Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hospital-acquired infection wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Herd immunity wikipedia , lookup
Vaccination wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Infection control wikipedia , lookup
Kawasaki disease wikipedia , lookup
Meningococcal disease wikipedia , lookup
Chagas disease wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Schistosomiasis wikipedia , lookup
Behçet's disease wikipedia , lookup
Ankylosing spondylitis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Neonatal infection wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Germ theory of disease wikipedia , lookup
365
Invasive Group B Streptococcal Disease: The Emergence of Serotype V
Henry M. Blumberg, David S. Stephens,
Matthew Modansky, Melinda Erwin, John Elliot,
Richard R. Facklam, Anne Schuchat, Wendy Baughman,
and Monica M. Farley
Division of Infectious Diseases, Department of Medicine, Emory
University School of Medicine; VA Medical Center; and Centers for
Disease Control and Prevention, Atlanta, GA.
Group B streptococci (GBS) cause invasive disease in neonates, pregnant adults, and nonpregnant
adults with underlying or chronic disease. Previous studies found capsular serotypes la, Ib, II, and
III cause invasive disease. Prospective population-based surveillance of invasive GBS disease was
done from June 1992 to June 1993 in metropolitan Atlanta: 279 patients had invasive disease. Of
these, 43% were ,;;;6 months old, and 57% were adults. The incidence among all adults was 7.7/
l00,OOO/year, 33% higher than in 1989-1990 (P < .01); the incidence in nonpregnant adults was
5.9/100,OOO/year, 37% higher than in 1989-1990 (P < .02). Serotyping of 178patient isolates revealed
that 34% had GBS serotype la or Ia/c, 8% had Ib/c, 6% had II or Wc, 29% had III, 0% had IV,
21% had V, and 2% were nontypeable. Serotype V was recovered from all groups and was the most
common serotype from nonpregnant adults. Serotype V isolates appeared to be highly related
genetically. The increasing incidence of GBS disease in adults, the changing distribution of serotypes,
and the emergence of serotype V will impact vaccine strategies.
Group B streptococci (Streptococcus agalactiae; GBS) are
the leading cause of sepsis and meningitis in newborns in the
United States and cause significant pregnancy-related morbidity affecting ~ 50,000 women each year in the United States
[1-4]. Recently, it has been recognized that GBS are also an
important cause of invasive disease in nonpregnant adults [5].
GBS disease in nonpregnant adults most commonly affects the
elderly or those with chronic disease (e.g., diabetes mellitus,
malignancy, and liver disease) and is often associated with a
rate of high mortality [5, 6].
GBS are classified into serotypes on the basis of structural
differences in capsular polysaccharides (Ia, Ib, and II- VI) and
the presence or absence of protein antigen c [7]. Protein antigen
c occurs in many serotype Ia and II strains, in all Ib strains,
and in some serotype IV and VI strains [8]. Serotyping has
been used traditionally to type GBS isolates; a currently used
serotyping system consists of Ia, Ia/c, Ib/c, II, Il/c, III, IV, and
V and of nontypeable isolates. The R and X protein antigens
classify a few additional human strains but are most useful for
serotyping bovine strains [9].
Received 28 April 1995; revised 20 October 1995.
Presented in part: Clinical Research Meeting, American Federation for Clinical Research, Baltimore, 2 May 1994 (abstract N-IN-0067).
Human Investigation Committee approval for this study was received from
the Emory University School of Medicine, the Georgia Department of Human
Resources, and the Centers for Disease Control and Prevention.
Financial support: Emory Medical Care Foundation, University Research
Council of Emory University, National Vaccine Program, and Medical Research Service of the Department of Veterans Affairs.
Reprints or correspondence: Dr. Henry M. Blumberg, Division of Infectious
Diseases, Emory University School of Medicine, 69 Butler St., S.E., Atlanta,
GA 30303.
The Journal of Infectious Diseases 1996; 173:365-73
© 1996 by The University of Chicago. All rights reserved.
0022-1899/9617302-0012$01.00
Resistance to infection with GBS has been correlated with
the presence of serum antibodies to type-specific determinants
of capsular polysaccharides in both experimental animals and
human neonates [10, 11]. Ongoing efforts to develop efficacious vaccines for the prevention of GBS disease in humans
will require precise knowledge about serotype distribution and
groups at risk for infection.
Previous studies have reported a distribution of capsular
serotypes Ia, Ib, II, and Ill, with few nontypeable isolates in
neonates with early-onset disease (i.e., GBS disease occurring
in the first week of life) and among pregnant women with
vaginal GBS colonization [2,12-14]. Late-onset neonatal disease (i.e., disease occurring in newborns ~7 days of age) and
meningitis among neonates is due primarily to serotype Ill,
which accounts for 70% of such cases [15]. Little is known
about serotype distribution or genetic relatedness of GBS isolates recovered from nonpregnant adults with invasive disease.
Using prospective population-based surveillance, we explored the incidence of GBS disease among all age groups, the
distribution of serotypes among GBS isolates recovered from
those with invasive disease, including nonpregnant adults, and
the molecular epidemiology of GBS disease in metropolitan
Atlanta.
