Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
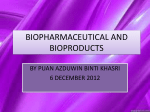
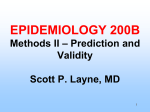
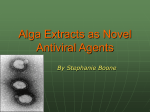
NDSSL Technical Report 10-042 March 29th, 2010 Title: Coevolution of Epidemics, Social Networks, and Individual Behavior: A Case Study Authors: Jiangzhuo Chen Achla Marathe Madhav V. Marathe Contact: Jiangzhuo Chen Email: [email protected] Tel.: +1 703 518 8032 Fax: +1 703 518 5376 To appear in: Acknowledgements: The 3rd International Conference on Social Computing, Behavioral Modeling, and Prediction (SBP10) March 30–31, 2010 We thank our external collaborators and members of the Network Dynamics and Simulation Science Laboratory (NDSSL) for their suggestions and comments. This work has been partially supported by NSF Nets Grant CNS-0626964, NSF HSD Grant SES-0729441, CDC Center of Excellence in Public Health Informatics Grant 2506055-01, NIH-NIGMS MIDAS project 5U01GM070694-05, NIH MIDAS project 2U01GM070694-07, NSF PetaApps Grant OCI-0904844, DTRA R&D Grant HDTRA1-09010017, DTRA CNIMS Grant HDTRA1-07-C-0113 and NSF NETS CNS0831633. Network Dynamics and Simulation Science Laboratory Virginia Bioinformatics Institute Virginia Polytechnic Institute and State University Abstract This research shows how a limited supply of antivirals can be distributed optimally between the clinics and the market so that the attack rate is minimized and enough revenue is generated to recover the cost of the antivirals. Results using an individual based model find that prevalence elastic demand behavior delays the epidemic and change in the social contact network induced by isolation reduces the peak of the epidemic significantly. A multi-theory methodology consisting of multi-layer social network modeling and multi-layer behavioral modeling is a major contribution of this work. In this paper we apply this methodology, combined with agent-based simulation, to analyze the fairness of the stockpile distribution, and the impact of contextual behavioral adaptation on the epidemic evolution. Key words: multiple theory, social network, epidemic, antiviral, behavioral modeling, agentbased simulation, microeconomic analysis 1 Introduction A severe epidemic presents a serious threat as it can affect the lives of millions of people and cost billions through morbidity and mortality. Successful pandemic preparedness demands full participation from the private sector and the public sector. Private sector knows which activities and personnel are most critical in their operations. The public sector needs to ensure that all critical infrastructures and resources stay operational and accessible. The roles and responsibilities of the private sector and the government need to be well coordinated and understood in order to construct effective intervention strategies. This research is motivated by our recent work as a part of a DHHS requested analysis undertaken by the NIH sponsored MIDAS program [9]. Recent expansion of antiviral drug production capacity and research based evidence of potential benefits of prophylactic antiviral drug has created a renewed interest in assessing the antiviral drug use strategies and potential stockpiling targets by the private and public sector [7]. The strategies for stockpiling antiviral drugs should ensure that sufficient quantities are available to support recommended interventions. The public sector stockpiles are expected to be available mostly for treatment purposes given the limited supply. Responsibility for purchasing antiviral drugs for prophylaxis will primarily be of the private sector and households [18, 22]. In the current H1N1 pandemic, a few countries have allowed antiviral drugs to circulate through markets, e.g., in India people can purchase Tamiflu if they have a prescription [1]. In this work we study the conditions for market distribution of antiviral drugs to become desirable. This research uses an economic perspective to study how disease prevalence, social contact networks and individual behavior co-evolve. A specific scenario is considered: given a limited stockpile of antivirals, is there an optimum antiviral allocation strategy between the market-based availability and public distribution via clinics that minimizes the attack rate and recovers the cost of antivirals through the market. An economic perspective for the evaluation of public health measures is important as it helps separate the effects of public health policies from those of private decision making. One of our major contributions is the study of the interaction between the prevalence of the disease, which is decreased by the demand for antivirals, and the demand for antiviral itself, which is increased by the extent of the disease. To our best knowledge this is the first study that uses individual based approach to analyze how behavioral changes occur in response to the growth of the disease and how these changes, in turn, affect the disease dynamics. The degree to which prevalence 1 induces demand for antiviral drugs determines the prevalence elasticity of demand for prevention against the disease. Note that prevalence