Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
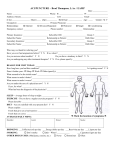
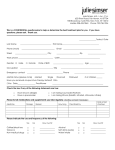
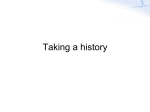
Healing Touch Acupuncture New Patient Intake & Financial Policy Form Date_________________ Name ___________________________ Date of Birth __________ Age _______ Address_____________________________________________________ City___________________ State ____________Zip____________ Home Phone ______________Work Phone _____________Cell___________ Email address_____________________ □M □ F Marital Status_________ Emergency Contact (Name & Number)____________________________ Employer__________________Occupation_____________Hours/wk______ Work Address_________________________________________________ Referred by?___________________May we thank them for the referral?_____ Primary Care Physician______________________Phone________________ Are you under a physician’s care now? □YES □NO Reason________________ Is this visit related to a work or motor vehicle injury? □YES □NO Injury Date____________ Have you had acupuncture before? □YES □NO Chinese Herbs? □YES □NO Insurance Information: (please fill out if you have acupuncture coverage) Insurance Co. Name________________________Policy #_______________ Insurance Co. Address___________________________________________ City ________________State ________________Zip____________ Phone_________________________________ Subscriber’s Name___________________ Relationship to Subscriber:_______ Address __________________________________Phone_______________ Subcriber’s Date of Birth ___________Policy #________Group # __________ Deductible Amount? __________Date Met? __________ Co-Pay Amount _____ Second Insurance Co. Name _________________Policy#_______________ Address __________________________________Phone_______________ I hereby assign to Chérri Gallison, LAc LPC any medical benefits for services rendered by her to which I am entitled. I authorize the release of any medical or other information necessary to process claims for those services. I understand I am responsible for any charges not covered by insurance. I agree to pay for services on the day received unless other arrangements are made. I understand that appointments missed or cancelled more than twice with less than 24 hours notice will incur full charges. I understand and agree to this financial policy: Signature _________________________________ Date _______________ 1 Medical History Form Date_________________ Name_______________________________ Reason for visit today?___________________________________________ How long have you had this condition?______________Is it getting worse?____ Does it bother your: □Sleep □Work □Other (what?)____________________ What was the initial cause?________________________________________ What makes it better?________________________________________ What makes it worse?________________________________________ Family Medical History: □Allergies □Cancer □Seizures □Arteriosclerosis □Diabetes □Stroke □Asthma □Alcoholism □Heart Disease □High Blood Pressure □Substance Abuse Is there anything else about your family history I should know?______________ Patient Health Information Ht.__________ Wt.__________ Blood Pressure_________ □Yes □No □No Do you have any reason to believe you are pregnant? Do you have any chronic infectious diseases? □Yes What prescription or over the counter medications do you take CURRENTLY? What vitamins/herbs/supplements do you take CURRENTLY? □ □ Do you have food or drug allergies or sensitivities? Yes No (Please List)______________________________________________ Your Medical History: (check if you had or currently have any of these conditions) □AIDS/HIV □Alcoholism □Allergies □Appendicitis □Epilepsy □Goiter □Gout □Heart Disease □Pleurisy □Major Traumas □Pneumonia (car, fall, etc. – list:) □Polio _______________ □Rheumatic Fever _______________ 2 □Arteriosclerosis□Hepatitis □Scarlet Fever □Tuberculosis □Asthma □Herpes □Stroke □Typhoid Fever □Birth Trauma □High Blood Pressure □Surgery (list) □Ulcers □Cancer □Measles ______________□Venereal Disease □Chicken Pox □Multiple Sclerosis ______________□Whooping Cough □Diabetes □Mumps ______________□Other (specify) □Emphysema □Pacemaker □Thyroid Disorders _______________ Your Diet & Lifestyle Issues: □Low □Normal □High □Coffee □Artificial Sweeteners □Soft Drinks □Sugar □Salty Foods Thirst for water? □Low □High Strongly like my water? □Cold □Hot □Tepid Appetite? Please describe your typical diet, including any foods that you do or do not eat: Do you feel this is a good diet for you? □Yes □No If No, in what ways would you like to change your diet?