Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
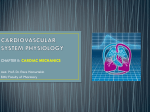
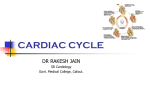
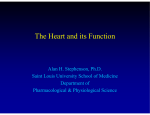
445 Effects of Stroke Volume and Velocity of Ejection on End-Systolic Pressure of Canine Left Ventricle End-Systolic Volume Clamping HlROYUKI SUGA AND KEN-ICHI YAMAKOSHI Downloaded from http://circres.ahajournals.org/ by guest on April 28, 2017 SUMMARY To study the effects of contraction mode on ventricular end-systolic pressure-volume relationship, we compared the end-systolic pressure of isovolumic contraction with that of ejecting contraction at an identical end-systolic volume. The left ventricle of excised cross-circulated canine hearts was fitted with a water-filled balloon. The balloon was connected to a hydraulic pump that allowed the ventricle to contract to a preset constant end-systolic volume (19-37 ml) from a variable end-diastolic volume. At each of control, enhanced, and depressed levels of contractility, differences of end-systolic pressures of steady state isovolumic and ejecting contractions were evaluated while stroke volume and velocity of ejection were widely varied. The end- systolic pressure in the ejecting contraction tended to decrease by 5-15% from that of the isovolumic beat with increases in either stroke volume to 20-25 ml or peak velocity of ejection to about 800 ml/sec. There was no obvious difference in the results at different levels of contractility. The magnitude of the end-systolic pressure depression due to ejection was, however, relatively small as compared to 4-fold changes in end-systolic pressure due to the changes in contractility. We, therefore, conclude that the ventricular end-systolic pressure-volume relationship is affected slightly by ejection, and that this effect is much smaller than the maximal effect of changing contractility on the end-systolic pressure-volume relationship. NO AGREEMENT exists today as to whether the endsystolic pressure-volume relationship of the mammalian ventricle is common to different modes of contraction under a constant contractile state. There are many reports'"8 which indicate that this relationship is common. However, these studies were conducted under conditions in which the stability of the contractile state was not rigorously assessed. We recently have found that the endsystolic pressure-volume relationship curve is virtually the same for both entirely isovolumic contraction and auxobarically ejecting contraction under a stable contractile state.9 In contrast, there are reports which indicate that the end-systolic pressure-volume relationship depends on the mode of contraction.l0> " However, one of these10 did not deal with the pressure-volume relationship using a direct method, and the other" merely indicated a speculative relationship derived from data on the frog heart. Recently, Burns et al.12 reported that the end-systolic pressure-volume relationship of isotonic contractions deviates from that of isovolumic contractions when the isotonic ventricular wall stress is relatively small and stroke volume relatively large. In relation to this problematic issue on the ventricle, some studies'3'14 on papillary muscle preparations showed that their force-length relationship at the end of contraction is independent of the history of contraction, whereas others15"19 indicate its dependency. Recently, the degree of this dependence was shown to be reduced by calcium ions and/or caffeine or tetanus.19 However, these findings were obtained in artificial experimental conditions. Therefore, it is still undetermined whether or not a similar uependence on contraction mode may significantly affect the end-systolic contractile force of the left ventricle ejecting under natural physiological conditions. The previous finding of the uniqueness of the end-systolic pressurevolume relationship9 suggests that the dependence of the end-systolic pressure-volume relationship on the history of contraction, if any, may not be significant, in the canine left ventricle. However, the design of this experiment9 is not appropriate to permit a firm conclusion. To study this problem we designed a pump that can accurately control and measure the instantaneous intraventricular volume and precisely clamp the residual ventricular volume at the end of systole regardless of other parameters of contraction. Connecting this pump to the left ventricle of excised, metabolically supported canine hearts, we studied whether and how much the end-systolic pressure at a given identical end-systolic volume changes, depending on stroke volume and velocity and timing of ejection. From the Department of Physiology, Faculty of Medicine. University of Tokyo, and Institute for Medical and Dental Engineering. Tokyo