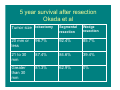
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Alternatives to Surgical Resection for Early Stage Lung Cancer Neil A. Christie MD University of Pittsburgh Medical Center Department of Thoracic Surgery Allied Health Personnel Symposium AATS 2014 Conflicts • Educational speaker for Varian Lung Cancer: Scope of the Problem • 170,000 plus cases in US each year • Leading cause of cancer death with 15% 5 year survival Limited Stage Lung Cancer • 16% of new cases stage IA or IB with tumor confined to the lung • Surgical cure rates for early stage lung cancer – 75% for pathologic stage IA – 60% for pathologic stage IB Surgery for Lung Cancer • anatomic lobectomy along with the N1 lymph nodes that are within the visceral pleural envelope • Sampling or formal lymphadenectomy of the central mediastinal N2 lymph nodes Medical Comorbidities and Early Stage Lung Cancer • Coexisting medical conditions can preclude surgery in some patients – COPD – Cardiac disease – Other medical comorbidities – Poor functional status Conventional XRT for Stage I Lung Cancer • Poor long term survival and poor local control Newer Ablative Therapies for Localized Lung Cancer • Radiofrequency Ablation (RFA) • Stereotactic Radiotherapy (SRT) • Potentially less morbid procedures which also allow preservation of lung function Talk Overview • Radiofrequency Ablation therapy results • Stereotactic Radiotherapy results • Rationale for patient selection for therapy in marginal patients with early stage lung cancer • Conclusions Radiofrequency Ablation (RFA) • Alternating current that moves from an active electrode (within a tumor) to dispersive electrodes (electrosurgical return pads) RFA System • Generator • Active electrode • Dispersive electrodes (return pads) RF generator Needle electrode Patient return pads (4 total; 2 on each thigh) Typical Thermal Lesions Produced in Liver 1.0 cm 3.5 cm Goal of RFA Therapy • Homogeneous necrosis of the entire tumor as well as a surrounding 1 cm margin of normal lung Upper limits of RF Ablation • Upper limit of homogenous tissue ablation for most RF ablation systems is between 4 or 5 cm • For ablation of tumors larger than 3 cm multiple overlapping spheres or cylinders of ablation are required with active electrode probe repositioning Published Results of RFA Therapy • 22 peer reviewed manuscripts reporting an experience in over 900 patients since 1st report in year 2000 RFA Procedure • Anesthetic – 50% done with conscious sedation – 40% done with general anesthesia – 10% done with epidural or local anesthesia only • Mean hospital stay 1.3 to 6 days with range from same day discharge to 35 days Results- Tumor Response After RFA Pre-RFA 1 month post-RFA 3 months post-RFA Tumor Ablation Rates • Tumor diameter is an important prognostic variable • Complete necrosis much more likely in tumors < 3 cm Tumor Ablation Rates • Herrera University of Pittsburgh with modified RECIST criteria – Complete or partial response • 67% of tumors < 5cm • 33% of tumors > 5 cm • Akebashi with contrast enhanced CT and PET – Complete ablation • 69% of tumors < 3 cm • 39% of tumors >3 cm Ablate and Resect Studies • Nguyen and Ambrogi –Complete necrosis in 38% and 67% respectively –Complete ablation more probable in tumors < 2 cm Survival following RFA • Ambrogi – Median survival for stage I lung cancer 18.9 months • Tumor < 3 cm median survival 30.5 mo • Tumor > 3 cm median survival 14.9 mo Survival following RFA • Simon with 75 stage I lung cancer patients median survival 29 months – 1 year 78% – 2 year 57% – 3 year 36% – 4 year 27% – 5 year 27% Complications of RFA • Mortality –One large study of 153 patients had a 2.6% mortality rate Complications of RFA • • • • • • • • • • • Pneumothorax: 0 – 54% (usually 20%) Pneumonia: 0 – 22% (1 fatal) COPD Exacerbation: 0 – 6% ARDS: 0 – 3% (3 fatal) Pulmonary abscess: 0 – 6% Hemoptysis: 0 – 12% (1 fatal) Hemothorax: 0 – 4% Pleural effusion: 0 – 4% Empyema: 1% BP fistula: 1% Pulmonary Contusion: 0 – 1% Stereotactic Radiotherapy (SRT) Conventional Radiotherapy • Standard approach 45 – 66 Gy total dose in 1.8 to 2 Gy fractions • 5 