Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
The Effects of Posture Change and
Continuous Positive Airway Pressure
Cardiac Natriuretic Peptides in
Congestive Heart Failure*
on
Michael A. Wilkins, BSc (Hons); Xiao-Ling Su, MD;
Mark D. Palayew, MD; Yoshihiro Yamashiro, MD; Peter Bolli, MD;
John K. McKenzie, MD; and Meir H. Kryger, MD, FCCP
We studied changes in the peripheral plasma levels of
atrial natriuretic peptide (ANP) and brain natriuretic
peptide (BNP) in seven patients with congestive heart
failure (CHF) during four 1-h protocols during which
patients maintained either an upright or a supine
posture with or without nasal continuous positive airway pressure therapy (N-CPAP) at a pressure of 10 cm
H20 (FIo2=0.21). The mean plasma ANP concentration
of patients increased significantly from baseline at the
end of 1 h of recumbency (65.9 + 5.8 to 82.6 ± 8.3 pg/mL
(mean ± standard error); p<0.05). This increase was
prevented by concomitant N-CPAP therapy (72.1 ± 8.0 to
61.0 ± 8.8 pg/mL; p=NS). The mean level of ANP
decreased significantly (71.9 ± 9.0 to 62.5 ± 8.0 pg/mL;
p<0.05) while patients simply maintained an upright
posture. A significant reduction was also observed when
patients remained upright with accompanying N-CPAP
(72.6 ± 10.9 to 54.6 ± 4.3 pg/mL; p<0.05). There were no
significant changes observed in the mean level of BNP
for any of the protocols undertaken. We conclude that
in patients with chronic CHF, (1) an increase in ANP
concentration occurs with recumbency, and this can be
prevented by N-CPAP therapy; (2) a decrease in ANP
occurs with maintenance of an upright posture, and that
this reduction may be augmented by N-CPAP; and (3) no
net change in BNP concentration occurs with either
posture change or N-CPAP. (Chest 1995; 107:909-15)
Cardiac atrial cells secrete atrial natriuretic peptide (ANP) primarily in response to the distention of the right atrium that occurs during central
volume expansion.1 Similarly, it has recently been
shown that brain natriuretic peptide (BNP) is released by cardiac ventricular cells under stretch.2 The
overall effects of these natriuretic hormones seem to
be the prevention of volume and pressure overload on
the central circulation. They achieve their effects by
modulating cardiovascular, renal, and endocrine
functions. Atrial natriuretic peptide acts primarily by
vasodilation of the peripheral vasculature and as a
diuretic, increasing urinary sodium excretion by increasing glomerular filtration rate, inhibiting tubular
sodium reabsorption, and reducing activity of the
renin-angiotensin-aldosterone system.1 Baseline ANP
and BNP levels have been found to be elevated in
proportion to congestive heart failure (CHF) severity, with findings of 50-fold and 500-fold increases
over normals, respectively, in the most severe cases.2'3
These elevations of ANP and BNP have also been
shown to decrease dramatically following successful
treatment of the heart failure.4'5
Our laboratory has shown previously that during
the sleep of patients with CHF, ANP levels are not
only at their highest concentration, but also fluctuate
widely.6 These findings suggest a possible worsening
of heart failure during sleep. Posture change from the
upright position of wakefulness to the recumbent
position of sleep may contribute to this cardiac
impairment. Sleep fragmentation and hypoxemia,
induced by apneic periods commonly found in
patients with CHF with Cheyne-Stokes respiration,
may also be responsible for cardiac deterioration
through a mechanism of sympathetic activation with
subsequent vasoconstriction and increased catecholamine levels.7 By studying patients who were neither
asleep nor hypoxic, we were able to isolate the effect
of posture change on ANP levels.
The increased levels of ANP that have been shown
*From the Department of Respiratory Medicine (Drs. Wilkins,
Su, Palavew, Yamashiro, andIKryger) and Nephrology (Drs.
Bolli and McKenzie), University of Manitoba, Winnipeg, Canada.
This work was supported by the Manitoba Health Research
Council, the St. Boniface Hospital Research Foundation, and the
Medical Research Council of Canada. Dr. Yamashiro is a fellow
of the Manitoba Lung Association.
Manuscript received December 2, 1993; revision accepted July
29, 1994.