Medical and Dental University, Tokyo, Japan. Dr. Suga's present address is: Department of Biomedical Engineering. The Johns Hopkins University School of Medicine, Baltimore, Maryland 21205. Address for reprints: Dr. Hiroyuki Suga, Department of Biomedical Engineering, The Johns Hopkins University School of Medicine, Baltimore, Maryland 21205. Received February 17, 1976; accepted for publication October 21, 1976. Methods HEART PREPARATION Fifteen pairs of mongrel dogs (10-19 kg) were anesthetized with sodium pentobarbital (30 mg/kg, iv). From each pair, an excised, cross-circulated heart preparation [128 ± 7 (SE) g] was instituted without stoppage of coronary flow.9 Briefly, a preparation dog was ventilated artificially and a thoracotomy was performed. The left subclavian artery and the right ventricle were cannulated and connected to the femoral arteries and veins, respectively, of a support dog. The heart-lung section was isolated from the 446 CIRCULATION RESEARCH Downloaded from http://circres.ahajournals.org/ by guest on April 28, 2017 systemic circulation by ligature. The pulmonary hili then were ligated and the lungs were cut off. The supported heart was excised from the thorax and suspended over a funnel. The right ventricular cannula was removed. The coronary venous blood flowing out of the ventricle was collected in the funnel and drained back to the support dog's vein. The left atrium was opened and all the chordae tendineae were freed from the mitral valves. A thin latex balloon with an unstressed volume of about 70 ml was placed within the left ventricle via the mitral annulus. A miniature pressure transducer (Konigsberg P-22) was placed inside the balloon, and its wire was pulled out through a stab incision at the apex. The opening of the balloon was fixed to a rigid connecting tube, and the roots of the mitral valves were tied around the neck of the tube with a purse-string suture. An appropriately shaped flange protruding from the end of the connecting tube was positioned to prevent bulging of the balloon into the aorta. The space between the balloon and the endocardium was reduced to a minimum by applying continuous suction through a catheter with multiple holes placed in this space. Since the balloon's membrane was flabby and its unstressed volume was larger than the intraventricular volume, we assumed that the balloon could go into most of the trabecular indentations. Coronary perfusion pressure was kept at a constant level between 75 and 120 mm Hg during each experimental run. The temperature of the coronary perfusion blood was kept at 37°C. END-SYSTOLIC VOLUME CLAMP The intraventricular balloon was connected via a semirigid tube [18-mm inside diameter (i.d.). 10 cm long] to a pump that consisted of a hydraulic and an air housing separated by a rolling seal diaphragm (effective area. 50 cm2) and a piston. The hydraulic housing was filled with water without leaving air bubbles. Compressed air supplied to the air housing actuated the piston of the pump. The movement of the piston was limited by an adjustable mechanical stopper so that the piston sucked intraventricular water only to this stopper. Thus, end-systolic intraventricular volume always was clamped at a preset constant value. Peak velocity of ejection was controlled by changing the compressed air pressure for pulling the piston. The electrocardiogram (ECG) signal from the left ventricular epicardial lead was used to trigger the control valve of the air flow to the pump with an adjustable delay from the Q wave. The delay was varied to shift the onset of ejection. The movement of the piston, which was linearly proportional to changes in the intraventricular volume, was converted to an electric signal by a linear potentiometer installed across the piston rod and cylinder of the pump. Total compliance of the volume measurement-control system including the connecting tube was 0.5 ml/100 mm Hg. PRESSURE AND VOLUME CALIBRATION The miniature pressure transducer was calibrated at the beginning of each experiment against an extracorporeal strain gauge pressure transducer.9 Thermal drift of the VOL. 40, No. 5, MAY 1977 miniature gauge was minimized by reducing the excitation voltage to the strain gauge. In a preliminary test, no thermal drift greater than 2 mm Hg was observed when the gauge was suddenly subjected to a flow of a velocity of 600 cm/sec over a half second in a beaker containing 37°C water. The volume signal was calibrated by the following two steps: First, the gain of the volume signal was calibrated by changing known amounts of water in the pump while the connecting tube to the heart was temporarily closed. Then the piston was pulled firmly to the stopper. Water was sucked out of the intraventricular balloon with a graduated syringe