elastic demand behavior is both good and bad. When the prevalence is high, the demand for prevention makes the disease self limiting. However, when the prevalence is low, the demand for prevention is low which makes it progressively harder to eradicate the disease. In fact, the prevalence elasticity of demand explains the oscillatory behavior of the disease prevalence [14, 15, 20]. This study aims to isolate the effects of changes in individual behavior caused by the fear of getting infected, and the effects of changes in the social contact network, on the spread of the disease. Our results show that prevalence elastic demand can delay the onset of the outbreak and changes in social network caused by isolation measures can reduce the peak of the epidemic curve by a significant amount. It also shows that allocating the entire stockpile of the antivirals to just the public sector or just the private sector is a sub-optimal strategy. Another contribution of this work is a multiple theory methodology. We develop an associated modeling environment, consisting of a dimension of social network models and a dimension of behavioral models, to study the coevolution of individual behavior, disease dynamics, and social networks. Finally, in this study we apply a novel microeconomic analysis methodology that combines behavioral economics [21] and agent-based simulation. We model each individual’s self intervention in an epidemic as economically motivated behavior and simulate how the behavior in an aggregated form affects the epidemic dynamics. The rest of the paper is organized as follows. We describe the infectious disease model, the contact network model, and various interventions including the antiviral market model in §2. Simulation settings are laid out in §3. We present our experimental results in §4 and conclude in §5. 2 Modeling Framework This study assumes that a “flu-like” disease spreads in a population through person-to-person contact. The disease progression within a host follows the usual SEIR model, explained in §2.1. Person to person contacts form a social contact network, explained in §2.2. Interventions to mitigate the epidemic includes antiviral administration that decreases the probabilities of disease transmission, and social distancing measures that decrease person-to-person contact, which eventually decrease the probabilities of disease transmission too. Details of the interventions are described in §2.3. We propose a multiple theory methodology and describe the coevolution of epidemics, social networks, and human behavior in §2.4 2.1 SEIR Disease Model In this study we follow the standard SEIR disease model from the mathematical epidemiology literature [2, 16, 19]. Each person in the model is in one of the following four health states at any time: susceptible, exposed, infectious, and removed. A person is in the susceptible state until he becomes exposed. If person v becomes exposed, he remains exposed for αv days, called incubation period, during which he is not infectious. Then he becomes infectious and remains so for γv days, called infectious period, during which he may be symptomatic or asymptomatic. A person in the infectious state will probabilistically transmit the disease to any of his contacts that are in the susceptible state. An asymptomatic person is less likely to transmit the disease to other people 2 than a symptomatic person. After γv days the infectious person v becomes removed (or recovered) and remains so permanently. Note that these state transitions are not reversible and are the only possible transitions. The SEIR disease model is explained in more detail in [5]. 2.2 Contact Network A contact network is a directed, edge-weighted graph G(V, E, w). Nodes V correspond to individuals in the population. Edges E represent contacts between individuals during each day and edge weights are the contact durations. There exists edge (u, v) ∈ E with weight w(u, v) if and only if node u has contact of duration w(u, v) with node v every day. The probability of disease transmitting from an infectious node u to a susceptible node v is an increasing function of the infectivity of the disease and the contact duration w(u, v). More details about the social contact network model and the disease propagation on a contact network can be found in [5]. 2.3 Interventions Interventions include pharmaceutical interventions (PI) and non-pharmaceutical interventions (NPI). PI interventions include administering antivirals, antibiotics and vaccines. NPI interventions refer to actions that effectively change the social network without administering any drugs. This includes various kinds of social distancing, such as school closure and isolation. See the recent federal pandemic influenza plan [8] for discussions on the efficacy of social distancing measures. At implementation level, a PI only changes the infectivity (if already in infectious state) or vulnerability (if still susceptible) of the intervened person. He maintains his usual daily activities. So the disease may transmit through the contact network via the same edges. But he becomes less likely to get infected