year survival rates 10 – 30% Dose Escalation • Benefit to dose escalation with dose – response relationship with local control and survival • Dose escalation limited by toxicity to lung with radiation pneumonitis 3-D Conformal RT • More sophisticated planning techniques that limit treatment volumes and radiation to normal lung tissue to allow safer dose escalation • Still have significant local failure Stereotactic Radiotherapy (SRT) • Three dimensional conformal planning techniques • Stereotactic targeting with image guidance • Systems to decrease the effect of lung motion Tumor targeting • Ablative doses to the tumor • Limit radiation to normal tissue to prevent toxicity Compensating for Respiratory Motion • Tumor tracking • Gating • Respiratory inhibition Diagnostic X-Ray Source Linear Accelerator Robotic Arm Image Detectors Treatment Couch Dosimetry • Potent dose which confidently hits the target while having a very sharp fall off dose gradient outside the region of the tumor • Multiple bream paths from multiple directions Pre Rx xxxxxxxxxxxx Radiosurgery Results • Onishi 2007 • Hypofractionated stereotactic radiotherapy for stage I lung cancer in 257 patients in a Japanese multi-institutional study • 18 – 75 Gray in 1 – 22 fractions • Median F/U 38 months • 5.4% incidence of symptomatic radiation pneumonitis Radiosurgery Results • Local recurrence in 36 patients (14%) – BED> 100 Gray 8.4% – BED< 100 Gray42.9% • 5 year survival 71% for those with BED> 100 vs 30% for BED< 100 • Nodal recurrences in 11% – 5.1% isolated to LN – 3.1% LN and local – 2.8% LN and distal Radiosurgery Results • Timmerman 2003 • Dose escalation study in 37 patients with medically inoperable stage I lung cancer • 3 fractions starting at 8 Gray and escalated to 20 Gray • No change in pulmonary function • 2 patients with grade three pneumonitis • 87% tumor response rate • 6 patients experienced relapse by 15 months Radiosurgery results • • • • • • Timmerman 2006 70 patients withT1 or T2 lung cancer 60 to 66 Gray in three fractions over 1 – 2 weeks Local control at 2 years was 95% Median overall survival 32 months Grade 3 – 5 severe toxicity or death in 14 patients • Median time to toxicity was 10.5 months Radiosurgery Results • Central tumor predictor of toxicity • Large tumor predictor of toxicity Outcomes with current Regimen • 20 Gy X 3 peripheral tumors • 12 Gy X 4 central tumors • Minimal toxicity / no change in PFTs • Local control rates 85 to 90 % Phase II Trial SBRT peripheral tumors • Timmerman et al. JAMA 2010 • Phase II North American Multicenter trial SBRT for T1T2N0 NSCLC (<5cm) peripheral medically inoperable • 18 Gy x 3, 3 year F/U • 55 patients (44T1, 11T2) Timmerman et al. • 51% complete response rate at 6.5 months post Rx • Complete or partial response in 89% patients Timmerman et al • 1/55 patients had recurrence at treated site • 3 year primary control rate 98% • 3/55 patients had recurrence within the involved lobe • 3 year primary tumor and involved lobe control rate 91% Timmerman et al. • 2/55 regional nodal failures (33 and 36 months) • 3 year local/regional control rate 87% • 11/55 metastatic disease Timmerman et al. • 26 patients died in F/U (10 of cancer) • 3 year disease free survival 48% • 3 year overall survival 56% • No treatment related deaths • 2 patients with grade III or IV adverse events SBRT vs Wedge Resection • Grills et al. Journal of Clinical Oncology, 2010. • T1-T2NO NSCLC (< 5 cm) • Wedge resection 69 patients • SBRT 58 patients (medically inoperable) – 12 Gy x 4 or 12 Gy x 5 • Staged PET/CT +/- mediastinoscopy (30% wedge patients and 20% SBRT patients) Grills et al. • Mean FEV1 1.39 both groups • SBRT patients older and higher comorbidity index • Median F/U 2.5 years Grills et al. Loc Rec Reg Rec Loc Reg Rec Dist Mets Over Surv Can Surv SBRT 4% n=55 4% 9% 19% 72% 93% Wedg 20% n=69 18% 27% 21% 87% 94% SBRT vs Surgery • Crabtree et al. JTCVS 2010 • 462 surgical patients F/U 31 months – 49 wedge, 16 seg, 375 lobe, 22 pneum • 76 SBRT patients F/U 19 months • Staged with CT and PET/CT • Surgical patients younger, lower comorbidity scores, better pulmonary function Crabtree et