Materials and Methods
Population-based surveillance. We did a prospective population-based surveillance of invasive GBS disease in the eight-county
metropolitan Atlanta area from 1 June 1992 through 30 June 1993.
The population of the surveillance area was 2,460,233 during the
study period (Georgia Department of Human Resources, Atlanta).
About 68% of the residents were white, 29% were black, and 3%
were of other races or ethnic groups (1990 US census data). During
the study period, there were 44,473 live births in the surveillance
area (Georgia Department of Human Resources).
366
Blumberg et al.
Infections were diagnosed on the basis of isolation of GBS from
normally sterile sites (e.g., blood, peritoneal fluid, or cerebrospinal
fluid). All patients with invasive GBS disease were living in the
surveillance area during the study period. Patients with urinary
tract infections and those with placental isolation were not included
unless they had bacteremia. GBS isolates were collected from 32
hospitals and 1 referral laboratory. Strains were identified as GBS
at local hospital laboratories with standard, commercially available
diagnostic kits. All kits were based on the extraction of streptococcal group antigens in soluble form and their identification with
use of latex particles coated with group-specific antibody. Isolates
collected from hospital clinical microbiology laboratories were
subcultured and incubated overnight. GBS isolates were then
stored at -70°C in sheep's blood until serotyping and molecular
typing studies were done.
Initial case reports of invasive GBS disease were obtained from
two independent sources: hospital microbiology laboratories and
hospital infection control practitioners. Every 6 months during the
study period, laboratory audits were done at all hospitals to evaluate reporting accuracy and to identify any cases that had not been
reported. Demographic information (including age, sex, race, and
pregnancy status) and clinical findings were obtained for all patients.
Serotyping. Serotyping was done by the Lancefield capillary
precipitin method [16]. Antisera to polysaccharide antigens la, Ib,
II, III, IV, and V and protein antigen c were used. Antisera were
prepared at the Centers for Disease Control and Prevention (CDC;
Atlanta).
Molecular typing studies. DNA restrictionfragment length polymorphism(RFLP) of rRNA genes (ribotyping) and restrictionendonuclease analysis of chromosomal DNA (REAC) were done as previouslydescribed[17].ChromosomalDNA was extractedas described
by Pitcher et al. [18] after organisms were grown overnight in ToddHewitt broth at 37°C with aeration. DNA (3 J-tg) was digested by
Hhal (1 J-tL or 10 U) for 2 h at 37°C in a 20-J-tL reaction mixture
accordingto manufacturer'srecommendations (New EnglandBiolabs,
Beverly, MA). An additional I J-tL of restriction enzyme was added,
and the reactionmixturewas reincubatedfor 2 h. Hhal was previously
shown to provide the best discrimination of hybridization banding
pattems among 24 restriction enzymes studied [17]. The digested
DNA was electrophoresed in a 1% agarose horizontalgel at 60 V for
18 h in TRIS-acetate buffer. After electrophoresis, gels were stained
in ethidiumbromide and photographed under UV light. A l-kb ladder
and A phage (GIBCO BRL, Gaithersburg, MD) were used as molecular size standards. Digested and electrophoresed DNA restriction fragments were denatured and transferredto a nylon membrane (magnagraph; MSI, Westboro, MA) by the method of Southem [19].
Escherichia coli 16Sand 23S rRNA (BoehringerMannheimBiochemicals,Indianapolis) were used for the probe.Hybridization experiments
were done with a nonradioactive labeling system (Genius system;
Boehringer Mannheim) as previously described [20, 21].
Pulsed-field gel electrophoresis (PFGE) was done on 47 GBS
isolates; whole cell DNA was prepared as described by Murray et
al. [22] with the following modifications: Mutanolysin (lJ-tg/mL;
Sigma, St. Louis) was added to the bacterial lysis solution, and
whole cell DNA was digested with Smal (Boehringer Mannheim).
PFGE was done using the contour-clamped homogeneous electric
field method; pulse time was increased from 1 to 30 s over 23 h
at 200 V. A A ladder PFGE marker (Boehringer Mannheim) was
JID 1996; 173 (February)
used as a molecular size standard. PFGE banding patterns were
compared visually; strains were considered distinguishable if
PFGE patterns differed by ;,,3 bands [23]. Banding patterns were
also compared by use of a computer-assisted system in which
DNA typing gels were analyzed using Bio Image/Millipore whole
band analyzer software (Bio Image, Ann Arbor, MI). Cluster analysis using the method ofunweighted pair-group average was done
to calculate similarity or dissimilarity among GBS isolates. A significant difference was defined as a coefficient of similarity of
<80%.
Statistical analysis. Incidence rates of invasive GBS disease
in the eight-county area during the study period were compared
to those previously reported [5] for the same area in 1989-1990
using Fisher's exact test. The surveillance area and methodology
used during both time periods were identical. Incidence rates of
GBS disease in black and in white patients during the study period
were compared using the Xl test. P < .05 was considered significant.