and even if he is infected he will be less likely to infect other people. On the contrary, an NPI changes the person-person interactions. For example, if we isolate a household, then each household member only has contacts with other members of the household. Any contact edge between a household member and an outside individual will be removed during the isolation. Interventions can also be classified as public health level measures and household level selfinterventions. The former does not involve a micro-level decision making based on private information such as household income. It includes antiviral administration through clinics to diagnosed individuals, and school closure. The latter involves household level decisions. We consider two kinds of household level interventions. One, each household can decide the amount of antivirals to demand in the market based on the price for antiviral, its budget, level of prevalence of the disease and its own risk aversion towards the disease. Each household can also decide to isolate all its members at home if one member shows symptoms. 2.3.1 Antiviral Market. In existing works the distribution of antiviral drugs is studied from the public health viewpoint. They are given to people, either targeted or random, chosen by the authorities [18, 22]. Who will receive antiviral is decided at the population level. In this work we explore antiviral distribution through the market. In an antiviral market who get the drugs is mainly an individual level decision, although the government can still plays an role, e.g., by putting an upper bound on the antiviral price. 3 We assume inelastic antiviral supply in the market and elastic demand from each household. The demand for antiviral of household h on day t, Dt,h , depends on the current epidemic prevalence xt , which is the fraction of the population in the infectious state on day t, the current market price Pt , ∂f ∂f ∂f ≥ 0. ≥ 0, ∂P ≤ 0, ∂B and its current budget constraint Bt,h : Dt,h = f (xt , Pt , Bt,h ). Usually ∂x t t t,h The demand function can take various functional forms, representing different risk aversion B (α + xβt ), upper towards the disease. For example, it can be linear in prevalence: Dt,h = Pt,h t B B bounded by Pt,h ; or exponential in prevalence: Dt,h = Pt,h (1 − e−γxt ). In the latter case the t t demand for antiviral increases quickly even at low levels of disease prevalence, compared with the former case. Therefore households with exponential demand are more sensitive to the epidemic. 2.4 Multiple Theory Methodology and Coevolution We propose a multiple theory methodology to study the coevolution of epidemics, social networks, and human behavior. We have developed an associated modeling environment, which is illustrated by a multi-layer representation in Figure 1. The first layer consists of a social contact network of individuals, as described in §2.2; the behavioral model on this layer is the within host disease progression, described in §2.1. The second layer consists of a social contact network of households. It is essentially the same as that on the first layer, except that all the nodes (individuals) from the same household are contracted to one node. The behavioral model on this layer is the household level self-motivated social distancing interventions, such as household isolation. The third layer consists of an economic network, where the nodes are the households as in the contact network on the second layer, plus a market node, and every household node is connected with the market node. The behavioral model on this layer is the household demand for antiviral. This novel methodology with the associated modeling environment is one of our major contributions. 2.4.1 Coevolution of Epidemics, Social Networks, and Human Behavior. Figure 2 shows how they interact with each other: (i) Disease dynamics affect individual behavior. Higher disease prevalence and infection occurring to themselves or household members make people voluntarily take social distancing measures and buy antiviral drugs from markets. (ii) Individual behavior changes the social network. Social distancing measures taken by individuals change the connectivity of the social contact network. (iii) Social network changes affect epidemic dynamics. Less connected contact network leads to fewer disease transmissions. (iv) Individual behavior affects the epidemic evolution. Antivirals taken by individuals lower their vulnerability to the disease and their infectvity to other people. This helps in containing the epidemic. 3 Experimental Setup In this section we describe our experiment environment and simulation settings. We introduce our simulation tool EpiFast in §3.1. Simulation data and parameters are described in §3.2. 3.1 EpiFast: a Fast Simulation for Epidemics EpiFast is a fast discrete event simulation for disease propagation over a contact network. It uses a parallel algorithm, which enables scaling on distributed memory systems. We have implemented 4 Mar Antiv ira ket l purc hase ork Netw c i om Econ Person p’s family Hous ehol ily) fam d iso lation al Soci Person p With in disea host se pr ogre ssion ct a cont ork ( netw al) ividu o etw ct n onta ial c nd rk (i S oc Figure 1: Multi-layer representation of our multiple theory modeling environment. transmissibility Epidemic Dymanics Social Network prevelance NPI(isolation) Individual Behavior antiviralmarket Figure 2: Interactions among epidemic dynamics, social network, and individual behavior. 