Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
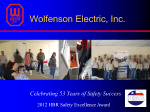
2017 John Maurer, SASHE, CHFM, CHSP Engineering Department The Joint Commission Engineering Department 2017- 1 © Copyright, The Joint Commission The Healthcare Environment Update © Copyright, The Joint Commission Survey Process Survey Process Agenda for Life Safety surveyor Evaluation starts upon arrival Specified OR Survey time both customers and surveyors Time allotted for primary surveyor responsibilities Engineering Department 2017- 3 © Copyright, The Joint Commission A single document list and tracking tool for Primary LSCS Survey Responsibilities LS.01.01.01 (SOC) LS.01.02.01 (ILSM) EC.02.03.01 (Fire Response Plan) EC.02.03.03 (Fire Drills) EC.02.03.05 (Fire Equipment Maintenance) EC.02.05.07 (Emergency Power Testing) EC.02.05.09 (Piped Medical Gas Testing and cylinders management) Engineering Department 2017- 4 © Copyright, The Joint Commission EC.02.05.01 (EP 15 – Pressure Relationships) Survey Resource Activity Guide has been updated to include “Life Safety and Environment of Care—Document List and Review Tool” This new resource is located on The Joint Commission website at http://www.jointcommission.org/life_safety_ code_information__resources/ This resource is also at the Joint Commission Connect™ extranet site Engineering Department 2017- 5 © Copyright, The Joint Commission To prepare for document review, the Survey Engineering Department 2017- 6 © Copyright, The Joint Commission Pre-Survey Checklist: EC & LS Engineering Department 2017- 7 © Copyright, The Joint Commission Pre-Survey Checklist: EC & LS LS/EC Document List & Review Tool Same tool for surveyor and organization Serves as organization prep tool and tracking tool during survey Identifies frequency Relates to standard/EP Request reflects scope of survey Engineering Department 2017- 8 © Copyright, The Joint Commission requirements EC Documents If Primary Survey Engineering Department 2017- 9 © Copyright, The Joint Commission Responsibility completed and LSCS will be conducting the EC Session, review these documents Building Tour Guidance should include Lists related standards/EPs Only guidance Does not reflect touring order Engineering Department 2017- 10 © Copyright, The Joint Commission Reflects what a tour Survey Analysis For Evaluating Risk (SAFER) Matrix © Copyright, The Joint Commission See also January 2017 Perspectives What is SAFER™? The Survey Analysis for Evaluating Risk™ (SAFER™) is a transformative approach for identifying and communicating risk levels associated with deficiencies cited during surveys. The additional information related to risk provided by the SAFER Matrix helps organizations prioritize and focus corrective actions. The SAFER Matrix™ provides one, comprehensive visual representation of The SAFER Matrix replaces the current scoring methodology, which is based on pre-determined categorizations of elements of performance (such as direct and indirect impact) – instead allowing surveyors to perform real-time, on-site evaluations of deficiencies. Placement of RFIs within the matrix will determine the level of detail required within each RFI’s Evidence of Standards Compliance follow-up. Engineering Department 2017- 12 © Copyright, The Joint Commission survey findings in which all Requirements for Improvement (RFIs) are plotted on the SAFER matrix™ according to the likelihood of the issue to cause harm to patients, staff or visitors, in addition to how widespread the problem is, based on the surveyor’s observations. The Joint Commission’s Survey Analysis for Evaluating Risk (SAFER) Matrix™ HIGH MODERATE LOW LIMITED PATTERN Scope WIDESPREAD © Copyright, The Joint Commission Likelihood to Harm a Patient/Staff/Visitor Immediate Threat to Life Customer Impacts No more Direct and Indirect EP designations All ESC now 60-day time frame Consolidated Evidence of Standards Compliance (ESC) into one time frame No more Measures of Success (MOS) See it / Cite it No more A or C categories Engineering Department 2017- 14 © Copyright, The Joint Commission No more Opportunities for Improvement (OFIs) © Copyright, The Joint Commission Post-Survey Actions “After a survey event, organizations have the opportunity to submit clarifying ESC if they believe that their organization was in compliance with a particular standard at the time of survey.” ACC-59 Engineering Department 2017- 16 © Copyright, The Joint Commission What is Clarification? Clarification Eligible Observations made in error Engineering Department 2017- 17 © Copyright, The Joint Commission Ineligible Required documentation; i.e. “D” icons SAFER placement Evidence of Standards Compliance (ESC) ESC due within 60 days 45 day ESC still applicable for organizations with a PDA decision All observations will require an ESC OFI section of the report no longer applicable fields Engineering Department 2017- 18 © Copyright, The Joint Commission Findings of higher risk will require 2 additional ESC Engineering Department 2017- 19 © Copyright, The Joint Commission Prioritized Follow-up Action Challenging Standards John Maurer, SASHE, CHFM, CHSP Engineering Department The Joint Commission Engineering Department 2017- 20 © Copyright, The Joint Commission Most Cited Observations EC.02.06.01 2015 % Noncompliance 62% 2016 % Noncompliance 68% 2016 Rank 1 IC.02.02.01 EC.02.05.01 LS.02.01.35 LS.02.01.30 59% 58% 46% 50% 60% 57% 49% 51% 2 3 4 5 LS.02.01.20 LS.02.01.10 EC.02.02.01 51% 45% 39% 46% 50% 48% 6 7 8 PC.02.01.03 RC.01.01.01 40% 47% 47% 42% 9 10 Standard Engineering Department 2017- 21 © Copyright, The Joint Commission Most Cited Standards EC.02.06.01 EP 1 Interior spaces meet the needs of the patient population and are safe and suitable to the care, treatment and services provided. 2017 Scoring at EC.02.05.09 EP 6 NEW! Storage – Secured, labeled, etc. Segregation – Full vs. Empty NFPA 99 – 2012 • Chapter 11 – Gas Equipment • Chapter 5 – Gas and Vacuum Systems Engineering Department 2017- 22 © Copyright, The Joint Commission Cylinder management EC.02.06.01 EP 1 Interior spaces meet the needs of the patient population and are safe and suitable to the care, treatment and services provided. 2017 Scoring at EC.02.05.09 EP 7 NEW! Previously scored at EC.02.01.01 EP 5 Secured Protected for the elements (sun, snow, water, etc.) Protective shipping mesh or wraps NFPA 99 – 2012 • Chapter 5 – Gas and Vacuum Systems • Chapter 11 – Gas Equipment Engineering Department 2017- 23 © Copyright, The Joint Commission Outside Cylinder Management EC.02.06.01 EP 1 Interior spaces meet the needs of the patient population and are safe and suitable to the care, treatment and services provided. Relocatable Power Taps (Power Strips) 2017 Scoring at EC.02.04.03 EP 14 if in patient care area NEW! EC.02.06.01 EP 1 if non-patient care Engineering Department 2017- 24 © Copyright, The Joint Commission NFPA 99 – 2012 Relocatable Power Taps RPTs may be used for non-patient care equipment such ensuring they are never “daisy-chained” preventing cords from becoming tripping hazards installing internal ground fault and over-current protection devices using power strips that are adequate for the number and types of devices used Engineering Department 2017- 25 © Copyright, The Joint Commission as computers/monitors/printers, and in areas such as waiting rooms, offices, nurse stations, support areas, corridors, etc. Precautions needed if RPTs are used include: Definitions From NFPA 99-2012 patient sleeping bed, or the bed or procedure table of a critical care area Patient-care-related electrical equipment is defined in section 3.3.137 as electrical equipment that is intended to be used for diagnostic, therapeutic, or monitoring purposes in the patient care vicinity Patient care room is defined in section 3.3.138 as any room of a health care facility wherein patients are intended to be examined or treated. Note that this term replaces the term “patient care area” used in the 1999 NFPA 99, but the definition has not changed Patient care vicinity is defined in section 3.3.139 as a space, within a location intended for the examination and treatment of patients (i.e., patient care room) extending 6 ft. beyond the normal location of the bed, chair, table, treadmill, or other device that supports the patient during examination and treatment and extends vertically 7 ft. 