Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
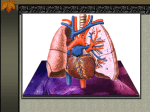
ANPS020 March 28, 2012 PULMONARY VENTILATION Maximum intrapulmonary pressure -maximum straining, a dangerous activity, can increase range --from -30 mmHg to +1—mmHg Weight lifter breath out (exhale) as they life (expert pressure) MODES OF BREATHING Respiratory movements are classified by pattern of muscle activity into: Quiet breathing (eupnea) -involves active inhalation and passive exhalation -diaphragmatic breathing or deep breathing -costal breathing or shallow breathing Forced Breathing (hyperpnea) -involves inhalation and exhalation -assisted by accessory muscle -maximum levels occur in exhaustion RESPIRATORY RATES AND VOLUMES Respiratory system adapts to changing oxygen demands by varying: -the number of breaths per minute (respiratory rate = f, 12-16) -the volume of air moved per breath (tidal volume; 500ml) = VT The respiratory minute volume = VE -Amount of air moved per minute -is calculated by f x VT = VE -respiratory rate (per minute) x tidal volume Anatomic Dead Space = VD -Only a part of respiratory minute volume reaches alveolar exchange surfaces -volume of air remaining in conducting passages in anatomic dead space ALVEOLAR VENTILATION =VA Amount of air reaching alveoli each minute -remember dead space (air already in lung) Calculated as: -respiratory rate x (tidal volume – anatomic dead space VA = f x (VT – VD) DEFINITIONS Resting tidal volume: Amount of air one can move in or out of lungs in single respiratory cycle (resting conditions) Expiratory reserve volume (ERV): amount of air one can voluntarily expel after completed normal respiratory cycle] Residual Volume: amount of air remaining in lungs after maximal exhalation (1200 males; 1100 females) -Minimal volume – amount of air left if lungs collapsed Inspiratory reserve volume (IRV): amount of air one can take in over and above tidal volume Inspiratory capacity: tidal volume + inspiratory reserve volume Functional residual capacity: amount of air remaining in lungs after a quiet respiratory cycle Vial capacity: maximum amount of air one can into or out of lungs in a single respiratory cycle Totally lung capacity: Total volume of lungs = vital capacity and residual capacity (avg = 6000ml males, 4200 females) GAS EXCHANGE How do you get oxygen from the air into your cells? -principle of diffusion: high pressure to low pressure -air is composed of many gases -gases dissolve into liquids Respiratory – Cardiovascular systems interact -RBCs (in blood vessels) an carry O2 INTRODUCTION TO HAS EXCHANGE Respiration refers to two integrated processes -external respiration --includes all processes involved in exchanging O2 and CO2 with the environment *Movement of O2 from air to alveoli to blood (in lungs then system) to interstitium -internal respiration --Also called cellular respiration --involves the uptake of O2 and production of the CO2 within individual cells Movement of O2 from interstitum into cells -Cellular respiration –use of O2 in the cells BLOOD SUPPLE TO THE LUNGS Blood supple to the lungs -#1 Pulmonary artery: (deoxygenated blood) -from the right ventricle -follow the bronchial…tree to alveoli #2 Bronchial arteries – capillaries -provide oxygen and nutrients to tissues of conducting passageways of lung, CT and pleura GAS EXCHANGE Occurs between alveolar air and blood Across the respiratory membrane (blood-air barrier) Into plasma and then Into hemoglobin Depends on -Diffusion of molecules between gas or liquid -partial pressures of the gases The Gas Laws: Diffusion occurs in response to concentration gradients Movement is high to low concentration Rate of diffusion depends on physical principles or gas laws GAS EXCHANGE Composition of Air Nitrogen s about 78.6% Oxygen is about 20.9% Water vapor is about 0.5% Carbon dioxide is about 0.04% Air in a container – has a pressure All molecules in air contribute to the total pressure --each gas has a partial pressure --all partial pressures together add up to 760 mmHg Dalton’s Law and Partial Pressure )abbreviate Px Atmospheric pressure (760 mmHg) -produced by air (gas) molecules bumping to the container wall -more bumping = more pressure Each gas contributes to the total pressure -in proportion to its number of molecules (Dalton’s Law)... Air: Nitrogen > Oxygen > Carbon Dioxide Henry’s Law When gas under pressure comes in contact with liquid (plasma0 -gas dissolves in liquid until equilibrium is reached At a given temperature -amount of a gas in solution is proportional to partial pressure of that gas Gas Content The actual amount of a gas in solution (at given partial pressure and temperature) depends on the solubility of that gas in that particular liquid Solubility in Blood Fluids (plasma) CO2 is very soluble O2 is less soluble N2 has very low solubility GAS EXCHANGE Normal Partial Pressure In pulmonary vein plasma (with O2) P CO2 = 40mmHg P O2 = 100 mmHg P N2 =573mmHg Diffusion and the Blood Air barrier -direction and rate of diffusion of gases across the respiratory membrane is determined by different partial pressures and solubilities VARIABLES IN GAS EXCHANGE Efficiency of gas exchange is due to: Substantial differences in partial pressure across the respiratory membrane -diffusion gradients required Distances involved in gas exchange are short O2 and CO2 is lipid soluble Totally surface area is large -more chances for diffusion -need more walls – hence more surface area Blood flow and airflow are coordinated --blood takes O2 away from alveoli GAS EXCHANGE Ineffiencies in gas exchange may occur: Substantial differences in partial pressure across the respiratory membrane -skiing in Colorado (lower oxygen in mountains) -receiving O2 in the hospital Distances involved in gas exchange are short -fibrosis (increased CT = increased wall thickness O2 and CO2 are lipid soluble -always true… Total surface area is large -emphysema – surface area is decreased Blood flow and airflow are coordinated -congestive heart failure ALVEOLI TO BLOOD O2 & CO2 Blood arriving in (to lungs) pulmonary arteries has Low P O2 --*deoxygenated blood from the system; right side of the heart High P CO2 The concentration gradient causes O2 to enter blood Co2 to leave blood --* P O2 is high in alveolar space, P CO2 is low Rapid exchange allows blood and alveolar air to reach equilibrium GAS EXCHANGE MIXING Oxygenated blood mixes with deoxygenated blood form conducting passageways Lowers the PPO2 of blood entering systemic circuit (drops to about 95 mmHg) BLOD TO CELLS Interstitial fluid in blood P O2 40 mmHg = 95 mmHg PCO2 45 mmHg = 40 mmHg Concentration gradient in peripheral capillaries is opposite of lungs - O2 diffuses out of blood - CO2 diffuses into blood GAS EXCHANGE A PROBLEM Gas pickup and delivery Blood plasma cannot transport enough O2 or CO2 to meet physiological needs GAS TRANSPORT: RBC RBC with hemoglobin -transports O2 and CO2 from, peripheral tissues -Remove O2 and CO2 from plasma, allows gases to diffuse into blood Blood (cells and plasma) carries O2 1. Dissolved in plasma 2. Attaché to heme groups in RBCs Hb + O2 HbO2 GAS TRANSPORT: RBCS Oxygen transport O2 binds to iron ions in hemoglobin (Hb) molecules -in a reversible Each RBC has about 280 million Hb molecules -each binds to four oxygen Hemoglobin Saturation The percentage of heme units in a hemoglobin molecule -that contain bound oxygen