al. Overall Survival surgery 68% Cancer Specific Survival 82% SBRT 32% 82% 3 year follow-up Local Control 96% 89% Crabtree et al. • Propensity matching to find 2 similar groups wrt age, clinical stage and comorbidity • No difference in overall survival, cancer specific survival, or local control • In high risk group operative mortality 7% with 44% complication rate (27% pneumonia or resp failure) Conclusions • RFA results comparable to conventional XRT, inferior to surgery and SBRT • Await results of ACOSOG phase II trial with standardized technique Conclusions • SBRT has excellent local control and better than expected regional control • Long term recurrences may be underestimated due to high non-cancer deaths in patient population studied • Results of SBRT in operative candidates now showing 80% T1N0 and 70% T2N0 Selection of Therapy in Patients with Pulmonary Compromise Treatment Options for Stage I NSCLC (T1/T2 N0 M0) • Surgical Resection – Lobectomy – Sublobar Resection • Segmentectomy • Wedge Resection • Nonsurgical Therapy – Ablative techniques • Stereotactic Radiosurgery • Radiofrequency Ablation – Radiation Therapy • No Treatment Lobectomy versus Sublobar Resection / Ablation Type of Resection: Lobectomy Sublobar Resection/ Ablation Local Control + + - - + Survival Lung Function - Local Control: Lobectomy vs Sublobar Resection • Ginsberg RJ, Rubinstein LV. Randomized Trial of Lobectomy versus limited Resection for T1N0 NSCLC. Annals of Thoracic Surgery 1995. 60(3):615. • Local recurrence – 21/122 (17%) sublobar resection – 8/125 (6%) lobectomy Survival: Lobectomy vs sublobar resection • LCSG • Limited resection associated with 30% increase in overall death rate and 50% increase in death with cancer 5 year survival after resection Okada et al Tumor size lobectomy Segmental resection Wedge resection 20 mm or less 96.7% 92.4% 85.7% 21 to 30 mm 87.4% 84.6% 39.4% Greater than 30 mm 81.3% 62.9% 0% Lung Fuction: Lobectomy vs sublobar resection • LCSG • FEV1 at 6 and 12 months F/U was preserved in the sublobar resection group versus the lobectomy group Periop mortality in patients with very poor lung Function (NETT) • 140 patients FEV1 < 20% DLCO < 20% • Perioperative mortality 28.6% Comorbidity, Functional Status and Survival in Stage I NSCLC • All were independent predictors of survival for lung cancer; independent of age and treatment modality • Age was not a predictor of poor outcome • When KPS < 70 and CIRS-G4 no benefit to Surgery – Surgical survival 11% – XRT survival 6% Lung Resection in the elderly • Port et al. Surgical resection for lung cancer in the octogenarian. Chest 2004 126:733. • 61 patients mean age 82 (range 80 – 87) – – – – • • • • 4 pneumonectomies 46 lobectomies 6 segmentectomies 5 wedge resections Death 1/61 (1.6%) Major complications 13% Length of stay 7 days 82% 5 year survival for Stage IA NSCLC Minimally Invasive Lung resection (Thoracoscopic Lobectomy) • Onaitis et al. Thoracoscopic lobectomy is a safe and versatile procedure. Experience with 500 consecutive patients. Annals of Surgery 2006; 24(3):420 • 1.6% conversion rate • Periop mortality 1% • Periop morbidity – A fib 10% – Resp failure 1.2 % – MI 0.4% • Median length of hospitalization 3 days • NSCLC Stage IA 2 year survival 85% Sx vs SBRT • Surgery – Pros • Definitive pathologic diagnosis • Enables invasive nodal staging • Adjuvant therapy in node pos patients – Cons • Morbidity and mortality • Possible benign disease Sx vs SBRT • SBRT – Pros • 5 year local control rates better than 90% • Outpatient and mild toxicity • Prservation of lung function and quality of life – Cons • Treatment without pathologic verification • Post treatment fibrosis masking local disease recurrence • Clinical staging underestimates regional nodal involvement in up to 25% of cases and would not be addressed by SRT – Cure rate for stage II lung cancer with surgery alone is 40% and would expected to be 0% with SRT • Determination of residual disease by imaging is not reliable so salvage surgery could be delayed allowing progression of cancer to an advanced (incurable) stage Thank You Lung Ablation Techniques, University of Pittsburgh