until the balloon was completely collapsed by a highly negative pressure. The electrical signal at this volume of water in the pump was regarded as representing zero intraventricular volume. The amount of water in the syringe indicated the clamped value for end-systolic volume. As long as the total volume of water in the system and the setting of the stopper were unchanged, the same calibration held for the end-systolic volume. With these sensitivity and zero calibrations, the volume tracing was translated into intraventricular water volume. Since the ventricle, even as collapsed as above, still contained the sum of the volumes of such intraventricular devices as the balloon, pressure gauge, etc.. this volume (7 ml) was added to the measured intraventricular water volume to obtain the real intraventricular volume. EXPERIMENTAL PROTOCOL After the preparation stabilized for about 30 minutes an end-systolic volume was chosen such that the isovolumic end-systolic pressure at this volume would be a constant between 80 and 1 20 mm Hg. The end-systolic volume thus chosen was kept unchanged throughout the rest of each experiment regardless of any later change in the isovolumic end-systolic pressure due to a spontaneous change in contractility. The end-systolic volume that was thus determined ranged from 19 to 37 ml among the preparations. Contractility of the left ventricle preparation without any additional inotropic intervention was considered "control." After a series of control runs contractility was enhanced by infusing 10% calcium chloride solution into the coronary artery perfusion tube at such a rate that the isovolumic end-systolic pressure would reach a steady level about 50% higher than control. Contractility was finally reduced by injecting an appropriate amount of 0.1% propranolol into the coronary artery so that the isovolumic end-systolic pressure would fall to a steady level about 50% less than control. Under each of three contractile states, the following three experimental runs were carried out while the endsystolic volume was clamped at the same constant value. The order of these runs at each contractility was randomized. 1. Stroke volume run: Stroke volume was varied from 0 (isovolumic) to 20 or 25 ml in five or six steps by increasing the end-diastolic volume. However, end-diastolic pressure was never allowed to exceed 20 mm Hg. Peak velocity of ejection was set at about 200 ml/sec. The onset of ejection from the Q wave was set at a value between 50 and 75 msec. 447 END-SYSTOLIC PRESSURE-VOLUME RELATIONSH IP/Saga and Yamakoshi volume in the same run. These end-systolic pressures coincided in time from Q wave of ECG with each other (time resolution = 10 msec). Note that the end-systolic pressure of ejecting beats was not necessarily the peak (P,) of the individual pressure curve which could occur before the end of ejection. Finally, the end-systolic pressures (P2) of the ejecting beats were compared with the end-systolic pressure (Plv) of the isovolumic beat in the same run. The velocity of ejection was assessed from the maximal slope of the volume tracing. Results Downloaded from http://circres.ahajournals.org/ by guest on April 28, 2017 FIGURE 1 Schematic illustration of ventricular pressure and volume curves of an isovolumic (solid) and an ejecting contraction (dashed) in the same run. The two curves were superimposed with respect to the time from Q wave of ECG. P, = an earlier peak or hump of the pressure curve which was observed before the end of ejection (T?) in contractions with relatively large stroke volume. P2 = another peak or hump of the pressure curve which was always observed after the end of ejection. Either P, or P2 was the peak pressure of the ejecting beat. Plv = peak isovolumic pressure. T[ = onset of ejection. T 3 = end of systole, where the ejecting pressure curve took P2 and the isovolumic pressure curve took P lv . 2. Ejection velocity run: Peak velocity of ejection was varied from about 100 ml/sec to 700-1.000 ml/sec in four or five steps, while stroke volume and the onset of ejection were kept constant approximately at 15 ml and 50-75 msec, respectively. 