Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Transmission (medicine) wikipedia , lookup
Bacterial morphological plasticity wikipedia , lookup
Human microbiota wikipedia , lookup
Triclocarban wikipedia , lookup
Germ theory of disease wikipedia , lookup
Gastroenteritis wikipedia , lookup
Infection control wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Globalization and disease wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Bioterrorism wikipedia , lookup
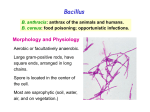
Bacillus Dr. Batool General Concepts: The family Bacillaceae, consisting of rod-shaped bacteria that form endospores, has two principal subdivisions: 1- Anaerobic spore-forming bacteria of the genus Clostridium. 2- Aerobic or facultative anaerobic spore-forming bacteria of the genus Bacillus. General Characteristics of Bacillus: Rod-shaped, Gram-positive bacteria. Endospore-forming aerobic or facultative anaerobic. The spores are resistant to heat, cold, radiation, desiccation, and disinfectants. Are ubiquitous, in soil, water, and airborne thermophilic (< 75°C) and psychrophilic (>5-8°C), also can flourish at extremes of acidity & alkalinity (pH 2 to 10). Catalase positive (rapidly differentiate from Clostridium). Types of Bacillus: Bacillus anthracis , Bacillus cereus, Bacillus stearothermophilus, Bacillus subtilis, Bacillus larvae. Bacillus anthracis Human pathogen isolation also considered zoonosis. Anthrax: is primarily a disease of herbivores. Humans acquire it as a result of contact with infected animals or animal products. In humans the disease takes one of three forms depending on the route of infection (Transmission): 1- Cutaneous anthrax result from contact human skin with spores or infected animals & animals products. which accounts for more than 95% of cases worldwide, results from infection through skin lesions. 1 Bacillus Dr. Batool 2- Gastrointestinal anthrax result when spores are ingested. usually in infected meat; and intestinal anthrax is analogous to cutaneous anthrax but occurs on the intestinal mucosa. 3- Pulmonary anthrax result when inhalation of dust containing anthrax spores inhaled. It is usually an occupational disease, such as in persons who handle or sort contaminated wools. Gastrointestinal and pulmonary anthrax are both more dangerous than the cutaneous form because they are usually identified too late for treatment to be effective. Virulence factors: 1-Capsule: is antiphagocytic and helps the anthracis to evade the immune system of the host. 2-The product of exotoxin: This toxin consists of three proteins: protective antigen (PA), lethal factor (LF) , and edema factor (EF). Cutaneous Anthrax human: cases are cutaneous infections 95% to 5 days after contact cause 1 small pruritic, 2 non-painful papule at inoculation site, papule develops into 3 hemorrhagic vesicle & 4 ruptures slow-healing painless 5 ulcer covered with black eschar surrounded by 6 edema Infection may spread to7 lymphatic / local adenopathy 8 septicemia may develop mortality in untreated cutaneous anthrax. Gastrointestinal (Ingestion) Anthrax: Virtually 100% fatal, abdominal pain, vomiting of blood, and severe bloody diarrhea. Inhalation Anthrax: Virtually 100% fatal, pneumonic meningitis may complicate with cutaneous anthrax and inhalation forms of disease (pharyngeal anthrax, fever pharyngitis and neck swelling). Anthrax spores, which are transported to the 1 regional lymph nodes 2 Bacillus Dr. Batool where they germinate, multiply, and produce toxin, and characterized by2 pleural effusions 3 dyspnea, 4 cyanosis, 5 stridor, 6 and shock. Epidemiology of Bacillus anthracis: The ultimate reservoir of B. anthracis is contaminated soil, in which spores remain viable for long periods. Herbivores, the primary hosts, become infected when foraging in a contaminated region. Enzootic in certain foreign countries (e.g., Turkey, Iran, Pakistan and Sudan). Bacillus cereus - Saprophytic, heat resistant spores. - Heat and acid stable toxin (Emetic syndrome bacillus). - Heat labile enterotoxin (Diarrheal disease). Virulence factor: include : Toxins and Enzymes TOXINS 1- One emetic toxin(ETE): This toxin is highly resistant to pH(2-11), to heat, and to proteolytic cleavage. 