Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
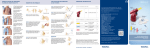
Sni Valley Fire Protection District Standard Operating Guidelines General EZ-IO Adult and Pediatric Intraosseous 01 January 2007 Indications 1. Intravenous fluids or medications needed and a peripheral IV cannot be established in 2 attempts or 90 seconds AND in patients who exhibit 1 or more of the following: a) An altered mental status (GCS of 8 or less). b) Respiratory compromise (SAO2 80 % after appropriate oxygen therapy, respiratory rate < 10 or > 40 a minute). c) Hemodynamic instability (systolic BP of < 90). *Use the pediatric needle if the patient conforms to the Browslow tape. Contraindications 1. Fracture of the tibia or femur (consider alternative tibia). 2. Previous orthopedic procedures (IO within 24 hours, knee replacement, consider alternate tibia). 3. Pre-existing medical condition (tumor near site or peripheral vascular disease). 4. Infection at insertion site (consider alternate site). 5. Inability to locate landmarks (significant edema). 6. Excessive tissue at insertion site. Page 1 of 3 Considerations Flow rates Due to the anatomy of the IO space you will note flow rates to be slower than those achieved with IV catheters. a) Ensure the administration of a 10 ml (5 ml for pediatric) rapid bolus with a syringe. b) Use a pressure bag for continuous infusion. Locations There are three anatomical landmarks for adult and pediatric for the insertion site that the EZ-IO user MUST be familiar with before using the device. The first landmark is the patella. To locate it, feel the front surface of the leg just below the femur or thigh bone for a floating bony structure. Second landmark is approximately 2 fingers width below the patella. It is the tibial tuberosity, a round oval elevation of bump on the front surface of the tibia or lower leg. Now, one finger width medial of the tibial tuberosity is our final landmark. An alternative location is the humeral head mid-shaft, expose shoulder and adduct humerus (place the patient’s arm against the patient’s body) resting the elbow on the ground. Forearm resting on the abdomen (with the patient in this position you may immediately note the humeral head on the anterior –superior aspect of the upper arm or anterior-lateral shoulder. Palpate and identify the mid-shaft humerus and continue palpating toward ht proximal aspect of humeral head. As you near the shoulder you will note a small protrusion. This is the base of the greater tubercle insertions site. With the opposite hand you may consider “pinching” the anterior and inferior aspects of the humeral head while confirming the identification of the greater tubercle. This will ensure that you have identified the midline of the humerus itself. Pain Insertion of the EZ-IO in conscious patients caused mild to moderate discomfort and is usually no more painful than a large bore IV. Technique 1. Wear you BSI. 2. Determine EZ-IO indications. 3. Rule out contraindications. Page 2 of 3 4. Locate insertion site. 5. Cleanse insertion site using aseptic technique. 6. Prepare the EZ-IO driver and needle set. 7. Stabilizes leg and insert EZ-IO needle set- confirm you can still visualize the 5mm mark. 8. Remove EZ-IO driver from needle set, secure stylet. 9. Remove stylet from needle set, secure stylet. 10. Confirm placement. 11. Connect primed EZ- connect. 12. Flush the EZ-IO catheter rapidly with 10 ml of normal saline using a 10 ml syringe. 13. Place a pressure bag on the solution being infused. 14. Begin infusion. 15. Dress site, secure tubing and apply wristband. 16. Monitor EZ-IO site and patient condition. Page 3 of 3