3. Ejection timing run: The onset of ejection measured from the Q wave was shifted from about 25 msec to 100125 msec, while stroke volume and peak ejection velocity were kept constant at about 15 ml and 200 ml/sec, respectively. Stability of the preparation during each run is a prerequisite for the present analysis. Therefore, we produced steady state beats of isovolumic contraction before and after each of the three runs to examine whether there was any change in peak isovolumic pressure. When we found a difference less than 5 mm Hg in steady state isovolumic end-systolic pressure values before and after the run. we judged that the preparation was reasonably stable during the run. About 75% of total runs proved to be stable and were subjected to the following analysis. DATA ANALYSIS First, the steady state peak pressure values of the entirely isovolumic contraction was read from strip chart tracings, being designated as the end-systolic pressure (Plv in Fig. 1). Second, in the steady state ejecting beats with different loading conditions in the same run. peak pressure values (P2 in Fig. 1) after the end of ejection (T2 in Fig. 1) were read, and designated as the end-systolic pressure of the ejecting beats. Figure 1 schematically illustrates the relationship between the end-systolic pressures of an isovolumic and an ejecting beat with a relatively large stroke Figure 2 (Panels A. B. and C) shows examples of the simultaneous recordings of left ventricular pressure, volume, and ECG in three different runs under different levels of contractility. The end-systolic volume was always kept constant accurately, as is evident in the second chan^ 500 msec LV 16 B Lv PRESSURE (mmHg) 500 msec 100h- LV VOLUME (ml) J V-- 60 LV PRESSURE 100h (mmHg) 0 LV VOLUME (ml) 20 m 60 i,0Y LV ECG ONSET OF EJECTION (msec) ISV 30 50 70 100 FIGURE 2 Simultaneous tracings of the left ventricular pressure, volume, and ECG. Arrows indicate the end of systole. Panel A shows the data in a stroke volume run under control contractile state. Panel B shows an ejection velocity run under an enhanced contractile state. Panel C shows an ejection timing run under a depressed contractile state. ISV = isovolumic contraction. CIRCULATION RESEARCH 448 Downloaded from http://circres.ahajournals.org/ by guest on April 28, 2017 net of each panel. Heart rate did not change with changes in the mode of contraction. Note that the contour of intraventricular pressure changed markedly with changes in the mode of contraction. As we indicated in previous papers.7- 9 these changes in pressure contour again seem to be largely explainable by the ventricular instantaneous pressure-volume relationship. Therefore, these phenomena were not analyzed in the present study, but the endsystolic pressure-volume relationship was analyzed as follows. Although the contour of the intraventricular pressure was thus markedly altered, the end-systolic pressure values in the ejecting beats changed only slightly with increases in stroke volume, as shown in Figure 2A. Similar trends were generally observed at all the levels of contractility in each preparation. Maximal depression of the endsystolic pressure was observed with stroke volume of 2025 ml. where the percent magnitude of the pressure depression. 100-(Piv - P2)/Piv, varied from 5% to 15% among preparations. Figure 2B shows the recordings in the ejection velocity run. The end-systolic pressure in ejecting beats generally decreased by about 10% when ejection velocity exceeded 200 ml/sec. Figure 2C shows that the end-systolic pressure changed little despite the shift of the onset of ejection over a wide range. Figure 3 is a representative plot of the end-systolic pressures against the three varied parameters under three different levels of contractility in one preparation. In these panels, the isovolumic end-systolic pressure is plotted against the zeros of the abscissas. Similar decreases in the end-systolic pressure with increases in stroke volume and ejection velocity were observed at all three different levels of contractility. Figure 4 is a su.nmary of statistical analyses of the data from all the preparations. End-systolic pressure values in ejecting beats were converted to percentage with respect to the isovolumic end-systolic pressure in each run. Data from different levels of contractility were pooled together. Since abscissa values for a given type of run were not always identical among separate runs, the abscissa was divided into several ranges and corresponding data within a given range were pooled together. Each data point represents the mean percent value of the end-systolic pressure ± 1 SEM of all the preparations at a specified abscissa range of parameter. The plots show that in general endsystolic pressure decreased with increases in stroke volume and peak velocity of ejection, and the decrease is on an average about 10% at most. The shift of onset of ejection had little effect on the end-systolic pressure except when the onset was very early or very late during systole. VOL. 0 500 1000 PEAK VELOCITY OF EJECTION ml /sec SIBOKE VOLUME 40. No. 5. MAY ONSET OF EJECTION 1977 msec FIGURE 3 Graphs showing the changes in end-systolic pressure with stroke volume (A), peak velocity of ejection (B), and onset of ejection (C) under three levels of contractile state in the same preparation. The present analysis indicated that the end-systolic