5 EpiFast in C++/MPI and it is proved to be fast and scalable, and to be able to handle largescale realistic epidemic simulations. EpiFast uses a disaggregated, agent based model which can represent each interaction between individuals and hence study critical pathways of the diseases. Disaggregated models require neither partitions of the population nor assumptions about large scale regularity of interactions. See [13, 10, 11, 12, 17] for results and discussions on this topic. For the details of the underlying algorithm, parallel implementation, and performance of EpiFast, see [5]. 3.2 Simulation Configurations The study is performed on a synthetic population of New River Valley, Virginia. The synthetic population is a set of synthetic people and households, located geographically, each associated with demographic variables recorded in the US census. Joint demographic distributions are reconstructed from the marginal distributions available in typical census data using an iterative proportional fitting technique [4]. The process guarantees that a census of our synthetic population is statistically indistinguishable from the original US census data [3, 6, 10]. The New River Valley population has about 150,000 people. We assume that a fixed amount, 15,000 courses, of antiviral drugs are to be allocated between clinics and markets. When an individual becomes infectious, with probability 2/3 he appears symptomatic and goes to clinic; otherwise he is asymptomatic. In the latter case he is 47% less likely to transmit the disease. At the clinic, the symptomatic individual is diagnosed with probability 60% and given one course of the antiviral, until the clinic allocation of antivirals runs out. There is no cost for receiving antivirals from the clinic. An individual who is not infected may be mis-diagnosed as infected. For that, we assume one such mis-diagnosis in every six people diagnosed as infected. Similar assumptions have been made in the DHHS sponsored study [9]. Each household, each day, observes the level of epidemic prevalence and the market price of the antiviral, and determines demand for the antivirals. If a household has just made a purchase and is still using the purchased antiviral, it has no demand. The price of the antivirals depends Qt , where Pmax and Pmin are the on the remaining amount of supply: Pt = Pmax − (Pmax − Pmin ) Q 0 upper and lower bounds set by the government, and Qt is the antiviral supply on day t. We set Pmax = $150, Pmin = $50. The budget for antiviral purchase is 1% of each household’s income. In this study we use the exponential demand function and set γ = 20. The market clearing mechanism works as follows. If a household has a positive demand for antiviral, it buys one course for each member, unless the market supply exhausts, or its budget is insufficient to buy one course per member. It may buy antivirals again after it finishes using what it had purchased, until its budget for the antivirals is used up. Each course of antiviral is applied for 10 continuous days. When antiviral is applied to an infectious person, his probability of transmitting the disease is reduced by 80%; when applied to a susceptible person, his probability of being infected is reduced by 87%. Isolation measure is taken by households depending on their members’ health states as well as the overall level of the disease prevalence. We assume a global threshold for isolation. Isolation does not occur until the disease prevalence reaches 0.002. After the threshold is met, when a member of a household is diagnosed as infected, with compliance rate 40%, all members of this household isolate themselves at home, until the diagnosed member is recovered. The epidemic is started from 20 randomly chosen seeds and simulated for 200 days in each simulation run. The overall attack rate is about 45% when there is no intervention. In this study, we try different levels of antiviral allocation between the public sector (clinics) and the private 6 sector (markets), starting from nothing allocated to clinics, to all to clinics, in 1K increments. The simulations are run on a cluster using 10 processors. 4 Experimental Results and Discussion We are interested in the problem of optimal allocation, of a limited stockpile of antivirals, between the clinics and the market, with the goal of controlling the epidemic. The observations are discussed in §4.1. The coevolution problem is studied by observing the progression of the epidemic when the household demand function is dependent or independent of the epidemic prevalence, as well as when changes to the social network occur. The results are discussed in §4.2. 