Results
Over 13 months (1 June 1992 to 30 June 1993), there were
279 cases of invasive GBS disease in metropolitan Atlanta.
Overall, 112 (40%) of the cases occurred among nonpregnant
adults, 48 (17%) among pregnant adults, 90 (32%) among neonates <7 days of age (early-onset neonatal disease), and 31
(11%) among infants ~7 days to <6 months old (late-onset
neonatal disease). There were no cases in persons 6 months to
15 years old. Of the 119 neonatal cases, 76% were due to
early-onset and 24% to late-onset neonatal disease. Of the 160
adult cases, 30% were pregnancy related and 70% occurred in
nonpregnant adults. The mean age of the adults with nonpregnancy-related GBS was 57.2 ± 18.1 years, and 53% were men.
Of the 279 people with GBS infection, 53% were black, 44%
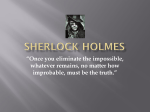
white, and 3% were of other races or ethnic groups. The incidence of invasive GBS disease was significantly higher among
blacks than whites for all age groups (P < .05) except the 5to 14-year-old group, in which there were no cases of invasive
GBS disease (figure 1).
The overall incidence of invasive GBS disease during the
study period was 10.51100,000 residents/year; this was a 14%
increase from 1989-1990, but the difference was not statistically significant (P = .1; table 1). The incidence among all
adults was 7.7/100,000/year during the study period, which
was 33% higher than in 1989-1990 (P < .01). This increase
among all adults (> 15 years old) was due to the increase in
GBS cases among nonpregnant adults. There were 5.9 cases/
100,000/year among nonpregnant adults, during the study period, 37% more than in 1989-1990 (P < .02). There were 2.7
cases/IOOO live births, a number similar to that seen in 19891990 (table 1).
Serotyping. GBS isolates from 178 (64%) of the 278 patients were available for further study. Serotyping and molecular typing studies were done on these isolates (81 from infants,
65 from nonpregnant adults, and 32 from pregnant adults). The
367
Emergence of Serotype V GBS Disease
JID 1996; 173 (February)
120
• Black
100
o
White
80
60
Figure 1. Incidence of invasive
GBS disease in metropolitan Atlanta
by age and race.
40
20
o L-~~~~==:::e====::-----j
5-14
0-4
15-39
40-59
60-74
Age (yr)
distribution of GBS serotypes is shown in table 2. Overall,
34% of the isolates were serotype la or laic, 8% were Ib/c, 6%
were II or Il/c, 29% were III, 0% were IV, 21% were serotype
V, and 2% were not typeable. Serotype V isolates were recovered from all age groups (neonates, pregnant adults, and nonpregnant adults). The proportion of GBS cases due to serotype
V ranged from 11% in the neonates to 31% among the nonpregnant adults. Serotype V and la or laic were the most common
serotypes associated with invasive GBS disease among nonpregnant adults (table 2).
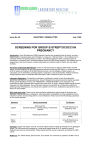
Molecular epidemiologic typing. One hundred seventy of
the GBS isolates were evaluated by restriction endonuclease
analysis of chromosomal DNA (REAC) and restriction fragment length polymorphism of rRNA genes (ribotyping) (figures
2,3). Overall, 13 different hybridization banding patterns (ribo-
Table 1. Incidence of invasive GBS disease in metropolitan Atlanta
(per 100,000 residents/year).
19921993
Overall
Adults
All (~15 years old)
Nonpregnant
(~20 years old)
Pregnant
Infants
(",6 months old)
Data from [5].
19891990'
Change
('Yo)
P
10.5
9.2
14
.10
7.7
5.8
33
<.01
5.9
66.4
4.3
49.4
37
34
<.02
.14
2.7 cases/
1000 live
births
2.6 cases/
1000 live
births
4
>.2
types) were noted among the 170 GBS isolates studied; 10 of
the ribotypes are shown in figure 2B. Three different ribotype
patterns were noted among the 58 la or laic isolates, 1 ribotype
among 13 serotype Ib/c isolates, 6 ribotypes among 11 serotype
II or Il/c isolates, 5 ribotypes among 47 serotype III isolates,
and a single ribotype (pattern 3) among all 37 serotype V
isolates studied. The distribution of ribotypes is shown in table
3. Patient age or race did not affect the distribution ofribotypes
(data not shown). All serotype Ib/c and V isolates and 3 serotype Il/c isolates had ribotype pattern 3 (table 3). Serotype V
isolates had identical or very similar REAC patterns; the REAC
pattern observed with serotype V isolates clearly differed from
that seen with serotype Ib/c isolates or ribotype 3, serotype
Il/c isolates (figure 3).