intraventricular pressure that was developed at a constant end-systolic intraventricular volume slightly decreased with increases in either stroke volume or peak velocity of ejection. This is the first direct experimental evidence showing this dependency. The observation of Burns et al.12 may appear somewhat similar to the present findings. However, they converted their ventricular pressure and volume data into ventricular wall force and fiber length and observed similar dependence of end-systolic contractile force on the amount of shortening. Therefore, it is difficult to evaluate the end-systolic pressure and volume relationship from their published data. Nevertheless, it is interesting to note that their degree of depression of endsystolic contractile force by ejection was about 11 % at most, which is close to our present observation. They compared the end-systolic contractile force of a steady state ejecting contraction with that of a steady state isovolumic contraction at a given end-systolic fiber length or volume. They did not compare end-systolic contractile 100 90 5 10 15 20 25 STROKE VOLUME ml LU % 100 in lU or, tr so Q. 100 200 400 800 PEAK dV/dt ml/sec 10 • 100 z UJ Discussion The design of the present experiments enabled us to study precisely whether the end-systolic pressure at a given constant end-systolic volume depends on the mode of the contraction of the ventricle. Since the end-systolic pressure of the ejecting mode was compared with that of the isovolumic mode at the same end-systolic volume (paired experiment) we could use the paired f-test which improved the precision of comparison.20 90 0 25 50 75 100 125 ONSET OF EJECTION msec FIGURE 4 Summary of statistical analyses of the percentile changes of end-systolic pressure at the same end-systolic volumes vs. stroke volume, peak velocity of ejection, and onset of ejection. The abscissas show the ranges and their central values where the end-systolic pressure data were pooled together. Solid circles and bars indicate the mean and the standard error of the mean. Asterisks show P < 0.05 by t-test as compared to 100%. END-SYSTOLIC PRESSURE-VOLUME RELATIONSHIP/Suga and Yamakoshi Downloaded from http://circres.ahajournals.org/ by guest on April 28, 2017 forces at the same end-systolic fiber length or volume among several ejecting beats with different stroke volumes. Therefore, it cannot be concluded from their data that the depression of end-systolic contractile force is dependent on stroke volume. Our study demonstrates this dependence. Here we discuss several possible mechanisms responsible for the observed depression of the end-systolic pressure in ejecting beats. Quick shortening of heart muscle has an uncoupling effect and this is one of the possible mechanisms. Brady21 found that in rabbit papillary muscle the peak isometric tension is substantially (30%) greater than the isotonic force level at the same end-systolic muscle length. He ascribed this to the uncoupling effect. Taylor15 observed a similar phenomenon in cat papillary muscle. However. Downing and Sonnenblick13 found that the isotonic and isometric length-tension relations could be superimposed in cat papillary muscle. Sonnenblick.14 Brutsaert and Sonnenblick.17 and Brutsaert et al.22 observed only a minor difference among the end-systolic fiber lengths of different beats loaded with the same isotonic force and shortening from different initial lengths. More recently. Bodem and Sonnenblick19 reported that the degree of mechanical damping and the sarcoplasmic calcium level critically affected the magnitude of the uncoupling effect. Temperature seems to be another factor which modifies the effect.19 These observations were, however, obtained in excised, artificially perfused papillary muscle preparations contracting under unphysiological conditions that were different among the investigators. Although it remains to be known whether such an uncoupling effect has any significant role for natural ventricular contraction, we cannot deny this possibility as a mechanism of the present findings. Peak isovolumic pressures at the same ventricular volume were the same before and after each experimental run. However, the contractility may have been altered in ejecting beats even in such stable preparations for the following reason: Contractility is known to change to another level when a mode of contraction.23"25 fiber length.26 or shortening velocity23 is altered in excised myocardium. These effects have been suspected to be due to changes in sarcoplasmic calcium level or to viscoelastic properties of myocardium.23"26 A similar phenomenon could be responsible for the present findings. However, there is no study in which the end-systolic fiber length of myocardium was clamped at a constant length and