6 in. above the floor Engineering Department 2017- 26 © Copyright, The Joint Commission Patient bed location is defined in section 3.3.136 as the location of a RPT Requirements Power strips may be used in a patient care vicinity to power The receptacles are permanently attached to the equipment assembly The sum of the ampacity of all appliances connected to the receptacles shall not exceed 75 percent of the ampacity of the flexible cord supplying the receptacles The ampacity of the flexible cord is suitable in accordance with the current edition of NFPA 70, National Electric Code. The electrical and mechanical integrity of the assembly is regularly verified and documented through an ongoing maintenance program Means are employed to ensure that additional devices or nonmedical equipment cannot be connected to the multiple outlet extension cord after leakage currents have been verifiedEngineering as safe Department 2017- 27 © Copyright, The Joint Commission rack-, table-, pedestal-or cart-mounted patient care-related electrical equipment assemblies, provided all of the following conditions are met, as required by section 10.2.3.6: RPT Requirements Patient bed locations in new health care facilities, or in existing facilities that undergo renovation or a change in occupancy, shall be provided with the minimum number of receptacles as required by section 6.3.2.2.6.2 pedestal-, or cart-mounted patient care-related electrical equipment assemblies are not required to be an integral component of manufacturer tested equipment. Power strips may be permanently attached to mounted equipment assemblies by personnel who are qualified to ensure compliance with section 10.2.3.6 Engineering Department 2017- 28 © Copyright, The Joint Commission Power strips providing power to rack-, table-, RPT Requirements power non-patient care-related electrical equipment (e.g., personal electronics) Power strips may be used outside of the patient care vicinity for both patient care-related electrical equipment & non-patient-care-related electrical equipment Power strips providing power to patient care-related electrical equipment must be Special-Purpose Relocatable Power Taps (SPRPT) listed as UL 1363A or UL 60601-1 Power strips providing power to non- patient-care-related electrical equipment must be Relocatable Power Taps (RPT) listed as UL 1363 Engineering Department 2017- 29 © Copyright, The Joint Commission Power strips may not be used in a patient care vicinity to EC.02.06.01 EP 1 Interior spaces meet the needs of the patient population and are safe and suitable to the care, treatment and services provided. Ligature/self harm risks (i.e. BHC) Current Risk Assessment Best Practice Guidelines • Design Guide for the Built Environment of Behavioral Health Facilities Engineering Department 2017- 30 © Copyright, The Joint Commission Ligature Risks – Psychiatric Settings See also Joint Commission Online, March 1, 2017 www.jointcommission.org/issues Engineering Department 2017- 31 © Copyright, The Joint Commission Process: self-harm risks identified Determination if previously identified Evaluate existing plans for removing the risks Evaluate the environmental risk assessment process Ligature Risks – Psychiatric Settings See also Joint Commission Online, March 1, 2017 www.jointcommission.org/issues Engineering Department 2017- 32 © Copyright, The Joint Commission Further evaluation Plans and policies on mitigation of harm posed by risks while removal occurs Adequacy of staffing patterns to the mitigation plans The patient suicide risk assessment process Ligature Risks – Psychiatric Settings The history of patient safety events and the process for root cause analysis of these events The organization’s process for monitoring its compliance with its policies Actions taken when noncompliance was identified Engineering Department 2017- 33 © Copyright, The Joint Commission Further evaluation Policies and practices related to actions needed for patients identified at risk Policies and processes of ensuring staff awareness of a patient’s level of risk The organization’s internal processes for improvement, including: IMPACT OF CMS ADOPTION OF THE Engineering