Reprint requests: Dr. Kryger, SBGH Research Center, 351 Tache Avenue, Rm. 2034, Winnipeg, MB, R2H 2A6 Canada
ANOVA=analysis of variance; ANP=atrial natriuretic
peptide; BNP=brain natriuretic peptide; CHF=congestive
heart failure; LVEF=Ieft ventricular ejection fraction;
N-CPAP=nasal continuous positive airway pressure;
NYHA=New York Heart Association
Key words: congestive heart failure; continuous positive
airway pressure; natriuretic peptide
CHEST / 107/4/APRIL, 1995
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21712/ on 05/02/2017
909
Table 1-Anthropometric Data*
Patient
No./Age,
yr/Gender
1/56/F
2/62/M
3/64/F
4/66/F
5/64/M
6/66/M
7/69/M
NYHA
FVC,
%
FEV1/FVC,
Diagnosis
LVEF,
%
FEV1,
kg/M2
%
%
Dco,
%
pH
PaCO2,
mm Hg
PaO2,
mm Hg
30
29
32
22
19
24
26
DCM
IHD
IHD
IHD
IHD
IHD
IHD
16
26
38
22
32
33
33
3
2
2
3
3
2
3
66
101
83
69
79
72
67
57
118
103
54
94
65
55
87
116
124
77
121
91
81
50
72
64
45
60
87
...
7.42
7.39
7.43
7.45
7.40
7.36
7.37
36
40
32
37
34
42
39
79
77
98
78
97
73
75
BMI,
*BMI=body mass index; FVC=forced vital capacity; DCM=dilated cardiomyopathy; IHD=ischemic heart disease; Dco=diff using capacity for
carbon monoxide.
to occur with recumbency were attributed to increased cardiac filling pressures caused by the immediate redistribution of blood from the extremities
to the thorax, then secondarily by the shift of fluid
from the interstitium into the intravascular space.8
These increased filling pressures in turn stretch the
right atrium and precipitate the release of ANP. It
has been postulated that any procedure that increases
intrathoracic pressure should prevent these changes
by reducing both preload and afterload on the heart
and by reducing chamber stretch through direct
transmural pressure.9 Nasal continuous positive airway pressure (N-CPAP), the most widely used treatment for obstructive sleep apnea, is a noninvasive
therapy that causes such an increase in intrathoracic
pressure.10 The impact of N-CPAP on the ANP levels of patients with CHF has only very recently been
examined; a preliminary report suggests that N-CPAP
prevents the rise in ANP seen with recumbency."1
Furthermore, if the high levels of BNP observed in
patients with CHF are the result of a mechanism
similar to that for ANP but involving ventricular
stretch, then they too may rise with recumbency due
to an increase in afterload, and N-CPAP may prevent
their rise. N-CPAP may reset the high levels of both
natriuretic peptides when used during the sleep of
patients with CHF and may alleviate some sequelae
of impaired cardiac function. We have been unable
to find literature detailing the response of BNP levels to either posture change or N-CPAP. In this study,
changes in the levels of ANP and BNP during
postural change with and without N-CPAP were used
to assess the effects of these two interventions on heart
failure.
METHODS
Patient Selection
Subjects were chosen on the basis of a left ventricular ejection
fraction (LVEF) less than 40%, New York Heart Association
(NYHA) classification of 2 to 4, absence of severe COPD, age
younger than 70 years, and informed written consent from the
patient's family physician and cardiologist. Patients who could
not lie flat were excluded. Seven patients (four men and three
910
women; age range, 56 to 69 years; mean, 64 years) were selected
(Table 1). Left ventricular ejection fractions, as determined by
radionuclide ventriculography, ranged from 16 to 39% (mean,
29%). Six patients had a diagnosis of ischemic heart disease. The
remaining patient was in heart failure due to an idiopathic dilated
cardiomyopathy. All patients were receiving pharmacologic
treatment for these conditions and their medications were not
altered during the study. Medications included inotropes, calcium
channel inhibitors, diuretics, beta-blockers and angiotensin-converting enzyme inhibitors.
Pulmonary function tests showed that on the basis of FEV1/
FVC ratio (range, 77 to 124% predicted; mean 100%), none of the
patients had severe COPD. Complete blood cell counts and serum
chemistry studies (electrolytes, liver enzymes, albumin, glucose,
urea, and creatinine) were normal. These tests were performed so
that patients with conditions other than CHF that might impact
on the natriuretic peptides in some way could be excluded.
Patients gave informed written consent to the study, which was
approved by the Committee on the use of Human Subjects in
Research at the University of Manitoba.
Study Protocol
Subjects were brought into the laboratory on four consecutive
days, for 2 h each day. To minimize circadian factors that might
affect the natriuretic peptides, sessions on the same patient were
scheduled for the same time each day.
Throughout the first hour of every 2-h session, patients were
kept at rest in an upright position to ensure that all subjects were
at the same relative baseline in terms of cardiac work and posture.
During this period, patients had an indwelling catheter inserted
into an antecubital vein. An earclip pulse oximeter (Biox 3740,
Ohmeda, Boulder, Colo) was attached and continually measured
patients for changes in SaO2 and heart rate. Blood pressure was
measured near the end of the first hour and again at the conclusion of the second hour of each day's session.