2- Three different enterotoxins: The first enterotoxins (HBL) haemolysin BL is also a hemolysin. the second enterotoxin (Nhe) nonhemolytic enterotoxin is not a hemolysin. The third enterotoxin (EntK) is a single component protein that has not been shown to be involved in food poisoning. All three enterotoxins are cytotoxic and cell membrane active toxins that will make holes or channels in membranes. ENZYMES Tissue destruction is mediated by cytotoxic enzyme including: 3 Bacillus Dr. Batool Cereolysin. Phospholipase C (This enzyme may have a secondary role in ocular infections). Bacillus cereus causes two types of food-borne illnesses: 1- One type is characterized by:- nausea and vomiting and abdominal cramps and has an incubation period of 1 to 6 hours. This is the "short-incubation" or emetic form of the disease is caused by a heat-stable emetic toxin(ETE). It resembles Staphylococcus aureus (staph) food poisoning in its symptoms and incubation period. 2-Second type is manifested primarily by: abdominal cramps and diarrhea following an incubation period of 8 to 16 hours. Diarrhea may be a small volume or profuse and watery. This type is referred to as the "long-incubation" or diarrheal form of the disease, and it resembles food poisoning caused by Clostridium perfringens. In either type, the illness usually lasts less than 24 hours after onset. In a few patients symptoms may last longer. The long-incubation form of illness is mediated by the heat-labile diarrheagenic enterotoxins (enterotoxin Nhe and /or hemolytic enterotoxin HBL). B. cereus may occasionally produce disease in immune compromised humans (eg, meningitis, endocarditis, endophthalmitis, conjunctivitis, or acute gastroenteritis). Epidemiology of Bacillus cereus : 1- Ubiquitous, in soil. People at risk include those who consume food contaminated with bacterium (e.g., rice, meat ,vegetable). 2-With penetration injuries (e.g., to eye). 3-Receive intravenous injection. 4 Bacillus Dr. Batool Bacillus subtilis This species is commonly found in the upper layers of the soil, and evidence exists that B. subtilis is a normal gut commensal in humans. The number of spores found in the human gut was too high to be attributed solely to consumption through food contamination. ΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩΩ Diagnosis: Cutaneous anthrax is diagnosed on the basis of the characteristic papule (early) or eschar (later) with extensive surrounding edema. History of exposure to animals or their products. Also is confirmed by observation of characteristic encapsulated bacilli in polychrome methylene blue-stained smears of blood, exudate, lymph and cerebrospinal fluid. Culture. ELISA for capsule antigens anthrax is (95% sensitivity). Control: Anthrax: Control in animals is essential for control in humans. In endemic areas, animals that die suddenly should be handled cautiously and livestock should be vaccinated annually. A human vaccine is available for individuals in high-risk occupations. Vaccine (controversial) Laboratory workers Employees of mills handling goat hair Active duty military members Food poisoning is controlled by Adequate cooking. Avoidance of recontamination of cooked food, and proper storage (efficient refrigeration). 5 Bacillus Dr. Batool Treatment: Anthrax is readily treated with antibiotics (e.g., penicillin, tetracycline, chloramphenicol, gentamicin, or erythromycin). Treatment is with non-ß-lactam antibiotics for Gram-positive bacteria. Antimicrobial Susceptibility of Bacillus spp Isolates DRUG ORGANISM Bacillus cereus Imipenem, Vancomycin, Ramoplanin,Teicoplanin, Chloramphenicol, Clindamycin, Gentamicin, Trovafloxacin, Levofloxacin, Ciprofloxacin, Norfloxacin, Ofloxacin, Sparfloxacin. Non - B. cereus Penicillin, Mezlocillin, Oxacillin, Cefazolin, Cefotaxime, Imipenem, Vancomycin, Chloramphenicol, Clindamycin, Ciprofloxacin. Spores may be: 1. Central. 2. Sub-terminal,(eg. Clostridium perfringens). 3. Oval and terminal, resembling a tennis racket. 4. Spherical and terminal, giving a drumstick appearance (Clostridium tetani) Medical Importance of Bacterial Spores Important features of Spores Medical Implications Spores are highly resistant to heating; spores are not killed by boiling (100OC) but are killed at 121OC. Medical supplies must be heated to 121oC for at least 15 minutes to be sterilized. Spores are highly resistant to many chemicals, including most disinfectants. Only solution designated as sporicidal will kill spores. Spores can survive for many years in soil and other inanimate objects. Wound contaminated with soils can be infected with spores and cause diseases such as tetanus, gas gangrene. Spores do not exhibit measurable metabolic activity. Antibiotics are ineffective against spores. Spores formed only when nutrients are insufficient. Spores are not found at the site of infection because nutrients are not limiting. 6 Bacillus Dr. Batool References: 1- Jawetz, Melnick, & Adelberg’s.( 2013). Medical Microbiology (Twenty-Sixth Edition). 2- Ray, C.G., ed. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. 7