Department 2017- 34 © Copyright, The Joint Commission 2012 LIFE SAFETY CODE (NFPA 101-2012) 2012 HEALTH CARE FACILITIES (NFPA 99-2012) Standards – NFPA 101-2012 The NFPA created a series of codes to provide guidance in building and maintaining buildings CMS adopted this body of codes, incorporating them into their COP as K-Tags The Joint Commission has also recognized the NFPA body of codes The Life Safety Chapter is based on NFPA 101-2012 In the Environment of Care several other NFPA • NFPA 10-2010, Standard for Portable Fire Extinguishers • NFPA 25-2011, Standard for Water-based Systems ITM Activity • NFPA 72-2010, Fire Alarm Code • NFPA 99-2012, Health Care Facilities Code Engineering Department 2017- 35 © Copyright, The Joint Commission codes are referenced, including: © Copyright, The Joint Commission Engineering Department 2017- 36 New vs. Existing Occupancies Existing Health Care Buildings, additions, renovations or changes in occupancy whose final plans were approved by the local Authority Having Jurisdiction (AHJ) prior to July 5th, 2016 Use Chapter 19 of the NFPA 101-2012 Life Safety Code® Engineering Department 2017- 37 © Copyright, The Joint Commission New Health Care Buildings, additions, renovations or changes in occupancy whose final plans were approved by the local AHJ after July 5th, 2016 Use Chapter 18 of the NFPA 101-2012 Life Safety Code® CMS Information Tuesday May, 3, 2016 CMS issued the final rule adopting the 2012 Life Safety Code®. The rule is effective July 5, 2016 This rule also adopts most of NFPA 99, 2012 edition. Chapters 7, 8, 12, 13 are excluded from the adoption Survey for compliance November 1, 2016 Emergency Management Published September 8, 2016 Implementation by November 15, 2017 Standards under review Engineering Department 2017- 38 © Copyright, The Joint Commission NFPA 99-2012: Risk-based Chapter 4: Building systems shall be designed to meet Category 1-4 Category 1: Failure likely to cause major injury of death Category 2: Failure likely to cause minor injury Category 3: Failure to cause discomfort Category 4: Failure with no impact to care Risk assessment Categories determined by organization’s risk assessment procedure Chapters identify new vs. existing application Engineering Department 2017- 39 © Copyright, The Joint Commission NFPA 99-2012 Adoption Exclusions Chapter 7: IT and Communication Systems Chapter 8: Plumbing Chapter 12: Emergency Management Engineering Department 2017- 40 © Copyright, The Joint Commission Chapter 13: Security Management CMS statement: “As stated in the proposed rule, we will not be adopting Chapters 7, 8 and 13 because we have no authority to regulate these specific topics in health care facilities. Additionally, the content of Chapter 12, Emergency management, is already being addressed in a separate rule for emergency preparedness. Although, we have not adopted these chapters, providers may use these chapters for their individual facility needs.” Source: Federal Register, Vol. 81, No. 86 Engineering Department 2017- 41 © Copyright, The Joint Commission NFPA 99-2012 Adoption Exclusions CMS Adoption Issues Roller latches continue to be prohibited Corridor doors Doors protecting hazardous areas ASC that renders one or more incapable continue to be AHC Outpatient surgical departments provisions of the Life Safety Code for unreasonable hardship Hospitals may install ABHR provided the installation adequately protects against inappropriate access Engineering Department 2017- 42 © Copyright, The Joint Commission There is a provision to allow CMS to waive specific While CMS does not directly enforce the Americans with Disabilities Act (ADA) it does expect compliance with the requirements as additional Federal requirements that facilities are required to follow. An example of this is corridor projections where the Life Safety Code (LSC) allows a noncontinuous projection to be no more than 6 inches from the corridor wall. Section 307 of the ADA Accessibility Guidelines for Buildings and Facilities” requires that projections be not more than 4 inches from the corridor wall. Facilities are required to meet this more stringent requirement as set forth by the