Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
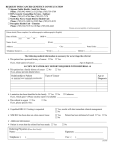
PATIENT HEALTH HISTORY Name: ________________________________ DOB:______________ Age: ______ Date: _______________ Referred by: _______________________________ Emergency Contact: _____________________________ Marital Status (please circle): Married Single Divorced Widowed Occupation: _________________________ Place of Employment: _________________________________ Problem today, if any ______________________________________________________________________ Medication allergies 1.____________________________________ 5.____________________________________ 2.____________________________________ 6.____________________________________ 3.____________________________________ 7.____________________________________ 4.____________________________________ 8.____________________________________ Current medications 1. ____________________________________ 5.____________________________________ 2. ____________________________________ 6.____________________________________ 3. ____________________________________ 7.____________________________________ 4. ____________________________________ 8.____________________________________ Other physicians you see and their specialty: 1. ________________________________________________________________________ 2. ________________________________________________________________________ 3. ________________________________________________________________________ Date of last: Mammogram: _________________________________ Bone density test: _____________________ Colonoscopy:__________________________________ History of Abnormal Pap (please circle) Y N History of Abnormal Mammogram (please circle) Y N First day of last menstrual cycle:________________________________ Number of pregnancies:___________________ How many children do you have:___________________ Smoking History (please circle): Current smoker Never smoked (additional questions on reverse) Past smoker Past surgeries: 1.___________________________________________________________ 2.___________________________________________________________ 3.___________________________________________________________ 4.___________________________________________________________ 5.___________________________________________________________ MRSA QUESTIONS 1. Have you had any open sores, wounds, spider bites or boils in the past year? ___Yes ___No 2. Have you ever been treated for MRSA or a staph infection? ___Yes ___No 3. Have you received antibiotics in the last year for a skin or wound infection? ___Yes ___No FAMILY HISTORY Please circle Y to those that apply to YOU and/or YOUR FAMILY, on both your mother’s and father’s side. Next to each statement, please list the relationship to you of the individual diagnosed and their age at diagnosis. RELATIONSHIP AGE AT DIAGNOSIS BREAST AND OVARIAN CANCER Y N Personal Breast Cancer before age 50 ____________ _______________ Y N Ovarian Cancer ____________ _______________ Y N Male breast cancer ____________ _______________ Y N 2 or more breast or ovarian cancers ____________ _______________ Y N Ashkenazi Jewish ancestry & personal Or family history of breast or ovarian cancer ____________ _______________ COLON AND UTERINE CANCER Y N Personal Uterine cancer before age 50 ____________ _______________ Y N Personal Colorectal cancer before age 50 ____________ _______________ Y N 2 or more uterine or colorectal cancers ____________ _______________ Signed _____________________________________________ Date _________________