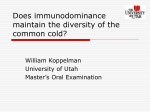
Forty-seven GBS isolates (33 serotype V and 14 of other
serotypes) were also studied by PFGE (figure 4). Twenty-five
of the 33 serotype V GBS isolates had the same PFGE banding
pattern, and all 33 serotype V GBS isolates were highly related,
having a coefficient of similarity of >80% (figure 4A). The
serotype V isolates were clearly different than other GBS serotypes studied by PFGE; the similarity coefficient between the
serotype V isolates and those of other serotypes studied was
50% (figure 4B). PFGE clearly differentiated between isolates
of different serotypes (V, Ib/c, and Il/c) that had ribotype pattern 3.
Discussion
GBS infections have emerged as an important cause of morbidity and mortality among nonpregnant adults as well as neonates and pregnant or postpartum women [5, 7). Our study
indicates that the incidence of invasive GBS disease among
368
lID 1996; 173 (February)
Blumberg et al.
Table 2. Distribution of GBS serotypes.
Adults
Neonates
Serotype
Overall
Early
Late
Total
Pregnant
Nonpregnant
Ia, laic
lb/c
60 (34)
15 (8)
II (6)
51 (29)
0
37 (21)
4 (2)
178
23 (36)
6 (9)
5 (8)
19 (30)
0
9 (14)
2 (3)
64
4 (23)
I (6)
0
12 (71)
0
0
0
17
27 (33)
7 (9)
5 (6)
31 (38)
0
9 (II)
2 (3)
81
13 (41)
4 (12)
I (3)
6 (19)
0
8 (25)
0
32
20 (31)
4 (6)
5 (8)
14 (21)
0
20 (31)
2 (3)
65
II, We
III
IV
V
NT
Total no.
NOTE. Data are no. (%) of patients. NT = nontypeable; early = early-onset neonatal disease (among infants
<7 days old); late = late-onset neonatal disease (among infants ;,,7 days of age).
A
Kh
lane
M
I
2
3 4 5
6
7
8
9 10 11
B
48.5 12.2 -
Kh
lane
M
2
1
3
4
5
6
7
8
9
6
7
10 1I
12.2 -
4.1 3.1 4.1 3.1-
2.0 2.0-
1.0 -
1.0-
-,--llJ t, ~II------r-serotype
laic
Ib/e V
We
III
ribotype
serotype
_-r--_lll ~ ~ U
2
laic
Iblc
V
IIIc
8
1L-- - - - , r - - III
Figure 2. A, Restriction endonuclease analysis of chromosomal DNA patterns of selected GBS isolates. Lane nos. correspond to those in
B. B, Corresponding hybridization banding patterns (ribotypes). Serotypes and ribotype pattern numbers are at bottom. By lane, serotype,
ribotype, and isolate designations are I, laic, I, and 400; 2, laic, 2, and 404; 3, laic, II, and 332; 4, Ib/c, 3, and 32 I; 5, V, 3, and 380; 6, III
c, 5, and 572; 7, IIIc, 12, and 406; 8, III, 6, and 441; 9, III, 7, and 368; 10, III, 8, and 324; and 11, III, 10, and 390. M, l-kb ladder (molecular
size marker).
lID 1996; 173 (February)
369
Emergence of Serotype V GBS Disease
lane
12M 3 4 5 6 7 8 9 10 II 12 13 14 15 16
48.5 -
12.2 -
5.1 Figure 3. Restriction endonuclease anal-
ysis of chromosomal DNAof GBS isolates
with ribotype pattern 3. Serotypes are at
bottom. By lanes, isolate designations are
I, 445; 2, 408; 3, 366; 4, 321; 5, 403; 6,
340; 7, 455; 8, 335; 9, 380; 10, 381; II,
360; 12, 388; 13, 389; 14, 384; 15, 385;
and 16,386. M, l-kb ladder(molecular size
marker).
4.1 -
2.0 -
1.0 -
IIle
lIIe
I~I~I~I~
V
V
V
V
V
V
V
V
V V
serotype
adults continues to increase in metropolitan Atlanta, primarily
due to an increase of disease among nonpregnant adults. In
our prospective population-based study, there was a 37% increase in the incidence of invasive disease among nonpregnant
adults in 1992-1993 (to 5.9 cases/100,000/year) compared
with a similar study in 1989-1990 [5]. In fact, the incidence
of invasive GBS disease appears to have more than doubled
over the past decade in metropolitan Atlanta. A populationbased retrospective survey by Schwartz et al. [6] done in metropolitan Atlanta in 1982-1983 estimated the annual incidence
of invasive GBS disease among nonpregnant adults to be 2.4/
100,000.
The reasons for the continuing increase in disease are unclear, although one factor may be longer survival of adults with
underlying chronic diseases who are at greatest risk for GBS
infection [7]. A 34% increase in the incidence of pregnancyrelated GBS disease among women during 1992-1993 compared with 1989-1990 was also seen, but the difference did
not achieve statistical significance (P = .14). There appears to
have been a marked increase in the incidence of pregnancyrelated disease in metropolitan Atlanta over the past decade,
as we noted a 3-fold increase in the incidence of pregnancyrelated adult disease compared with that reported by Schwartz
et al. [6] (66.4 vs. 22/100,000 pregnancies). The incidence of
neonatal or infant cases (2.7/1000 live births) during our study
period was unchanged from that in 1989-1990. It remains
to be determined whether recently published strategies (i.e.,
intrapartum chemoprophylaxis of high-risk maternal carriers)
to prevent infection of the neonate [1, 24, 25] will influence
rates of neonatal infection in metropolitan Atlanta. A survey
done in August 1993 of 192 physicians suggested that many
Georgia physicians who provide obstetric care were not using
recommended practices to prevent perinatal GBS disease [26].