The second hour of each session involved one of the following
four conditions: (1) the patient remained upright with no
N-CPAP; (2) the patient was placed supine with no N-CPAP; (3)
the patient remained upright with N-CPAP; or (4) the patient was
placed supine with N-CPAP. Over the 4 days of the study, each
patient completed all four of the second hour-conditions but the
order in which this was done was randomly decided for each
participant. During the N-CPAP protocols, patients were fitted
with a nasal mask and administered room air (FIo2=0.21) with
N-CPAP at 10 cm H20 pressure. One patient who was unable to
tolerate a pressure of 10 cm H20, due to discomfort, was studied
at 7 cm H20.
Measurement of the Natriuretic Peptides
Blood samples for ANP and BNP analysis were drawn four
Effects of Posture Change and CPAP on Cardiac Natriuretic Peptides in CHF (Wilkins et al)
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21712/ on 05/02/2017
Table 2-Plasma Concentrations of Atrial Natriuretic and Brain Natriuretic Peptides During Second Hours*
BNP, pg/mL
ANP, pg/mL
Time,
min
Upright
Supine
Upright+N-CPAP
Supine+N-CPAP
Upright
Supine
Upright+N-CPAP
Supine+N-CPAP
0
20
40
60
71.9+8.9
64.9 + 7.4
59.9 ± 6.5
65.9 ± 5.8
68.1+6.8
65.4 + 6.8
72.6 ± 10.9
61.3±6.5
82.6±8.3t
34.3±6.3
33.8±6.6
32.0±6.2
38,1±3.8
31.6±3.8
32.2±3.4
30.7 ±4.6
32.4±4.8
29.4±4.3
28.5 ±2.6
27.2 + 4.9
35.4+3.8
28.9±6.0
62.5±8.Ot
72.1±8.0
63.1±6.6
57.4±4.1
61.0±8.8
53.1±5.3
54.6±4.3t
33.8+5.7
29.3±6.0
36.6±6.4
*Data given as mean ± SE.
tDenotes p<0.05 (one-tailed paired t test) comparing time 0 values with time 60 values.
times for each condition. The initial 8-mL aliquot was taken at the
transition point between the first and second hours. The next two
samples were taken 20 and 40 min into the second hour, with the
final sample taken at the conclusion of the second hour. Blood was
collected into ice-cold tubes containing EDTA (3.5 mM) to which
aprotinin, a proteinase inhibitor, had been added to achieve a final concentration of 500 KIU/mL. The plasma was then immediately separated in a refrigerated centrifuge at 4°C, split into
three samples, and stored at -80°C until batch analysis of all
patient samples could be performed.
Plasma concentrations of ANP and BNP were determined by
radioimmunoassay kits (Peninsula Laboratories, Belmont, Calif).
Similar ANP kits have previously been shown by our laboratory
to have minimum sensitivities of 1 pg per tube with intra-assay
and interassay coefficients of variation of 8.7 and 11.1% (n=8),
respectively. Cumulative data from a number of earlier studies
conducted by our laboratory using the same kit indicated the
normal value of ANP to be 18.8 ±2.8 pg/mL. The BNP kit coefficients were not determined by our laboratory but were both
reported to be below 15% by the kit manufacturers. Normal BNP
values obtained from a non-age-matched (age range, 55 to 69
years; mean, 61 years) group of ten healthy volunteers were shown
to be 11.9 ±3.1 pg/mL.
I
ii
One-tailed Student t tests for paired values were
used to compare the mean plasma ANP and BNP
values at the baseline with their respective values at
the end of each of the four different protocols. This
analysis was done to determine the significance at the
95% confidence level of net peptide changes by the
end of the second hour. In addition, two-way analyses of variance (ANOVAs) (without replication) were
used to compare the baseline and 60-min values in
each protocol with their respective time points in
other protocols to detect treatment effects for both
peptides. When significant differences were detected
(p<0.05), a post hoc test (Tukey's) was applied to
identify specifically what these were. Linear regressions were also applied to see if significant correlations existed between the levels of these peptides and
anthropometric data.
-
40:
e.
Statistical Analysis
401-
ii
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Sup +ineenPA Tlime (minuts
UpieCPA Tim mnts
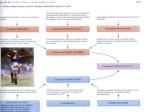
FIGURE 1. Net change in ANP during the treatment hour for the four conditions. The thin lines represent individual values; thick lines, group means. A one-tailed t test was used to compare time 0 values with time 60-min values. Note that the ANP increased only in the supine position.
&
80'
0
CHEST / 107 / 4 / APRIL, 1995
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21712/ on 05/02/2017
911
0
(a
c
U
80
60
40
20 K
r = -0.76
< 0.05
.
p
.
.
.
.
.
n
-20 10
.
