaCO2 70 mm Hg, PaO2 38 mm Hg, SaO2 52% on room air (FIO2=.21, at sea level). At the same time, his oxygen saturation measured by pulse oximetry (SpO2) is 65%. Explain, in physiologic terms, reason(s) for both the low PaO2 and low SaO2. PaO2 is reduced from two physiologic causes: increased PaCO2 and ventilation-perfusion imbalance. Note that with pure hypoventilation to PaCO2 of 70 mm Hg (e.g., CNS depression with normal lungs), the resulting PaO2 should be about 60 mm Hg. This is determined by the alveolar gas equation: PAO2 = .21(760-47) - 1.2(70) = 66 mm Hg Assuming a normal A-aO2 difference of about 6 mm Hg gives a PaO2 of 60 mm Hg, which is much higher than the actual PaO2 of 38 mm Hg. The reason has to be an additional physiologic cause, which is ventilation-perfusion imbalance. Both physiologic causes of the patient's low PaO2 are a result of COPD. SaO2 is reduced because of the reduced PaO2 AND also from elevated carbon monoxide (CO) level; the latter is inferred because the SaO2 of 52% is lower than predicted from an oxygen dissociation curve based on normal pH and PaCO2 of 70 mm Hg. While elevated PaCO2 will shift the O2 dissociation slightly to the right (lowering SaO2 for a given PaO2), PaCO2 of 70 mm Hg with pH of 7.38 should give an SaO2 in the mid to high 60s. Note that elevated CO level shifts the O2 dissociation curve to the left, but that slight increase in SaO2 for a given PaO2 is miniscule compared to the absolute reduction in SaO2 brought on by excess COHb; it is essentially 1 for 1; for every percent increased COHb, SaO2 decreases by one percent.