Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
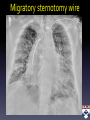
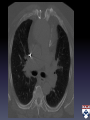
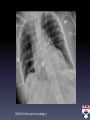
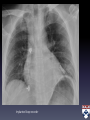
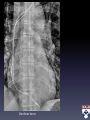
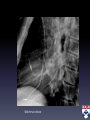
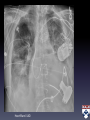
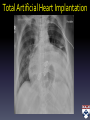
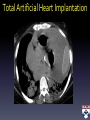
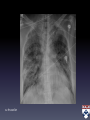
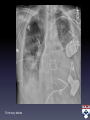
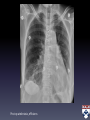
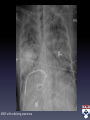
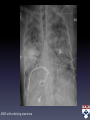
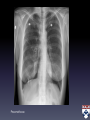
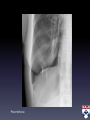
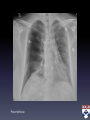
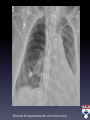
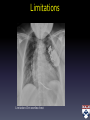
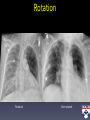
Imaging in the ICU: Stay Up-to-Date and Beware of Snares Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania Disclosures • No Financial Disclosure • Updated slide-set now available at online link Objectives • Identify the latest devices on a portable chest radiograph • Distinguish between common disease entities that mimic each other on portable chest radiograph • Discuss factors causing limitations in interpretation of portable chest radiograph Outline • Indication • Technique • Image Interpretation – Lines, Tubes, Devices, Hardware – Distinction Points for CXR findings – Limitations • Communication ACR appropriateness criteria Indication Rating Patient with clinical worsening 9 Post-insertion of tube or catheter 9 Admission or transfer to ICU 7 Post-chest tube removal 5 Stable patient. No change in clinical status 3 Rating Scale: 7,8,9 Usually appropriate 4,5,6 May be appropriate 1,2,3 Usually not appropriate Updated 2014 ACR appropriateness criteria Indication Rating Patient with clinical worsening 9 Post-insertion of tube or catheter 9 Admission or transfer to ICU 7 Post-chest tube removal 5 Stable patient. No change in clinical status 3 Rating Scale: 7,8,9 Usually appropriate 4,5,6 May be appropriate 1,2,3 Usually not appropriate Updated 2014 Technique: ACR standards for portable CXR Cooperative patients — Upright, SID 40-72 inches (as close to 72 inches as possible) Uncooperative patients — Semi-upright or supine, SID 40 inches or more kVp—70-100 without a grid or >100 with a grid Penetration / Display — Optimally retrocardiac vasculature and thoracic spine visible. Lung displayed at mid-gray level Exposure technique charts for Digital Radiography ALARA and good QC program Updated 2014 Tricks • Always look for pneumothorax – Apex if semi-upright, upright – Can be basilar if supine • Indication/History for the exam is sometimes very helpful • At end of search pattern for Lines/tubes – glance at the axillae and midline neck to catch additional lines/tubes Snares • Pneumothorax vs. skin fold • Pneumothorax on supine: deep sulcus sign • Pneumoperitoneum • Pneumomediastinum/ pneumopericardium • Mediastinal widening following LVAD placement (hematoma) Pneumomediastinum Snares • Sternal dehiscence- migratory sternotomy wire • Duplicated SVC/ Left SVC vs. arterial cannulation of a catheter • Catheter Fragments and retained electrodes from cardiac device – Can be associated with fibrin sheath Pneumoperitoneum, Ingested tooth 54 y/o M, New or Worsening Cardiopulmonary Symptoms or Signs Earlier that day Ingested tooth Snares • Unexpected objects – Tooth, Dental material – Foreign body • Satisfaction of Search Ingested Dental implant Ingested dental implant Migratory sternotomy wire Sternal fragment separation Non-vascular Tube Optimal Tip position / range Note NG/OG Gastric fundus Side-hole below GE junction Feeding tube (Dobhoff) Gastric pylorus – Duodenal/Jejunal junction Often ok with stomach ETT 3 – 6 cm above carina Assess balloon Tip moves with neck flexion/extension Tracheostomy tube Tip fixed Pay attention to balloon Endobronchial valve(s) Lodged in the small-medium sized airways Chest tube Tip in pleural space Sentinel hole in pleural space Bravo esophageal pH probe Bravo esophageal pH probe NG/OG tube looped in esophagus Feeding tube down right main bronchus into lung NG/OG tube down right