___________________ Do you use tobacco (what form/how much)?____________________________ Do you drink alcohol (what form/how much)?___________________________ Exercise (what form/how much)?____________________________________ Sleep Habits ___________________________________________ Are you sexually active? □Yes □No Method of contraception?__________________________________ What are the major stressors in your life?______________________________ What gives you pleasure?__________________________________________ Hobbies/Interests?_________________________________ Do you have a spiritual or faith practice (please explain) ?_________________ ____________________________________________________________ What emotions predominant in your life? ____________________________________________________________ Have you experienced any major traumas (please explain)? ____________________________________________________________ Is there anything else I should know about you? ___________________________________________________________ 3 Body System Review – Please check any areas of concern, whether current, past, or occasional. Current Past Occasional GENERAL: Current Past Occasional Feeling hot or cold Cold hands or feet Fatigue Low energy Anemia Slow wound healing Chronic infections Allergies Difficulty sleeping Unexplained fever Headaches Frequent colds Alcohol or substance abuse CARDIOVASCULAR: Heart disease Stroke Chest pain High blood pressure Low blood pressure Heart palpitations Irregular heartbeat Heart murmur Rheumatic fever Varicose veins Ankle swelling Water retention/edema MUSCULO-SKELETAL: Lower back pain Upper back pain Neck pain Shoulder pain Arm/wrist/hand pain Leg/foot pain Joint pain/stiffness Arthritis Muscle spasms/cramps RESPIRATORY: Shortness of breath Difficulty breathing Lung congestion Persistent cough Asthma/wheezing Chronic bronchitis Influenza Pneumonia Pleurisy Emphysema Tuberculosis NERVOUS SYSTEM; Numbness/tingling Paralysis/atrophy Dizziness/Vertigo Fainting Seizures/Epilepsy Tics Forgetfulness/Poor memory Depression Irritability Easily stress Anxiety/Nervousness Mood swings Abuse survivor Considered/attempted suicide Seeing a therapist GASTROINTESTIONAL: Poor appetite Excessive appetite Changes in appetite Weight gain or loss Excessive thirst Belching Gas/bloating Indigestion Acid regurgitation/heartburn Nausea/vomiting Abdominal cramps/pain Hemorrhoids Hiccups Bad breath Peculiar tastes Diarrhea ENDOCRINE: Hypo/hyper thyroid Low blood sugar Diabetes I or II Unusual day sweats Night sweats Current Past Occasional Current Past Occasional 4 Frequent stools Constipation Slow/infrequent stools Laxative use Undigested food in stool Mucous in stool Black or bloody stool Itchy or burning anus Colitis/Irritable bowel Intestinal pain or cramping Rectal pain Appendicitis Gall bladder problems Liver trouble EENT: Vision problems/changes Eye pain or strain Red, itchy eyes Floaters (spots) in vision Poor night vision Glaucoma Tearing/dryness Glasses/contacts Hearing problems Earaches/discharge Ear ringing/tinnitus Sinus problems Phlegm Nose bleeds Frequent sore throats Enlarged thyroid Hay fever Teeth grinding Jaw pain/clicking Dental problems Headaches Migraines Concussion SKIN & HAIR: Frequent bruising Itching Dryness Rashes Acne Eczema Psoriasis Herpes Hives Shingles Ulcerations Fungal infections Hair loss GENITO-URINARY: Freq. urinary tract infections Painful urination Excessive urination Changes in steam Leakage of urine Bed wetting Blood in urine Sexually transmitted disease Kidney stones Kidney disease MEN’S HEALTH: Sexual difficulties Prostate problems Testicular pain/swelling Discharge from penis Changes in sexual desire or function Fertility issues WOMEN’S HEALTH: PMS Menstrual irregularity Menstrual cramping Changes in menstrual cycle Bleeding between cycles Vaginal pain/infections Vaginal discharge Frequent yeast infections Pain with intercourse Breast pain/lumps Nipple discharge Menopause symptoms Hot flashes Menopause Changes in sexual desire or function Sexual difficulties Fertility issues 5