In our surveillance area, blacks account for 29% of the population, but over half of all patients with invasive GBS disease
were black. The incidence of GBS infection was higher among
blacks than whites for all age groups (i.e., infants and pregnant
and nonpregnant adults). Our findings are consistent with those
nn 1996;173 (February)
Blumberg et al.
370
Serotype
A
..--. V
V
2
'---v
3
_v
4
V
5
I-...-V
6
V
7
V
8
I
9
Iale
10
Iale
11
Ilie
12
1
I lie
13
1
III
14
I
15
III
16
III
17
1
II
18
1
Ille
19
1
Ihle
20
1
r
Ihle
21
1
I
Ihle
22
2
25
I-
I
1
I
I
1
L--
r
1
50
55
60
65
70
75
80
85
90
95
1
1
Figure 4. A, Dendrogram of 47
GBS isolates studied by pulsed-field
gel electrophoresis (PFGE) showing
degree of relatedness (coefficient of
similarity). Serotype, lane no. corresponding to lanes in B, and no. of
isolates with particular PFGE banding pattern are at right. B, Representative PFGE patterns ofGBS. Lanes:
1-8 are serotype V (isolates 576,
360, 385, 472, 392, 402, 380, and
526, all ribotype 3); 9-11 are laic
(isolate 453, not ribotyped; isolates
442 and 440, ribotypes 1 and 2, respectively); 12 and 13 are Il/c (isolates 408 and 437, ribotype 3); 14 is
II (isolate 345, ribotype 8); 15 is III
(isolate 377, ribotype 8); 16 and 17
are III (isolates 396 and 227, ribotype 6); 18 is II (isolate 517, ribotype
5); 19 is Wc (isolate 406, ribotype
12); and 20-22 are lb/c (isolates
426, 337, and 340, ribotype 3).
100
Coefficient of Similarity (%)
of previous studies, which also noted higher rates of GBS
infection among blacks [5, 6, 27, 28]. The reasons for higher
rates of GBS disease among blacks than whites are incompletely understood. Differences in the incidence of disease may
reflect socioeconomic conditions or potentially higher rates of
chronic disease among nonpregnant black adults. Higher rates
of pregnancy-related and neonatal disease among blacks may
also be related to higher rates of vaginal colonization. Regan
et al. [29] found a higher prevalence of GBS vaginal colonization in black (~2l %) than in white (~14%) pregnant women.
Other smaller studies, however, have reported no differences
in GBS prevalence by ethnic group [30, 31].
Despite structural similarities, the GBS capsular type polysaccharides (la, lb, II, III, IV, V, and VI) are immunologically
distinct, and mechanisms of host protection are believed to be
based in large part on recognition by antibodies of capsular
antigen specificity. Antisera raised to GBS type-specific capsular antigens are protective against experimental GBS infection, and in human disease, type-specific antibodies correlate
with protection in neonates [10]. In contrast, antisera to the
common group B antigen fail to protect in animal models of
lethal GBS infection, and the level of naturally occurring common group B antibody correlates poorly with resistance to
human infection [10, 32, 33]. Current research is focused on the
Emergence of Serotype V GBS Disease
JID 1996; 173 (February)
B
Kb
371
lane
2
3
4
5
6
7
8
9 10 1112 13 14 15 16 17 18 19 20 21 22
533.5~36.5-
339.5-
291.0242.5194.0145.5-
97.0-
48.5-
development of type-specific polysaccharide-protein conjugate
vaccines. Encouraging results in immunogenicity have been
obtained for capsular polysaccharide -protein conjugate vaccines of serotypes Ia, II, III, and, recently, serotype V in the
Table 3.
Serotype
la, laic
la, laic
laic
Ib/c
We
We
II
II
We
We
III
III
III
III
III
V
NT
laic
Ib/c
III
Distribution of hybridization banding patterns (ribotypes).
Ribotype pattern*
n
1
2
II
3
3
4
5
8
12
13
36
6
23
13
9
1
1
37
4
2
2
4
7
8
10
14
3
3
NO
NO
NO
21
1
13
3
I
2
3
I
1
NT = nontypeable; ND = not done.
* Ribotype pattern indicates hybridization banding pattern as shown in
NOTE.
figure 2B.
prevention of GBS infection in a mouse animal model [II,
34, 35].
Knowledge of the distribution of serotypes is essential for
developing and formulating a protective human GBS vaccine.