4.1 Optimal Antiviral Allocation The efficiency of the antiviral stockpile allocation between the clinics and the market, in terms of decreasing the attack rate, is shown in Fig. 3. The attack rate decreases as more of the antiviral stockpile is allocated to the clinics. This is because the antivirals allocated to the clinics are targeted to those who are infectious, while the market stockpile is distributed to people according to the household income rather than their health states. It may not be optimal to allocate all antiviral stockpile to clinics, however. The simulation results indicate that when 40% of the stockpile is assigned to the clinics, the attack rate reaches its minimum at 5%. After that, there is no significant decrease in attack rate from larger clinic allocation. The number of antivirals distributed by the clinics is approximately a constant fraction of the number of infected people. This is because only a fraction of the infected are symptomatic and of those, only a fraction go to clinic and of those, only a fraction are correctly diagnosed. Therefore, there is a lower bound on the attack rate below which the attack rate cannot be reduced through the clinic allocation. In our simulation experiments, this lower bound is 5%. Further allocation of antivirals to the clinics does not help reduce the attack rate because they do not get used. In light of this knowledge, it will be more efficient to allocate part of the antiviral stockpile to the market to help recover its production cost. In fact, our simulations show that if the antiviral unit price varies between $50 and $150, the 40-60 allocation (40% to the clinics and 60% to the market) scheme will help recover about $629k, see Fig. 4. This implies that if the actual cost of the antivirals is $42 or less, total revenue will be enough to break even. 4.2 Coevolution We are particularly interested in understanding the interactions between the epidemics, human behavior and social networks. The following experiment is performed to capture this interaction. Two sets of scenarios are simulated. In the first set, two types of demand is considered. One in which the demand for antivirals is independent of the level of disease prevalence; and in the other, demand is an exponential function of the prevalence. Other parameters and assumptions are the same as in §3.2 in both sets. This set is expected to shed light on how human behavior and the epidemics interact. In the second set, two types of household isolation strategies are allowed. In one, the household members isolate themselves when a member is diagnosed as infected and in the other the household members do not isolate themselves. In both cases all other parameters and assumptions are kept 7 Attack Rate Decreases with Increasing Clinic Allocation 30 Revenue from Antiviral Market vs. Clinic Allocation 1600 1400 1200 revenue ($k) attack rate (%) 25 20 15 1000 800 600 400 10 200 5 0 0 20 40 60 80 100 0 20 fraction allocated to clinics (%) 40 60 80 100 fraction (%) allocated to clinics Figure 3: Targeted antiviral intervention is more Figure 4: Recover cost of antiviral production effective. from the market. Prevalence over Time Demand over Time 4500 45 with isolation, D = function(prevalence) no isolation, D = function(prevalence) with isolation, D != function(prevalence) 3500 with isolation no isolation 40 35 3000 30 demand (k) number of infectious nodes 4000 2500 2000 25 20 1500 15 1000 10 500 5 0 0 0 50 100 day 150 200 0 Figure 5: Comparison of prevalence. 20 40 60 80 100 day 120 140 160 Figure 6: Comparison of demand. 8 180 200 the same. In both cases the demand is an exponential function of the prevalence. This set is expected to capture the effect of social networks on the epidemics. Now, we compare the following three cases: (i) isolation is on and the demand function is exponential in prevalence; (ii) isolation is off and demand is exponential in prevalence; (iii) isolation is on and demand is independent of the prevalence. In case (iii), each day each household with probability 0.01 has a positive demand for antivirals and otherwise has a zero demand. If it has a B . positive demand, the demand is Dt,h = Pt,h t Figure 5 compares the day-by-day prevalence under these three cases. It suggests that the dependence of demand on prevalence postpones the epidemic peak by about a month; and that isolation decreases the peak infections by more than 1000. In Fig. 6, we compare the day-by-day demand for antivirals under different cases. We omit case (iii) in the plot since the curve will be a flat line close to the x-axis. The figure suggests that antiviral demand increases by about 15K in the absence of isolation, which is mainly caused by higher prevalence. It is also interesting to see which households purchase antiviral from the market. We sort the households by per capita income and draw the percentile graph. In addition, we plot the amount of antiviral purchase, and the number of infected in these households in Fig. 7. Surprisingly, with exponential demand function, only households with income of 70 percentile or more buy antivirals, and the purchase is dominated by the richest percentile households. Households of lower income do not buy because early in the epidemic the prevalence is low; later