ADA. Engineering Department 2017- 43 © Copyright, The Joint Commission CMS Quote: CMS Adoption Issues If the sprinkler system is shut down for 10 or more hours, a fire watch or evacuation of the building or affected portion of the building must occur Every sleeping room has outside door or window Windows in atrium walls are considered outside windows Exception: newborn nurseries and rooms intended for less than 24hour stays (see NFPA 101-2006 18/19.3.8) higher than 36 inches above the floor (with exceptions, see NFPA 101-2006 18/19.3.8.2) Required sprinkler protection of all high rises (>75 ft) Includes Chapter 43, Building Rehabilitation Engineering Department 2017- 44 © Copyright, The Joint Commission In new buildings the fixed window sill height is to be no Impact to Standards [Estimated for 2017] Environment of Care 149 – 1 = 148 + 13 = 161 31 modifications 203 – 5 = 198 +21 = 219 32 modifications Engineering Department 2017- 45 © Copyright, The Joint Commission Life Safety Chapter 2017 © Copyright, The Joint Commission Environment of Care Chapter EC.02.02.01 EP 9 The hospital minimizes risks associated with Note: Hazardous gases and vapors include, but are not limited to, ethylene oxide and nitrous oxide gases; vapors generated by glutaraldehyde; cauterizing equipment, such as lasers; waste anesthetic gas disposal (WAGD); and laboratory rooftop exhaust. (For full text, refer to NFPA 992012: 9.3.8; 9.3.9) Engineering Department 2017- 47 © Copyright, The Joint Commission selecting, handling, storing, transporting, using, and disposing of hazardous gases and vapors. EC.02.03.05 EP 25 The hospital has written documentation of annual inspection and testing of door assemblies by individuals who can demonstrate knowledge and understanding of the operating components of the door being tested. Testing begins with a pre-test visual inspection; testing includes both sides of the opening. Engineering Department 2017- 48 © Copyright, The Joint Commission Note: For additional guidance on testing of door assemblies, see NFPA 101-2012: 7.2.1.5.10.1; 7.2.1.5.11; NFPA 80-2010: 4.8.4; 5.2.1; 5.2.3; 5.2.4; 5.2.6; 5.2.7; 6.3.1.7; NFPA 105-2010: 5.2.1. EC.02.03.05 EP 25 When the door rating of a higher rating than required in an opening May be modified provided they continue to meet the requirements of the barrier Barrier and door information is documented on the Life Safety Drawings Label may remain if the door was not modified (i.e. hardware intact). If the organization chose to remove the hardware, the label should also be removed as the door no longer meets original design. If the door was intact but in a lesser barrier (i.e. 90 minute door in a 30 minute barrier), the label could remain as part of the original assembly. Engineering Department 2017- 49 © Copyright, The Joint Commission EC.02.05.01 EP 8 The hospital labels utility system controls Note 1: Examples of utility system controls that should be labeled are utility source valves, utility system main switches and valves, and individual circuits in an electrical distribution panel. Engineering Department 2017- 50 © Copyright, The Joint Commission to facilitate partial or complete emergency shutdowns. Note 2: For example, the fire alarm system’s circuit is clearly labeled as Fire Alarm Circuit; the disconnect method (that is, the circuit breaker) is marked in red; and access is restricted to authorized personnel. Information regarding the dedicated branch circuit for the fire alarm panel is located in the control unit. For additional guidance, see NFPA 101-2012: 18/19.3.4.1; 9.6.1.3; NFPA 72-2010: 10.5.5.2. Engineering Department 2017- 51 © Copyright, The Joint Commission EC.02.05.01 EP 8 (cont.) EC.02.05.01 EP 18 Medical gas storage rooms and transfer and manifold rooms comply with NFPA 992012: 9.3.7. Ventilation Engineering Department 2017- 52 © Copyright, The Joint Commission EC.02.05.01 EP 19 equipment and environment are maintained per manufacturers’ recommendations, including ambient temperature of at least 40°F; ventilation supply and exhaust; and water jacket temperature (when required). (For full text, refer to NFPA 99-2012: 9.3.10) Engineering Department 2017- 53 © Copyright, The