Our data suggest that there has been a significant shift in the
distribution ofGBS serotypes causing invasive disease and that
serotype V has emerged as a major cause of disease. Studies
done more than a decade ago indicated that neonatal disease
was caused by serotypes la, Ib, II, and III, with few nontypeable
isolates [2, 12-14]. Little has been known about serotype distribution among adults, especially among nonpregnancy-related
cases. In our study, serotype V isolates were seen among all
age groups except neonates with late-onset disease. Serotype
V isolates accounted for 21 % ofthe 178 GBS isolates examined
(14% in neonates with early-onset disease, 25% in pregnant
adults, and 31% in nonpregnant adults). Serotype V was the
most common serotype recovered from nonpregnant adults
with invasive GBS disease and the second most commonly
recovered serotype from pregnant adults. Clearly, an effective
capsular polysaccharide vaccine to prevent disease among neonates and pregnant and nonpregnant adults should be multivalent and provide protection against serotype V disease.
Serotype V was first reported by Jelinkova and Motlova [36]
in 1985; it was identified among a collection of previously
nontypeable GBS isolates recovered between 1960~ 1981, including nontypeable US isolates collected by Wilkinson [37].
Type-specific antibodies to serotype V isolates do not crossreact with other GBS capsular types and appear to recognize
an epitope that is not as heavily dependent on the presence of
372
Blumberg et al.
the terminal side chain sialic acid residues as that of type la,
II, and III GBS polysaccharides [38]. Serotype V isolates have
been recovered from a number of countries around the world
[31,39-42]; however, these reports suggested that serotype V
was a distinctly uncommon serotype. There have been a few
recent clinical case reports that have described invasive GBS
disease due to serotype V in neonates with early- or late-onset
disease in the United States and Europe, and there has been a
report of invasive disease in one nonpregnant adult [43-46].
In addition, a recent brief report indicated that serotype V
disease had emerged in Maryland and accounted for 9 (12%)
of 77 GBS isolates recovered from neonates and 44 (31%) of
141 isolates recovered from adults with invasive GBS disease
in 1991-1993 [47]. Our findings on the proportion of serotype
V isolates causing invasive GBS disease in Atlanta are similar
to those reported from Maryland.
It is uncertain when, how, and why serotype V emerged, but
it may have been a common serotype in the United States since
at least the mid-1980s. Serotyping studies on isolates recovered
from neonates in the 1970s rarely demonstrated isolates that
were nontypeable. However, a prospective laboratory-based
surveillance project by the CDC in 1986 in California, Missouri, New Jersey, Oklahoma, Tennessee, and Washington recovered a number of GBS isolates that were nontypeable by
antisera to serotypes Ia, lb, II, and III (17 [24%] of 72 isolates
recovered from nonpregnant patients >6 months of age, 5
[12%] of 43 from pregnant patients, and 10 [8%] of 110 from
patients with early-onset neonatal disease) [15]. Many of the
nontypeable isolates from that CDC project have recently been
demonstrated to be serotype V isolates (unpublished data). In
addition, a number of GBS isolates recovered from nonpregnant adult patients at Grady Memorial Hospital (Atlanta) in
1987-1988 that were nontypeable with antisera to serotypes
Ia, lb, II, and III have recently been confirmed as serotype V
(unpublished data).
Molecular analyses of GBS using REAC and ribotyping or
PFGE have proven to be useful subtyping methods and have
provided the ability to discriminate among isolates of the same
serotype [17, 48-50]. In our study, we noted 13 different ribotype patterns among the 170 isolates studied; 159 isolates were
of six different ribotype patterns. As noted previously [17],
these methods were very reproducible and REAC appeared to
be a more sensitive typing method than ribotyping. PFGE also
proved to be more sensitive than ribotyping, and because fewer
bands are produced, it is much simpler than REAC to analyze.
All serotype V isolates studied had the same ribotype (pattern
3) and the same or similar REAC patterns, and the 33 serotype
V isolates studied by PFGE had the same or similar PFGE
banding patterns (coefficient of similarity of >80%), suggesting that serotype V GBS isolates recovered from patients
in our surveillance area are highly related. PFGE and REAC
clearly differentiated between serotype V isolates and isolates
of other serotypes (Ib/c and Il/c) that had ribotype hybridization
banding pattern 3. Molecular analysis of serotype V isolates
JID 1996; 173 (February)
from other geographic areas will be needed to definitively determine if all serotype V isolates are highly related.
In summary, the incidence of invasive GBS disease (particularly among nonpregnant adults) continues to increase in the
Atlanta area. Serotype V has emerged as a major cause of
disease among all age groups and especially among adults.
Serotype V isolates recovered from patients with invasive disease appear to be highly related genetically, suggesting the
dissemination of closely related strains. The changing distribution of serotypes and emergence of serotype V will have a
major impact upon vaccine development.
Acknowledgments
We thank 1. WilliamEley for assistancewith statistical calculations, Susan Hunter for assistance with cluster analysis, and the
hospitals of Georgia Health District III and the staff of the Atlanta
Active Surveillance Project for help and cooperation.
References
I. American Academy of Pediatrics, Committee on Infectious Diseases,
Committee on Fetus and Newborn. Guidelines for prevention of group
B streptococcal (GBS) infection by chemoprophylaxis. Pediatrics
1992;90:775-8.
