Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
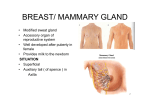
n Case Report Quadrilateral Space Syndrome With Involvement of the Tendon of the Latissimus Dorsi Ryuji Koga, MD; Kozo Furushima, PhD; Hiroshi Kusano, MD; Junichiro Hamada, PhD; Yoshiyasu Itoh, PhD abstract Quadrilateral space syndrome (QSS) is the term used to describe axillary nerve palsy due to compression of the axillary nerve and posterior circumflex artery in the quadrilateral space. The precise pathophysiology of QSS is still unclear; hence, a consensus of diagnosis and treatment for QSS has not yet been achieved. The authors present the case of a 17-year-old male baseball player with symptoms of QSS, including right elbow and shoulder joint pain and upper limb numbness while throwing. The symptoms had worsened during baseball. Conservative management for 3 months failed to resolve the symptoms, so surgery was performed. Axillary nerve decompression resulted in functional improvement. The cause of QSS has been previously reported to be fibrous bands, the long head of the triceps, and Bennett lesions. However, the cause of QSS in this case was compression of the axillary nerve between the proximal humerus and the tendinous attachment of the latissimus dorsi. The authors incised a 10- to 15-mm segment of the medial edge of the tendinous insertion of the latissimus dorsi, which resulted in resolution of QSS symptoms. [Orthopedics. 201x; xx(x):xx-xx.] O riginally defined by Cahill and Palmer,1 quadrilateral space syndrome (QSS) is a rare clinical syndrome in which the axillary nerve and the posterior circumflex humeral artery are compressed in the quadrilateral space. Patients with QSS experience a variety of symptoms, which makes definitive diagnosis difficult. Moreover, no clear surgical criteria have been established. The pathophysiology of QSS has been thought to be caused by fibrous bands, the long head of the triceps,2,3 and Bennett lesions of the shoulder. The current authors propose a new pathophysiology of QSS caused by axillary nerve compression by the tendinous insertion of the latissimus dorsi. Case Report The authors’ institutional review board approved a patient registry, and the patient provided informed consent. A 17-yearold, right-hand–dominant boy presented with right elbow and shoulder joint pain MONTH/MONTH 201x | Volume xx • Number X and upper limb numbness while throwing. He was a pitcher for a high school baseball team, and the symptoms had prevented him from playing baseball effectively for several months. There was no history of trauma or surgery of the shoulder or elbow. Physical examination revealed tenderness over the quadrilateral space, especially at the anterior entrance of the quadrilateral space that is the medial edge of the insertion of the latissimus dorsi tendon. Sensory disturbances were localized in the axillary nerve region. The pain worsened when the arm was abducted and externally rotated. Physical examination did not suggest glenohumeral instability and internal impingement. Radiography showed no bony abnormalities. Magnetic resonance imaging of the elbow showed no ligamentous injury or osteochondritis dissecans. The patient was diagnosed with QSS. The authors initially treated The authors are from Keiyu Orthopaedic Hospital (RK, KF, HK, YI), Gunma, and Kuwano Kyoritsu Hospital (JH), Koriyama, Japan. The authors have no relevant financial relationships to disclose. Correspondence should be addressed to: Ryuji Koga, MD, Keiyu Orthopaedic Hospital, 1741 Hanetsuku Tatebayashi, Gunma 374-0011, Japan ([email protected]). Received: September 1, 2016; Accepted: December 12, 2016. doi: 10.3928/01477447-20170117-06 1 n Case Report Figure 1: Intraoperative photograph of the lateral aspect of the axillary region. A 4-cm transverse incision was made at the lateral margin of the axilla over the neck of the humerus (black line: skin incision site). Figure 3: Schematic drawing showing the axillary nerve (AN) entrapped by the tendon of the latissimus dorsi (LD) against the humerus. The incision of 10 to 15 mm of the medial edge of the tendon successfully decompressed the nerve (red line: resection line). the patient conservatively with medication (mecobalamin) and physical therapy (stretching of the glenohumeral joint and muscle strengthening around the scapula); however, there was no improvement for 3 months. Hence, surgery was conducted. Surgery was performed under general anesthesia, with the patient in the lateral decubitus position using the SPIDER2 Limb Positioner (Smith & Nephew, Bridgeville, Pennsylvania) to bring the upper limb into “zero” position. The authors performed axillary nerve decompression through the lateral margin of the axilla. A 4-cm transverse incision was made over the lateral margin of the axilla (Figure 1). The authors confirmed that abduction and 2 Figure 2: Intraoperative photograph of the pseudoneuroma of the axillary nerve (AN). Abbreviation: LD, latissimus dorsi. external rotation of the upper arm tightly compressed the axillary nerve between the proximal humerus and the tendon of the latissimus dorsi. The axillary nerve was released through a 10- to 15-mm incision along the medial edge of the latissimus dorsi tendon insertion. There was a pseudoneuroma of the axillary nerve (Figure 2). Surgery completely relieved the QSS