Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
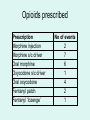
Audit Opioid use in palliative patients on general hospital wards Dr Helen Mitchell Hospital Palliative Care Team Cardiff and Vale University LHB Background • Strong opioids commonly used on general wards – – – – – – Acute pain Post-op pain Vascular insufficiency Cardiac chest pain Breathlessness Cancer Controlled drug prescribing • Guidance – Junior doctor ‘pocket guides’ – BNF – Anaesthetic department guidelines – Hospital formularies – Palliative textbooks / web pages – Palliative care teaching • Legal requirements Controlled drug regulation • Medicines Ethics and Practice: A guide for pharmacists and pharmacy technicians Royal Pharmaceutical Society of Great Britain 2009 • Safer Management of Controlled Drugs: A guide to good practice in secondary care (England) Department of Health 2007 • Standards for Medicines Management Nursing Midwifery Council 2008 Why this study? • Clinical incident occurred • Incorrect dose of Sevredol was administered • Other instances? Aim • Review prescriptions for strong opioids for patients known to the hospital palliative care team and note any discrepancies Setting standards • All prescription/administration of controlled drugs should conform to: – Legal requirements – EAPC guidance on use of morphine and alternative opioids (2001) – locally accepted ‘good practice’ Study design • Prospective review of hospital prescription charts - patients known to Hospital Palliative Care Team at Llandough Hospital and University Hospital of Wales • 3 month period • Data recording sheet completed by HPCT member if ‘incident’ noted • Issue discussed with relevant ward staff and action / outcome recorded Results • 23 events – UHW 20 – Llandough 3 • Malignancy 18 – Surgical 7 – Medical 6 – Haem 5 • Medical 12 – Haematology 5 • Surgical 11 – General surgery 9 – Head & neck 1 – Orthopaedics 1 • Non malignancy 5 – Surgical 4 – Medical 1 Opioids prescribed Prescription Morphine injection Morphine s/c driver Oral morphine Oxycodone s/c driver Oral oxycodone Fentanyl patch Fentanyl ‘lozenge’ No of events 2 7 6 1 4 2 1 Types of problems identified Event relating to: Medical Surgical Regular dose 4 3 PRN dose 4 3 Co-analgesics 1 2 Omitted dose 2 1 Supply 1 Documentation 1 Other 1 Problems with regular opioid prescriptions Related to: Administration Prescribing 4 6 Administration - regular opioids • • • • • 10 pm dose withheld; ‘patient too drowsy’ 4 hourly dose withheld; ‘patient confused’ 10 pm dose not signed for Fentanyl patch removed but not replaced Patient self-administered syringe driver medication due to severe pain • Syringe driver not set up because of incompatible drug volume Prescribing - regular opioids • Usual dose stopped; ‘patient unwell’ • Usual dose not charted on admission; ‘patient vomiting’ • Syringe driver dose incorrectly prescribed for 48 hours • Incorrect switch from oral to syringe driver (opioid toxicity) • Incorrect switch from syringe driver to oral Problems with ‘PRN’ opioids • Administration 4 • Prescribing 2 Administration - PRN doses • Prescribed dose not given accurately – more or less? • Patient incorrectly advised of PRN dose on discharge (‘Take 2 tabs’ but stronger strength prescribed & dispensed) • Patient in pain but no PRN doses given Prescribing - PRN doses • Oral oxycodone changed to IM morphine • Concern that PRN dose used frequently, but ‘inappropriately’ low dose prescribed (morphine liquid 10 mg PRN with oral morphine equivalent 160 mg/24 hrs) Co-analgesics • Frequent combinations with strong opioids – Tramadol – Co-codamol Action taken • Each incident risk assessed • Discussion / education – Ward staff teaching – Clinical incident forms completed if indicated • Clinical governance issues addressed • Targeted education session by HPCT consultant to ward staff Future action • Ongoing education • Issues to address – Rationale of WHO analgesic ladder – Appropriate (and legal) PRN medication use – Opioid conversions – Assessing suspected opioid toxicity • Re-audit next year? Lessons learned • Safe use of opioids for palliative patients may prove difficult on general hospital wards • Despite available teaching and guidance, discrepancies and errors occur Lessons Learned • Need for vigilance from ‘expert’ teams • Need for ongoing education and support – doctors – nursing staff – pharmacists References • Hanks GW. Morphine and alternative opioids in cancer pain: the EAPC recommendations. Br J Cancer 2001; 84(5): 587-93 • Cardiff and Vale NHS Trust. Procedure for ordering, storage and safe administration of controlled drugs. Nov 2003. • The ‘How to Guide’ for Improving Medicines Management: Preventing Harm from High-Alert Medications in Secondary Care. www.1000livescampaign.wales.nhs.uk Thank you