2. Baker CJ, Edwards MS. Group B streptococcal infections. In: Remington
JS, Klein JO, eds. Infectious diseases of the fetus and newborn infant.
4th ed. Philadelphia: WB Saunders, 1995;980-1054.
3. Institute of Medicine, National Academy of Sciences. New vaccine development: establishing priorities. Vol I. Diseases of importance in the
United States. Washington, DC: National Academy Press 1985:42439.
4. Baker CJ, Rench MA, Kasper DL. Response to type III polysaccharide in
women whose infants have had invasive group B streptococcal infection.
N Engl J Med 1990;322:1857-60.
5. Farley M, Harvey C, Stull T, et al. A population-based assessment of
invasive disease due to group B streptococcus in nonpregnant adults.
N Engl J Med 1993;328:1807-11.
6. Schwartz B, Schuchat A, Oxtoby M, Cochi S, Hightower A, Broome e.
Invasive group B streptococcal disease in adults. A population-based
study in metropolitan Atlanta. JAMA 1991;266:1112-4.
7. Wessels M, Kasper D. The changing spectrum of group B streptococcal
disease. N Engl J Med 1993;328:1843-4.
8. Wilkinson HW, Eagon RG. Type-specific antigens of group B type Ie
streptococci. Infect Immun 1971;4:596-604.
9. Colman G. Typing of Streptococcus agalactiae (Lancefield group B). Eur
J Clin Microbiol Infect Dis 1988;7:226-31.
10. Baker CJ. Vaccine prevention of group B streptococcal disease. Pediatr
Ann 1993;22:711-4.
II. Paoletti LC, Wessels MR, Rodewald AK, Shroff AA, Jennings HJ, Kasper
DL. Neonatal mouse protection against infection with multiple group
B streptococcal serotypes by maternal immunization with a tetravalent
GBS polysaccharide-tetanus toxoid conjugate vaccine. Infect Immun
1994;62:3236-43.
12. Baker CJ, Barrett FF. Group B streptococcal infections in infants: the
importance of the various serotypes. JAMA 1974;230:1158-60.
13. Wilkinson HW, Facklam RR, Wortham Ee. Distribution by serological
type of group B streptococci isolated from a variety of clinical material
over a five-year period (with special reference to neonatal sepsis and
meningitis). Infect Immun 1973;8:228-35.
JID 1996;173 (February)
Emergence of Serotype V GBS Disease
14. Wilkinson HW. Analysis of group B streptococcal types associated with
disease in human infants and adults. J Clin Microbioll978; 7:176-9.
15. Wenger ill, Hightower AW, Facklam RR, Gaventa S, Broome CV. Bacterial meningitis in the United States, 1986: report of multistate surveillance study. J Infect Dis 1990; 162:1316-23
16. Lancefield RC. Serological differentiation of specific types of bovine hemolytic streptococci (group B). J Exp Med 1934;61:335-49
17. Blumberg HM, Stephens DS, Licitra C, et al. Molecular epidemiology of
group B streptococcal infections: use of restriction endonuclease analysis of chromosomal DNA and DNA restriction fragment length polymerphisms of ribosomal RNA genes (ribotyping). J Infect Dis
1992; 166:574-9.
18. Pitcher DG, Saunders NA, Owen RJ. Rapid extraction of bacterial genomic
DNA with guanidium thiocyanate. Lett Appl Microbiol 1989; 8:151-6.
19. Southern EM. Detection of specific sequences among DNA fragments
separated by gel electrophoresis. J Mol BioI 1975; 98:503-17.
20. Blumberg HM, Kiehlbauch JA, Wachsmuth IK. Molecular epidemiology
of Yersinia enterocolitica 0:3 infections: use of chromosomal DNA
restriction fragment length polymorphisms of rRNA genes. J Clin Microbioll991;29:2368~ 74.
21. Wachsmuth IK, Kiehlbauch JA, Bopp CA, et al. The use of plasmid profiles
and nucleic acid probes in epidemiologic investigations of foodborne,
diarrheal diseases. Int J Food Microbiol 1991; 12:77-90.
22. Murray BE, Singh KV, Heath JD, Sharma BR, Weinstock GM. Comparison of genomic DNAs of different enterococcal isolates using restriction
endonucleases with infrequent recognition sites. J Clin Microbiol
1991;28:2059-63.
23. Tenover FC, Arbeit RD, Georing RV, et al. Interpreting chromsomal DNA
restriction patterns produced by pulsed-field gel electrophoresis: criteria
for bacterial strain typing. J Clin Microbiol 1995;33:2233-9.
24. Larsen JW, Dooley SL. Group B streptococcal infections: an obstetrical
viewpoint. Pediatrics 1993;91:148~9.
25. Centers for Disease Control and Prevention. Prevention of group B streptococcal disease: a public health perspective. Federal Register
1994;59:64764-73.
