Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
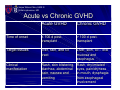
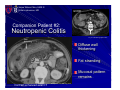
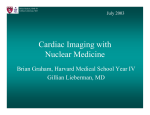
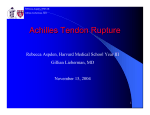
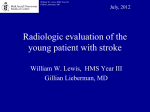
Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD November 2006 Graft-Versus-Host Disease Jaime Wilson-Chiru, HMS III Gillian Lieberman, M.D. Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD History 21-year-old male presents with 2 days of nausea, vomiting, diarrhea Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Supine Our Patient’s Abdominal Plain Films PACS, BIDMC Upright PACS, BIDMC Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Our Patient Axial CT Slice Target sign Increased mesenteric fat Featureless small bowel PACS, BIDMC Non-contrast coronal CT PACS, BIDMC Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Findings on CT Featureless small bowel Mild bowel wall thickening Increased visceral fat “Target” pattern of bowel Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD History 21-year-old male presents with 2 days of nausea, vomiting, diarrhea Day 39 s/p allogenic bone marrow transplant for non-Hodgkin lymphoma Acute graft-versus-host-disease Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD GVHD Overview Complication of allogenic bone marrow transplantation in which mature donor lymphocytes attack recipient tissues (including intestinal mucosa) T-cells present in the graft produce inflammatory cytokines, including TNF-α and IL-1 HLA antigens principal initiators GVHD Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Borrowed from Dr. Hines-Peralta Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Epidemiology Occurs in up to 50 % of patients who receive an allogenic transplant from an HLA-identical sibling Risk factors – HLA disparity – Older age – Donor and recipient gender disparity – Splenectomy Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Acute vs Chronic GVHD Acute GVHD Chronic GVHD Time of onset ≤ 100 d posttransplant > 100 d posttransplant Target tissues liver, skin, and GI tract Clinical manifestation Liver, skin, GI – oral mucosa and esophagus Rash, skin blistering, Rash, dry/irritated diarrhea, abdominal eyes, pain/dryness in mouth, dysphagia pain, nausea and from esophageal vomiting involvement Now, let’s focus on the radiological manifestations of GVHD Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Intraluminal Hemorrhage GVHD – Companion Patient #1 Contrast study of the GI tract Coy et al, Radiolographics 2003 Contrast-enhanced axial CT Featureless small bowel Courtesy of J. Kruskal Now, back to our patient… Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD GVHD – Our Patient Target sign Increased mesenteric fat Featureless small bowel PACS, BIDMC Axial CT Slice Non-contrast coronal CT PACS, BIDMC Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Radiologic Findings Diffuse featureless loops of bowel with loss of mucosal pattern Submucosal edema “Target” sign or “halo” sign http://faculty.southwest.tn.edu/jiwilliams/models_of_the_digestive_system.htm Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Differential Diagnosis of GVHD Neutropenic Colitis (Typhlitis) Pseudomembranous Colitis Infectious Colitis Inflammatory Bowel Disease Jaime Wilson-Chiru, HMS III GVHD Gillian Lieberman, MD Companion Patient #2: Neutropenic Colitis Coy et al, Radiolographics 2003 Wall thickening Diffuse wall thickening Fat stranding Fat Stranding Mucosal pattern remains Contrast-enhanced axial CT Kirkpatrick et al, Radiology 2003 Jaime Wilson-Chiru, HMS III GVHD Gillian Lieberman, MD Companion Patient #3: C. diff. Colitis Mucosal irregularity Wall thickening Coy et al, Radiolographics 2003 Diffuse wall thickening Mucosal irregularity Contrast-enhanced axial CT Coy et al, Radiolographics 2003 Shaggy wall contour Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Diagnosis of GVHD Diagnosis from clinical grounds, with radiological and histological confirmation Severity of disease is variable Grading determined by an assessment of the degree of involvement of the skin, liver, and GI tract Stage of Acute GVHD by Organ System ORGAN GRADE DESCRIPTION Skin +1 Maculopapular rash over <25 % of body area +2 Maculopapular rash over 25 to 50 % of body area +3 Generalized erythema +4 Generalized erythema with bullous formation, desquamation +1 Bilirubin 2.0 to 3.0 mg/dL; SGOT 150 to 750 +2 Bilirubin 3.1 to 6.0 mg/dL +3 Bilirubin 6.1 to 15.0 mg/dL +4 Bilirubin >15.0 mg/dL +1 Diarrhea >30 mL/kg or >500 mL/day +2 Diarrhea >60 mL/kg or >1000 mL/day +3 Diarrhea >90 mL/kg or >1500 mL/day +4 Diarrhea >90 mL/kg or abdominal pain with or without ileus >2000 mL/day Liver Gut Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Prophylaxis & Treatment Prophylactic regimen a combination of methotrexate and cyclosporine Corticosteroids first and most effective treatment option One study demonstrated a 30% cure rate of moderate to severe acute GVHD Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Conclusions Patients who undergo hematopoietic cell transplant are at risk for GVHD Radiological manifestations of GVHD can look like other inflammatory and infectious entities Prompt diagnosis is essential, since prognosis is dependent on early treatment Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD Acknowledgements Andrew Hines-Peralta, MD Gillian Lieberman, MD Pamela Lepkowski Larry Barbaras, Webmaster Jaime Wilson-Chiru, HMS III Gillian Lieberman, MD References 1. Chao, NJ. Pathogenesis of graft-versus-host-disease. UpToDate. http://www.uptodate.com. Accessed 11/08/2006. 2. Coy, DL, et al. Imaging Evaluation of Pulmonary and Abdominal Complications Following Hematopoietic Stem Cell Transplantation. Radiographics 2005; 25:305-318. 3. Gore, RM, et al. Inflammatory Conditions of the Colon. Seminars in Roentgenology 2001; 2:126-137. 4. Iwasaki, T. Recent Advances in the Treatment of Graft-Versus-Host Disease. Clinical Medicine and Research 2004; 2(4):243-252