symptoms, and the patient had an uneventful recovery. The patient was allowed to throw a ball as hard as possible at 1 month postoperatively. He successfully returned to competitive baseball as a pitcher 3 months postoperatively. Discussion Quadrilateral space syndrome is an uncommon syndrome that is characterized by vague symptoms; consequently, clinical diagnostic criteria are lacking. Additionally, the sensitivity of imaging findings is unclear. Atrophy or abnormal signal around the teres minor muscle on magnetic resonance imaging may suggest QSS; however, this finding is rare, with an incidence rate of 0.8%.4 Occlusion of the posterior circumflex humeral artery on abduction and external rotation of the arm shown with subclavian angiography is reportedly useful in QSS diagnosis.5,6 In the current case, the diagnosis of QSS was supported by clinical signs such as tenderness over the anterior entrance of the quadrilateral space, sensory disturbances in the deltoid region innervated by the axillary nerve, and an increase in shoulder or elbow pain when the patient’s arm was abducted and externally rotated. The authors confirmed that the axillary nerve compression was caused by the tendinous attachment of the latissimus dorsi, and the entrapment was firm during abduction and external rotation of the arm. Therefore, incision of a 10- to 15-mm segment of the medial edge of the tendinous insertion of the latissimus dorsi released the axillary nerve and improved the QSS. Previous research has shown that the quadrilateral space can cause an entrapment syndrome that compresses the axillary nerve and the posterior circumflex humeral artery. Fibrous bands in the quadrilateral space are believed to be the cause of nerve and artery compression in most patients with QSS.1,7 The most common site for fibrous band development is between the teres major and the long head of the triceps.7 However, the pathogenesis of QSS in the current case was axillary nerve compression caused by the tendinous attachment of the latissimus dorsi. The current authors expanded the quadrilateral space using the posterior approach8 but found no obvious entrapment site or fibrous bands as previously reported.1,8 In fact, a large amount of muscle tissue at the attachment of the teres major was found. The firm entrapment that causes neurovascular compression was not found in this area. One of the authors (Y.I.) determined that the mechanism of axillary nerve compression was the rolling up of the latissimus dorsi tendon when the humerus was in an abducted and externally rotated position, based on previous reports of latissimus dorsi muscle transfer with the neurovascular pedicle for reconstructions of the paralyzed shoulder and elbow.9,10 The current authors detected the typical pseudoneuroma of the axillary nerve (Figure 2), which confirmed the entrapment on visual inspection. The QSS was due to the entrapment of the axillary nerve by the tendon of the latissimus dorsi while the shoulder was abducted and externally Copyright © SLACK Incorporated n Case Report rotated (Figure 3). This arm position is necessary for throwing. The authors believe that repetitive overhead arm motions caused the pseudoneuroma of the axillary nerve to develop. To completely understand the pathology of QSS, further study, including anatomic or clinical research, may be necessary. Conclusion To the authors’ knowledge, this is the first report of QSS caused by entrapment of the axillary nerve between the insertion of the tendon of the latissimus dorsi and the proximal humerus, exacerbated by an abducted and externally rotated arm position. The incision of 10 to 15 mm of the medial edge of the tendon of the latis- simus dorsi decompressed the nerve and relieved the patient’s symptoms. References 1. Cahill BR, Palmer RE. Quadrilateral space syndrome. J Hand Surg Am. 1983; 8(1):65-69. 2. Brown SA, Doolittle DA, Bohanon CJ, et al. Quadrilateral space syndrome: the Mayo Clinic experience with a new classification system and case series. Mayo Clin Proc. 2015; 90(3):382-394. 3. McClelland D, Hoy G. A case of quadrilateral space syndrome with involvement of the long head of the triceps. Am J Sports Med. 2008; 36(8):1615-1617. 4. Cothran RL Jr, Helms C. Quadrilateral space syndrome: incidence of imaging findings in a population referred for MRI of the shoulder. AJR Am J Roentgenol. 2005; 184(3):989-992. 5. Okino S, Miyaji H, Matoba M. The quadrilateral space syndrome. Neuroradiology. 1995; MONTH/MONTH 201x | Volume xx • Number X 37(4):311-312. 6. Redler MR, Ruland LJ III, McCue FC III. Quadrilateral space syndrome in a throwing athlete. Am J Sports Med. 1986; 14(6):511513. 7.McClelland D, Paxinos A. The anatomy of the quadrilateral space with reference to quadrilateral space syndrome. J Shoulder Elbow Surg. 2008; 17(1):162-164. 8.McAdams TR, Dillingham MF. Surgical decompression of the quadrilateral space in overhead athletes. Am J Sports Med. 2008; 36(3):528-532. 9. Itoh Y, Horiuchi Y, Nemoto K, Uchinishi K. Latissimus dorsi transfer for restoration of active elbow flexion [in Japanese]. Kanto J Ortho Trauma. 1982; 13:445-449. 10. Itoh Y, Sasaki T, Ishiguro T, Uchinishi K, Yabe Y, Fukuda H. Transfer of latissimus dorsi to replace a paralysed anterior deltoid: a new technique using an inverted pedicled graft. J Bone Joint Surg Br. 1987; 69(4):647651. 3