26. Jafari HS, Schuchat A, Hilsdon R, Whitney C, Toomey K, Wenger ill.
Barriers to prevention of perinatal group B streptococcal disease. Pediatr
Infect Dis J 1995; 14:682-7.
27. Schuchat A, Oxtoby M, Cochi S, et al. Population-based risk factors for
neonatal group B streptococcal disease: results of a cohort study in
metropolitan Atlanta. J Infect Dis 1990; 162:672-7.
28. Schuchat A, Deaver-Robinson K, Plikaytis BD, Zangwill KM, MohleBoetani J, Wenger ill. Multistate case-control study of maternal risk
factors for neonatal group B streptococcal disease. Pediatr Infect Dis J
1994; 13:623~9.
29. Regan JA, Klebanoff MA, Nugent RP. The epidemiology of group B
streptococcal colonization in pregnancy. Obstet Gynecol 1991; 77:60410.
30. Baker CJ, Barrett FF, Yow MD. The influence of advancing gestation on
GBS colonization in pregnant women. Am J Obstet Gynecol
1975; 122:820-3.
31. Schauf V, Hlaing V. Group B streptococcal colonization in pregnancy.
Obstet GynecoI1976;47:719-21.
32. Lancefield RC, McCarty M, Everly WN. Multiple mouse-protective antibodies directed against group B streptococci: special reference to anti-
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
373
bodies effective against protein antigens. J Exp Med 1975; 142:16579.
Anthony BF, Concepcion NF, Concepcion KF. Human antibody to the
group-specific polysaccharide of group B Streptococcus. J Infect Dis
1985; 151:221-6.
Wessels MR, Paoletti LC, Kasper DL, et al. Immunogenicity in animals
of a polysaccharide-protein conjugate vaccine against type III group B
Streptococcus. J Clin Invest 1990;86:1428-33.
Wessels MR, Paoletti LC, Pinel J, Kasper DL. Immunogenicity and protective activity in animals of a type V group B streptococcal polysaccharide-tetanus toxoid conjugate vaccine. j Infect Dis 1995; 171:879-84.
Jelinkova J, Motlova J. Worldwide disfJibution of two new serotypes of
group B streptococci: type IV and-provisional type V. J Clin Microbiol
1985;21:361-2.
Wilkinson HW. Nontypable groap B streptococci isolated from human
sources. J Clin Microbioll977;6:183-4.
Wessels MR, DiFabio JL, Benedi VJ, et al. Structural determination and
immunochemical characterization of the type V group B Streptococcus
capsular polysaccharide. J Bioi Chern 1991;266:6714-9.
Takazawa Y, Tomizawa I. Serotypes and antibiotic susceptibility of group
A and B streptococci clinically isolated in Sapporo in the last five years.
J Jpn Assoc Infect Dis 1991; 65:938-44.
Wibawan IWT, Lammler C, Lautrou Y, Warsa LlC. Serotyping and further
characterization of group B streptococcal isolates from Indonesia. Int J
Med Microbiol Virol Parasitol Infect Dis 1992;277:260-6.
Geslin P, Sissia G, Jelinkova J, Fremaux A, Motlova J. Serotype distribution of group B streptococci isolated from human sources in France
over a 10-year period (1980- I 989). New perspectives on streptococci
and streptococcal infections. Zentralbl Bakt Suppll992;22:484-5.
Chong Y, Lee K, Kwon OH, Nahm CH, Murai T, Inazumi Y. Trend of
isolation and serotypes of group B streptococci in Korea. Yonsei Med
J 1993; 34:78-83.
Hervas J, Benedi V. Neonatal sepsis caused by a new group B streptococcal
serotype (type V) [letter]. J Pediatr 1993; 123:839.
Greenberg D, Ascher D, Yoder B, Hensley D, Heiman H, Keith J. Group
B streptococcus serotype V. J Pediatr 1993; 123:494-5.
Galloway A, Deighton C, Deady J, Marticorena I, Efstratiou A. Type V
group B streptococcal septicaemia with bilateral endophthalmitis and
septic arthritis. Lancet 1993;341:960-1.
Rench M, Baker C. Neonatal sepsis caused by a new group B streptococcal
serotype. J Pediatr 1993; 122:638-40.
Harrison LH, Dwyer DM, Johnson JA. Emergence of serotype V group
B streptococcal infection among infants and adults [letter]. J Infect Dis
1995; 171:513.
Fasola E, Livdahl C, Ferrieri P. Molecular analysis of multiple isolates of
the major serotypes of group B streptococci. J Clin Microbiol
1993; 31:2616-20.
Gordillo ME, Singh KV, Baker CJ, Murray BE. Typing of group B streptococci: comparison of pulsed-field gel electrophoresis and conventional
electrophoresis. J Clin Microbiol 1993; 31:1430-4.
Bingen E, Denamur E, Lambert-Zechovsky N, et al. Analysis of DNA
restriction fragment length polymorphism extends the evidence for
breast milk transmission in Streptococcus agalactiae late-onset neonatal
infection. J Infect Dis 1992; 165:569-73.