Joint Commission The emergency power supply system’s EC.02.05.03 EP 10 seconds for the following: Emergency lighting at emergency generator locations. The hospital’s emergency power system (EPS) has a remote manual stop station (with identifying label) to prevent inadvertent or unintentional operation. A remote annunciator (powered by storage battery) is located outside the EPS location. Note: For guidance in establishing a reliable emergency power system (that is, an essential electrical distribution system), refer to NFPA 99-2012: 6.4.1.1.6; 6.4.1.1.17; 6.4.2.2.3.3; NFPA 110-2010: 5.6.5.6; 7.3.1. Engineering Department 2017- 54 © Copyright, The Joint Commission The hospital provides emergency power within 10 EC.02.06.05 EP 2 When planning for demolition, construction, Note: See LS.01.02.01 for information on fire safety procedures to implement during construction or renovation. Engineering Department 2017- 55 © Copyright, The Joint Commission renovation, or general maintenance, the hospital conducts a preconstruction risk assessment for air quality requirements, infection control, utility requirements, noise, vibration, and other hazards that affect care, treatment, and services. EC.02.05.05 EP 1 When performing repairs or maintenance Engineering Department 2017- 56 © Copyright, The Joint Commission activities, the hospital has a process to manage risks associated with air-quality requirements; infection control; utility requirements; noise, odor, dust, vibration; and other hazards that affect care, treatment, or services for patients, staff, and visitors. Medical Equipment & Utilities Systems All scheduled maintenance activities for Engineering Department 2017- 57 © Copyright, The Joint Commission non-high-risk medical equipment and utility systems components in an alternative equipment maintenance (AEM) program inventory are to be completed at 100%. AEM frequency is determined by the organization AEM program. Medical Equipment Note 3 Update …Scheduled maintenance activities for non-high-risk medical equipment in an alternative equipment maintenance (AEM) program may be deferred … provided the completion rate is not less than 90% for AEM for non-high-risk medical equipment. CMS indicated that 100% of the maintenance has to be completed and that AEM is performed at a frequency defined by the organization’s AEM program Engineering Department 2017- 58 © Copyright, The Joint Commission CMS response: Note allows for completion rate of 90% © Copyright, The Joint Commission Life Safety Chapter 2017 LS.01.01.01 EP 2 In time frames defined by the hospital, the hospital performs a building assessment to determine compliance with the Life Safety chapter. Requires documentation of the policy Policy requires time frame Policy on how an assessment is completed Does not include review of results of assessment Engineering Department 2017- 60 © Copyright, The Joint Commission The hospital maintains current and accurate drawings denoting features of fire safety and related square footage. Fire safety features include the following: Areas of the building that are fully sprinklered (if the building is partially sprinklered) Locations of all hazardous storage areas Locations of all fire-rated barriers Locations of all smoke-rated barriers Sleeping and non-sleeping suite boundaries, including the size of the identified suites Locations of designated smoke compartments Locations of chutes and shafts Any approved equivalencies or waivers Engineering Department 2017- 61 © Copyright, The Joint Commission LS.01.01.01 EP 3 When the hospital plans to resolve a deficiency through a Survey-Related Plan for Improvement (SPFI), the hospital meets the 60-day time frame. Note 1: If the corrective action will exceed the 60-day time frame, the hospital must request a time-limited waiver within 30 days from the end of survey. Note 2: If there are alternative systems, methods, or devices considered equivalent, the hospital may submit an equivalency request using its Statement of Conditions (SOC). Note 3: For hospitals that use Joint Commission accreditation for deemed status purposes: if there are existing alternative systems, methods, or devices, the