effects of a history of contraction on the steady state level of contractility was assessed. A third possibility is that cardiac oxygen consumption increases with increases in stroke volume or ejection velocity and consequently oxygen supply becomes inadequate for load. However, this possibility seems less likely since coronary vessels haye marked autoregulatory capability under constant perfusion pressure, as shown by Monroe et al.27 A fourth possibility is that there is some viscous resistance againt deformation among myocardial fibers and layers and this may impede their shortening and cause the depression of pressure. Such an effect may not be a serious factor in papillary muscles, where the fibers are in parallel 449 and contract synchronously. Within the ventricular wall, however, fibers and layers are arranged in a complex manner28 and contract asynchronously.29 producing shear and bending force among them. Although there is no more volume change at the end of systole, the ventricular dimensions may still be changing because of the asynchrony. We cannot evaluate this possibility quantitatively at present because of the lack of published data. If ejection per se increased asynchrony of ventricular contraction, it could cause the pressure depression. However, the observed depression was not accompanied by a widening of the pressure curve which would be expected as a result of a greater asynchrony.29 Therefore, we probably can negate this possibility. It also is unlikely that the ventricular wall inertia causes the observed depression of pressure .30 The ejection had already been completed and there was no more net flow out of the ventricle at the end of systole in ejecting beats. Therefore, kinetic energy of the ejected flow could not reduce the measured pressure at the end of systole. However, if there remained some local flow within the ventricular cavity, especially in the vicinity of the miniature pressure transducer, even after the end of ejection, it could reduce the measured pressure by the amount equal to the kinetic energy of the flow (Bernoulli principle).31 However, it is difficult to consider the existence of such a local flow that holds kinetic pressure large enough to explain the observed pressure depression, since a kinetic pressure of 10 mm Hg requires a flow velocity of about 300 cm/sec.31 Whatever the underlying mechanism might be, the degree of the end-systolic pressure depression in ejecting contraction was at most 10% on the average. The range of stroke volume examined in this experiment is wide enough to cover the physiological range of the stroke volume in dogs of comparable size (10-25 ml in 10- to 20-kg dogs).30 The range of velocity of ejection is more than the physiological range, according to the measured value (571 ml/ sec) under maximal stimulation of cardiac sympathetic nerves.30 The onset of ejection was also varied widely enough to cover the physiological range. Consequently, we speculated that the degree of the depression of endsystolic pressure in ejecting beats in normal physiological circumstances will not exceed the present observation. The depression of the end-systolic pressure is. however, relatively small as compared to changes in the end-systolic pressure due to experimentally attainable changes in contractility. In the present experiment, the end-systolic pressure with the same volume was varied easily by ±50% around control level by calcium and propranolol. respectively. In our previous studies7-9l32 the end-systolic pressure at the same end-systolic volume increased by as much as 300% from control with administration of catecholamines to the heart or a nearly maximal stimulation of the cardiac sympathetic nerves. Compared with these percentages, the percentile change in end-systolic pressure due to ejection is almost negligible. Acknowledgments We are indebted to Dr. Kiichi Sagawa for critical comments and encouraging advice in the preparation of this manuscript. CIRCULATION RESEARCH 450 References Downloaded from http://circres.ahajournals.org/ by guest on April 28, 2017 1. Cross CE, Rieben PA, Salisbury PE: Influence of coronary perfusion and myocardial edema on pressure-volume diagram of left ventricle. Am J Physiol 201: 102-108, 1961 2. Monroe RG, French GN: Left ventricular pressure-volume relationships and myocardial oxygen consumption in the isolated heart. Circ Res 9: 362-374, 1961 3. Urshell CW, Covell JW, Sonnenblick EH, Ross J Jr, Braunwald E: Myocardial mechanics in aortic and mitral valvular regurgitation; concept of instantaneous impedance as a determinant of the performance of the intact heart. J Clin Invest 47: 867-883, 1968 4. Taylor RR, Covell JW, Ross J Jr: Volume-tension diagrams of ejecting and isovolumic contractions in left ventricle. Am J