Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
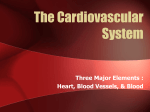
Cell‐based description of ventricular contraction in a model of the human cardiovascular system 1 2 2 S. Kosta , J. Negroni , E. Lascano , P. C. Dauby 1 1 University of Liège, GIGA - Cardiovascular Sciences, Belgium 2 Department of Compara�ve Cellular end Molecular Biology, Favaloro University, Buenos Aires, Argen�na A mul�scale model of the cardiovascular system is presented, where hemodynamics is described by a lumped parameter model, while heart contrac�on is described at the cellular scale. Pulmonary circula�on Passive chamber: Ac�ve chamber: Electrophysiology elastance Pulmonary artery Calcium kine�cs Mechanical contrac�on Pulmonary vein Thick filament pressure volume Q Thin filament Flow through the vessels: Po R Pi Parallel element ACTIVE Right Le� ventricle CONTRACTION ventricle Volume varia�on: Vena cava From cell to ventricle Qout Qin V Aorta Systemic circula�on Cardiac valve: Results Baseline End-systolic elastance: a good index of cardiac contrac�lity ? Par�cular a�en�on was paid to the sarcomere length, which must vary between physiological extremes. A good cardiac contrac�lity index should only vary with inotropy and not with load. End-systolic elastance (Ees) is the gold standard for assessing cardiac contrac�lty, but with our model we show that this index is load-dependent. Load varia�on Pressure-volume loops are correctly reproduced, as well as the different flows and pressures �me evolu�on. Hemorrhage (preload decrease) Heart failure Ees calcula�on Rmt increase (preload decrease) Rsys increase (a�erload increase) Results A prolonged ac�on poten�al, a lower intracellular calcium and a weaker produced force are characteris�c symptoms of heart failure. This leads to smaller pressurevolume loops. Ees is calculated with a linear regression over the three first endsystolic points of the PV loop Conclusion Acknowledgements Our mul�scale model of the human cardiovascular system is able to reproduce baseline results at both scales (cellular and hemodynamic). It can also reproduce pathological behaviors that originate at the cellular scale, like heart failure. It also indicates that the end-systolic elastance is not loadindependent, as o�en assumed in many CVS models using the varying elastance to describe heart contrac�on. P. D. acknowledges for FRS-FNRS travel support. Contact [email protected]