Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
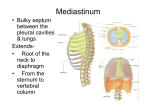
Thoracic Aortic Aneurysm This laboratory exercise is in two parts. First, you will follow a surgical procedure to repair an aneurysm of the descending thoracic aorta. Second, you complement the procedure with an anatomical dissection of the posterior and superior mediastinum. CC: End-stage ischemic cardiomyopathy Essential Question: How does embryonic folding affect the structure of the posterior and superior mediastinum? Guiding Questions: What are the contents of the posterior mediastinum? Superior mediastinum? Why does the recurrent laryngeal nerve recur about different structures on the right and left sides? Which vessels in the superior mediastinum are derived from embryonic arches four and six? Describe the arterial anastamoses within the chest wall. How is blood supplied to the vertebral column? Describe the course of parasympathetic nerves in the mediastinum. What is the major lymphatic vessel of the posterior mediastinum? Use the history and physical and laboratory data to answer the following questions: What evidence is there of cardiovascular disease? Flash movie hp_1 Where is the aneurysm located? Flash movie hp_2 Why is high blood pressure a problem for a patient with an aneurysm? Flash movie hp_3 Diagnostic Studies: Andy: do we have any plain films or CT’s of this patient’s aneurysm? I believe Ann shows an aneurysm of the arch in her workshop It is essential to preserve the blood supply to the spinal cord (arteries of Adamkiewicz). To do this, intercostal arteries were injected with contrast dye. The arteries of Adamkiewicz generally originate from intercostal arteries 9 or 10. Operative approach: In an actual case, you would use a left lateral thoracotomy in the fifth intercostal space and direct the anesthesiologist to collapse the left lung, but you have already removed the chest plate and lungs to provide you ample access to the aorta. A bypass machine would be installed in the femoral artery and vein. The blood would be cooled to 18oC and the head packed in ice. This would stop the heart and enable the brain and spinal cord to tolerate the absence of blood-flow for 45 minutes. You can take more time to do today’s procedure. 1. In preparation for suturing in a graft, detach the descending aorta from the esophagus and thoracic spine. Which veins will be placed at risk and what territories to they drain? Flash movie oa_1a Which arteries are placed at risk and what territories to they supply? Flash movie oa_1b Which lymphatic vessels are placed at risk and what territories to they drain? Flash movie oa_1c What nerves are placed at risk and what would be the consequence of injuring them? Flash movie oa_1d 2. Make an incision along the length of the descending aorta. In an actual case the length of the incision would correspond to the length of the aneurysm, but you should make your incision about 7-8 cm. What nerve is potentially placed at risk at the superior end of the incision? Locate on your donor an important branch of this nerve where it wraps around the aorta. What landmark will help you identify this branch? Flash movie oa_2 3. Make transverse incisions about half the diameter of the aorta at each end of your longitudinal incision. Open the aorta, remove any clotted blood and examine the paired branches of intercostal arteries. Generally, these are not connected to the graft, but are ligated shut. How will the intercostal spaces be perfused? Flash movie oa_3a What circumstance, discussed earlier, would lead the surgeon to connect a pair of intercostal arteries to the graft? Flash movie oa_3b Normally, the graft is laid into the open bed of the aorta, sutured to the healthy aorta at each end and the diseased wall of the aorta folded over the graft and sutured back together. However, we will continue with an anatomic exploration of the superior and posterior mediastinum. This will demonstrate the challenges for aneurysm repairs in other parts of the thoracic aorta and other surgical procedures in the region. 1. Posterior to the manubrium, you may recognize a fatty/fibrous mass that is the remnant of the thymus. What was the function of the thymus? When does it begin to atrophy? Flash movie eh_1 2. Find the two brachiocephalic veins and their junction to form the superior vena cava. Which brachiocephalic vein crosses the midline deep to the manubrium? How would this vessel appear of on a sagittal view of an MRI? Flash movie eh_2 3. Divide the left brachiocephalic vein along the midline and reflect the vein laterally to view branches of the arch of the aorta. How does the branching pattern of your donor compare to common variations? Identify these vessels on a arteriogram and trace them through the axial slices of a CT. 4. Find the ligamentum arteriosum and the recurrent laryngeal branch of the left vagus. Note that the region is rich in lymph nodes. Why? If a neoplasia or enlarged lymph node compressed the recurrent laryngeal nerve, with what symptom(s) would the patient present? Flash movie eh_4 5. Where does the right recurrent laryngeal branch from the vagus? Why is this different from the left recurrent laryngeal nerve? Flash movie eh_5 6. Trace the vagus nerves towards the esophagus and observe how they ramify to form a nerve plexus about the esophagus. Which vagus nerve do you observe ramifying on the anterior surface of the esophagus? The posterior surface? Why do the right and left vagus nerves travel on the anterior and posterior surfaces of the esophagus rather than on the right and left sides? Flash movie eh_6 7. Look for the thoracic duct. Inject it with paint and massage the paint superiorly. How far can you trace the paint? Where should it go? What does this vessel do? What would happen if it were severed during surgery? Flash movie eh_7