Physiol 216: 1097-1102, 1969 5. Suga H: Time course of left ventricular pressure-volume relationship under various extents of aortic occlusion. Jap Heart J 11: 373-378, 1970 6. Suga H, Sagawa K: Mathematical interrelationship between instantaneous ventricular pressure-volume ratio and myocardial force-velocity relation. Ann Biomed Eng 1: 160-181, 1972 7. Suga H, Sagawa K, Shoukas AA: Load independence of the instantaneous pressure-volume ratio of the canine left ventricle and effects of epinephrine and heart rate on the ratio. Circ Res 32: 314-322,1973 8. Mahler F, Covell JW, Ross J Jr: Systolic pressure-diameter relations in the normal conscious dog. Cardiovasc Res 9: 447-455, 1975 9. Suga H, Sagawa K: Instantaneous pressure-volume relationship and their ratio in the excised, supported canine left ventricle. Circ Res 35: 117-126, 1974 10. Rosenblueth A, Alanis J, Rubio R: Some properties of the mammalian ventricular muscle. Arch Int Physiol Biochim 67: 276-293, 1959 11. Schneider M: Einfuehrung in die Physiologie des Menschen. Berlin, Springer-Verlag, 1964, pp 86-91 12. Burns JW, Covell JW, Ross J Jr: Mechanics of isotonic left ventricular contractions. Am J Physiol 224: 725-732, 1973 13. Downing SE, Sonnenblick EH: Cardiac muscle mechanics and ventricular performance; force and time parameter. Am J Physiol 207: 705715, 1964 14. Sonnenblick EH: Determinants of active state in heart muscle; force, velocity, instantaneous muscle length, time. Fed Proc 24: 1396-1409, 1965 15. Taylor RR: Active length-tension relations compared in isometric afterload and isotonic contractions of cat papillary muscle; their dependence on inotropic state. Circ Res 26: 279-288, 1970 16. Brady AJ: Active state in cardiac muscle. Physiol Rev 48: 570-600, 1968 VOL. 40, No. 5, MAY 1977 17. Brutsaert DL, Sonnenblick EH: Force-velocity-length-time relations of the contractile elements in heart muscle of the cat. Circ Res 24: 137-149, 1969 18. Brutsaert DL, Claes VA, Donders JJH: Effects of controlling the velocity of shortening on force-velocity-length and time relations in cat papillary muscle. Circ Res 30: 310-315, 1972 19. Bodem R, Sonnenblick EH: Deactivation of contraction by quick releases in the isolated papillary muscle of the cat; effects of lever damping, caffeine, and tetanization. Circ Res 34: 214-225, 1974 20. Snedecor GW, Cochran WG: Statistical Methods. Ames, Iowa State University Press, 1971, p 97 21. Brady AJ: Mechanics of isolated papillary muscle. In Factors Influencing Myocardial Contractility, edited by RP Tanz, F Kavaler, J Robens. New york, Academic Press, 1967, pp 53-64 22. Brutsaert DL, Claes VA, Sonnenblick EH: Effects of abrupt load alterations on force-velocity-length and time relations during isotonic contractions of heart muscle; load clamping. J Physiol (Lond) 216: 319-330, 1971 23. Parmley WW, Brutsaert DL, Sonnenblick EH: Effects of altered loading on contractile events in isolated cat papillary muscle. Circ Res 24: 521-532, 1969 24. Kaufmann RL, Lab MJ, Henneckes R, Krause H: Feedback interaction of mechanical and electrical events in the isolated mammalian ventricular myocardium (cat papillary muscle). Pfluegers Arch 324: 100-123, 1971 25. Jewell BR, Rovell JM: Influence of previous mechanical events on the contractility of isolated cat papillary muscle. J Physiol (Lond) 235: 715-740,1973 26. Parmley WW. Chuck L: Length-dependent changes in myocardial contractile state. Am J Physiol 224: 1195-1199, 1973 27. Monroe RG, Gamble WJ, LaFarge CG, Vatner SF: Homeometric autoregulation. In The Physiological Basis of Starling's Law of the Heart. Ciba Found Symp (new series) 24: 257-277, 1974 28. Streeter DD, Hanna WT: Engineering mechanics for successive states in canine left ventricular myocardium. II. Fiber angle and sarcomere length. Circ Res 33: 656-664, 1973 29. Osadjan CE, Randall WC: Effects of stellate ganglion stimulation on left ventricular synchrony in dogs. Am J Physiol 207: 181-186. 1964 30. Tallarida RJ, Rusy BF, Loughname MH: Left ventricular wall acceleration and the law of Laplace. Cardiovasc Res 4: 217-223. 1970 31. McDonald DA: Blood Flow in Arteries. Baltimore, Williams & Wilkins, 1974, pp 36-37, 203-204 32. Suga H, Sagawa K, Kostiuk DP: Controls of ventricular contractility assessed by pressure-volume ratio, E^,,. Cardiovasc Res 10: 582-592. 1976 Effects of stroke volume and velocity of ejection on end-systolic pressure of canine left ventricle. End-systolic volume clamping. H Suga and K Yamakoshi Downloaded from http://circres.ahajournals.org/ by guest on April 28, 2017 Circ Res. 1977;40:445-450 doi: 10.1161/01.RES.40.5.445 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1977 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/40/5/445 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/