main bronchus Double-lumen endotracheal tube Vascular Catheter Mid line Tip position Axilla Peripherally inserted central catheter (PICC) Low SVC – RA/SVC junction Central venous catheter (CVC) High SVC – Low SVC Dialysis catheter Low SVC- High RA Chemotherapy port (non-vesicant meds) Mid SVC – RA/SVC junction Chemotherapy port (vesicant meds) Low SVC – RA/SVC junction Pulmonary artery (PA) catheter (SwanGanz) RVOT – bilateral hila ECMO cannula (venous) IVC (just below RA/IVC junction) and/or SVC IVC filter L1 – L2 level IABP Just below superior margin of aortic knob Cardiac • Bioprosthetic valve • Mechanical valve • Annuloplasty ring • TAVR • Pacemaker • ICD • Atrial appendage clip • ASD closure device Valve Atrial Electrophysiology Ventricular • Impella • LVAD • RVAD Mechanical aortic valve Bioprosthetic aortic valve TAVR and similar valvular replacement across mitral valve Also, ASD occluder device seen Mitral clip Mitral clip Implanted loop recorder Watchman device Watchman device HeartWare LVAD Total Artificial Heart Implantation Total artificial heart implantation Total Artificial Heart Implantation Glossal stimulator Glossal stimulator Neurologic Glossal stimulator for sleep apnea Spinal stimulator Spinal infusion pump Ventricular shunts Imaging Distinction Points Pulmonary edema spectrum Pleural effusion vs. Mucus Plugging Aspiration vs. Atelectasis vs. Pneumonia Pneumothorax vs. Skin fold Pulmonary Infarct Pulmonary edema vs. ARDS vs. Multifocal pneumonia Pulmonary edema spectrum Notes Pulmonary venous congestion Interstitial edema Alveolar (Pulmonary) edema Distended veins, cephalization Blurred vessel margins Obscured vessels 19-25 >25 PCWP 13-18 mm Hg Note: Pulmonary venous congestion description is based on upright CXR Pulmonary venous congestion 12 hrs earlier Interstitial edema 12 hrs earlier Pulmonary edema Aspiration bilateral lower lobes Atelectasis, Aspiration and Pneumonia Atelectasis Aspiration Pneumonia Predominan t feature Volume loss, linear opacities, vascular crowding Patchy bibasilar and perihilar opacities Dense focal or multifocal consolidation Helpful scenarios Post-op Midline esophageal and tracheal tubes, especially when interval change Fever, Elevated WBC Post-op atelectasis, effusions RLL Infarct Pulmonary infarct Hampton’s hump ARDS with underlying pneumonia Pulmonary edema, ARDS and multifocal pneumonia Pulmonary edema ARDS Multifocal pneumonia Predominant feature Opacities are densest around hila and fade towards periphery Opacities are mediumdense and fairly uniform density from hila to periphery Dense multifocal patchy consolidations Helpful scenario Bilateral pleural effusions Intubated Febrile, elevated WBC ARDS with underlying pneumonia Skin fold Pneumothorax and Skin fold Pneumothorax Skin fold Predominant feature Helpful scenario Sharp opaque line. Not a margin Margin between gradually increasing (central to peripheral) opacity and sudden drop-off as a peripheral lucency. Not a line Multiple See vascular markings peripherally Pneumothorax Pneumothorax Pneumothorax Pneumothorax Pneumothorax Pneumothorax Left lung atelectasis due to mucus plugging Resolving Left lung atelectasis after suction of mucus plug Mucus plugging and Pleural effusion Mucus plugging Pleural effusion Predominant feature Ipsilateral mediastinal shift, volume loss, Contralateral mediastinal shift Helpful scenario Happens suddenly within hours Very dense opacification following thoracentesis, consider hemothorax Large left pleural effusion Limitations Limitation: Chin overlies chest Limitations • Positioning: affects pleural effusions – Upright – Semi-upright – Supine • Overlying structures – Chin, arms • Rotation – Causes asymmetric attenuation of L vs. R hemithorax – Can mimic pleural effusion Rotation Rotated Not rotated Communication • Succinct Impression in radiology report • Reporting most likely abnormality in each case is better than giving wide/blanket differentials • Comment on interval change of findings since prior • Communicate urgent/critical findings verbally to clinical team Take home points • Malpositioned lines/tubes and pneumothorax on every ICU CXR • Latest devices included in report • Narrow differential diagnosis for added value