in the epidemic when the prevalence increases, the price increases as well, making it unaffordable for the people with lower income. In the case where the demand is independent of prevalence, the antiviral purchase seems to be distributed more evenly among households of different income levels, see Fig. 8. Antiviral Purchase and Infection by Income Level 8000 7000 6000 6000 5000 5000 count count 7000 Antiviral Purchase and Infection by Income Level 8000 antiviral purchase exposure count 4000 4000 3000 3000 2000 2000 1000 1000 0 antiviral purchase exposure count 0 10th 20th 30th 40th 50th 60th 70th 80th 90th income percentile 10th 20th 30th 40th 50th 60th 70th 80th 90th income percentile Figure 7: Distribution of antivirals purchased Figure 8: Distribution of antivirals purchased and exposure counts by household income level. Demand is prevalence elastic. and infections by household income level. Demand is not prevalence elastic. 5 Conclusions We study the problem of allocating a limited supply of antiviral drugs between the private sector and the public sector to minimize an epidemic. We find that while the public sector should be given priority, it can be beneficial to distribute part of the stockpile through an antiviral market. This may help recover the cost of antiviral manufacturing, and achieve the overall goal of containing 9 the epidemic at the same time. Our simulation results also suggest significant interaction and coevolution of epidemics, social networks, and human behavior. References [1] Centre approves restricted retail sale of Tamiflu, 2009. http://www.livemint.com/2009/08/ 28001825/Centre-approves-restricted-ret.html. [2] N. T. Bailey. The mathematical theory of infectious diseases and its applications. Hafner Press, New York, 1975. [3] C. Barrett, K. Bisset, J. Leidig, A. Marathe, and M. Marathe. Estimating the impact of public and private strategies for controlling an epidemic: A multi-agent approach. In Proceedings of the 21st IAAI Conference, 2009. [4] R. J. Beckman, K. A. Baggerly, and M. D. McKay. Creating synthetic baseline populations. Transportation Research, Part A: Policy and Practice, 30:415–429, 1996. [5] K. Bisset, J. Chen, X. Feng, V. A. Kumar, and M. Marathe. EpiFast: a fast algorithm for large scale realistic epidemic simulations on distributed memory systems. In Proceedings of the 23rd International Conference on Supercomputing (ICS), pages 430–439, 2009. [6] K. Bisset and M. Marathe. A cyber environment to support pandemic planning and response. DOE SciDAC Review Magazine, Issue 13, Summer 2009. [7] Dept. of Health and Huamn Services. Guidance on antiviral drug use during an influenza pandemic 2009. http://www.flu.gov/individualfamily/vaccination/antiviral_use.pdf, accessed on Nov 6, 2009. [8] Dept. of Health and Huamn Services. HHS pandemic influenza plan, 2007. [9] J. Epstein, S. Eubank, M. Lipsitch, R. Hammond, C. Bergstrom, E. Goldstein, A. Marathe, M. Raifman, and B. Lewis. Modeling of distribution alternatives of home antiviral drug stockpiling. NIH MIDAS Meeting, June 17, 2008. [10] S. Eubank, H. Guclu, V. A. Kumar, M. Marathe, A. Srinivasan, Z. Toroczkai, and N. Wang. Modeling disease outbreaks in realistic urban social networks. Nature, 429:180–184, 2004. [11] N. L. Ferguson, D. A. T. Cummings, S. Cauchemez, et al. Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature, 437:209–214, 2005. [12] N. L. Ferguson, D. A. T. Cummings, C. Fraser, J. C. Cajka, P. C. Cooley, and D. S. Burke. Strategies for mitigating an influenza pandemic. Nature, 442:448–452, 2006. [13] T. Germann, K. Kadau, I. M. Longini Jr, and C. A. Macken. Mitigation strategies for pandemic influenza in the United States. PNAS, 103(15):5935–5940, 2006. [14] M. Gersovitz and J. S. Hammer. Infectious diseases, public policy, and the marriage of economics and epidemiology. The World Bank Research Observer, 18(2):129–157, 2003. 10 [15] M. Kremer. Integrating behavioral choice into epidemiological models of the AIDS epidemic. The Quarterly Journal Of Economics, 111(2):549–73, 1996. [16] Y. Kuznetsov and C. Piccardi. Bifurcation analysis of periodic SEIR and SIR epidemic models. Journal of Mathematical Biology, 32:109–121, 1994. [17] L. Meyers, M. Newman, M. Martin, and S. Schrag. Applying network theory to epidemics: Control measures for outbreaks of mycoplasma pneumonia. Emerging Infectious Diseases, 9:204–210, 2003. [18] A. Monto, M. Pichichero, S. Blanckenberg, et al. Zanamivir prophylaxis: an effective strategy for the prevention of influenza types A and B within households. J Infect Dis, 186:1582–8, 2002. [19] J. D. Murray. Mathematical Biology: I. An Introduction. Springer, 3rd edition, 2007. [20] T. Philipson. Economic epidemiology and infectious diseases. In A. J. Culyer and J. P. Newhouse, editors, Handbook of Health Economics, volume 1, chapter 33, pages 1761–1799. Elsevier, 2000. [21] M. Rabin. A perspective on psychology and economics. European Economic Review, 46:657– 685, 2002. [22] R. Welliver, A. Monto, O. Carewicz, et al. Effectiveness of oseltamivir in preventing influenza in household contacts: a randomized controlled trial. JAMA, 285:748–74, 2001. 11