hospital may submit a waiver request using their Statement of Conditions (SOC). Note 4: For additional guidance on equivalencies, see NFPA 2012: 101:1.4.3 Engineering Department 2017- 62 © Copyright, The Joint Commission LS.01.01.01 EP 4 EP 5 For hospitals that use Joint Commission accreditation for deemed status purposes: The hospital maintains documentation of any inspections and approvals made by state or local fire control agencies. EP 6 The hospital does not remove or minimize an existing life safety feature when such feature is a requirement for new construction. Existing life safety features, if not required by the Life Safety Code, can be either maintained or removed. (For full text, refer to NFPA 101-2012: 4.6.12.2; 4.6.12.3) Engineering Department 2017- 63 © Copyright, The Joint Commission LS.01.01.01 EP 5 & 6 LS.02.01.34 EP 3 EP 3 The ceiling membrane is installed and Engineering Department 2017- 64 © Copyright, The Joint Commission maintained in a manner that permits activation of the smoke detection system. (For full text, refer to NFPA 101-2012: 18/19.3.4.1) LS.02.01.35 EP 5 also free from corrosion, foreign materials, and paint and have necessary escutcheon plates installed. (For full text, refer to NFPA 101-2012: 18.3.5.1; 19.3.5.3; 9.7.5; NFPA 25-2011: 5.2.1.1.1; 5.2.1.1.2; NFPA 13-2010: 6.2.6.2.2; 6.2.7.1) Engineering Department 2017- 65 © Copyright, The Joint Commission Sprinkler heads are not damaged. They are LS.02.01.35 EP 10 portable fire extinguisher is 75 feet or less. Portable fire extinguishers have appropriate signage, are installed either in a cabinet or secured on a hanger made for the extinguisher, and are at least four inches off the floor. Those fire extinguishers that are 40 pounds or less are installed so the top is not more than 5 feet above the floor. (For full text, refer to NFPA 101-2012: 18/19.3.5.12; 9.7.4.1; NFPA 102010: 6.2.1.1; 6.1.3.3.1; 6.1.3.4; 6.1.3.8) Engineering Department 2017- 66 © Copyright, The Joint Commission The travel distance from any point to the nearest LS.02.01.70 EP 1 compartment where flammable liquids, combustible gases, or oxygen is used or stored; these areas have signs that read “NO SMOKING” or display the international symbol for no smoking. In facilities where smoking is prohibited and signs are prominently placed at all major entrances, secondary signs that prohibit smoking in hazardous areas are not required. (For full text, refer to NFPA 101-2012: 18/19.7.4) Note: The secondary sign exception is not applicable to medical gas storage areas. Engineering Department 2017- 67 © Copyright, The Joint Commission Smoking is prohibited in any room, ward, or LS.02.01.70 EP 2 ashtrays are safely designed and made of noncombustible material. Metal containers with self-closing cover devices in which ashtrays can be emptied are readily available to all areas where smoking is permitted. (For full text, refer to NFPA 1012012: 18/19.7.4) Engineering Department 2017- 68 © Copyright, The Joint Commission In areas where smoking is permitted, Department of Engineering 630-792-5900 George Mills, MBA, FASHE, CEM, CHFM, CHSP, Green Belt Director Andrea Browne, PhD., DABR John Maurer, CHFM, CHSP, SASHE Medical Physicist Engineer Engineer James Woodson, P.E., CHFM Engineer Kathy Tolomeo, CHEM, CHSP Engineer Kate Dolezal, MA, CRC, LPC Technical Coordinator Engineering Department 2017- 69 © Copyright, The Joint Commission Herman McKenzie, MBA, CHSP The Joint Commission Disclaimer The Joint Commission reserves the right to change the content of the information, as appropriate These slides are only meant to be cue points, which were expounded upon verbally by the original presenter and are not meant to be comprehensive statements of standards interpretation or represent all the content of the presentation. Thus, care should be exercised in interpreting Joint Commission requirements based solely on the content of these slides These slides are copyrighted and may not be further used, shared or distributed without permission of the original presenter or The Joint Commission Engineering Department 2017- 70 © Copyright, The Joint Commission These slides are current as of 3/24/2016.