1
15
2
2
20 25
LVEF (%)
40
RESULTS
Changes in ANP and BNP levels for the four different protocols are shown in Table 2. Paired t tests
reveal that the mean plasma ANP level decreased
significantly (from baseline 71.9 ± 9.0 to 62.5 ± 8.0
pg/mL; p<0.05) by the end of the second hour of the
protocol in which patients simply remained upright
(Fig 1). When patients remained upright with
N-CPAP, ANP fell further (from 72.6 ± 10.9 to
54.6±4.3 pg/mL; p<0.05; there was a decrease of
9.4±17.0 pg/mL for upright alone vs 18.0±15.2
pg/mL for upright with N-CPAP). When patients
were placed in a supine position, the mean ANP level
increased significantly (from 65.9 5.8 to 82.6 8.3
pg/mL; p<0.05), but when N-CPAP was administered with recumbency, the level of ANP did not
change significantly (from 72.1±8.0 to 61.0±8.8
pg/mL; p=NS; Table 2, Fig 1). There was no statistically significant net change in BNP by the end of the
second hour for any of the four experimental protocols.
Two-way ANOVAs (without replication) that evaluated the baseline and 60-min marks, respectively,
found that between protocols, neither the baseline
mean plasma levels of ANP nor BNP varied significantly. However, there were significant differences
(F=7.19; p=0.002) in ANP levels among the four
conditions at the 60-min mark. Using Tukey's test,
the only significantly different value was the increased mean level of ANP at the 60-min mark of the
supine without N-CPAP protocol.
The magnitudes of the increases in ANP levels seen
with recumbency were highly correlated (r= -0.76;
p<0.05) with the LVEFs of the patients (Fig 2).
Baseline ANP and BNP concentrations were not
found to be significantly correlated with patient age,
body mass index, NYHA class, or LVEF. In addition,
no significant changes were noted in patient heart
rates, blood pressures, and oxygen saturations
throughout the study.
±
912
±
FIGURE 2. Relationship between LVEF (percent)
and ANP (percent change with recumbency) showing that ANP changed the most in the supine position with lower LVEF.
DISCUSSION
rial natriuretic peptide is a peptide that is
.sed primarily from the right atrium in response
-etch from volume and pressure overload.' The
ary function of ANP is to maintain central cir-ion homeostasis through peripheral vasodilanatriuresis, and downregulation of the reninAtensin axis.2 Previously, ANP levels in patients
CHF have been shown to be chronically ele.2,3 This was confirmed in our patients, demated by a fivefold to sixfold increase in baseline
compared with normals (70.6±21.7 pg/mL
group vs 18.8 ± 2.8 pg/mL normals), with levdicating our patients to be in moderate CHF.3'4
ie reduction in ANP observed when patients reted upright for the second hour of study may be
ined by continuing blood volume redistribution
idary to gravity, away from the central circulainto the peripheral circulation. As the heart is
aded in this fashion, atrial stretch and, in turn,
>release diminish.
inversely, the increase in ANP observed when
nts were placed in a supine position for the sechour of study can be explained by blood volume
tribution into the central circulation, initially
the peripheral circulation and then later by a
shift out of the extracellular space. The resultncrease in central venous pressure and preload
es the right atrium provoking ANP release.8
ically, this central volume overload may manils orthopnea and paroxysmal nocturnal dyspnea,
cardinal symptoms of CHF.
imal and human studies have shown that conus positive pressure ventilation and N-CPAP
be beneficial to the failing heart. Continuous
ive pressure ventilation causes marked drops in
right and left end-diastolic volumes of dogs.12
an studies have demonstrated that N-CPAP
,to improvements in dyspnea, LVEF, cardiac
x, and stroke volume index in a subgroup of pa-
Effects of Posture Change and CPAP on Cardiac Natriuretic Peptides in CHF (Wilkins et al)
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21712/ on 05/02/2017
tients with poor initial baseline hemodynamics and
higher left ventricular diastolic pressures.'13"4 These
improvements were attributed primarily to a diminution of left ventricular afterload on the basis of
earlier studies'12"15'7 that showed cardiac output in
patients with CHF to be significantly afterload
dependent. Increased intrathoracic pressure will also
decrease preload, which if reduced in CHF with
volume overload will lead to decreased right atrium
stretch, decreased ANP release, and improved myocardial performance.
A more recent study using N-CPAP in patients
with severe CHF found no improvements in exercise
tolerance, dyspnea, or left ventricular function.18
Indeed, marked deterioration of two patients receiving N-CPAP led to early study termination. This
worsening was postulated to be due to a decrease in
venous return resulting in a fall in cardiac output.
The baseline hemodynamics of these patients were
not discussed. The differences between these studies
primarily relate to the volume status of the patients
studied and the separation of patients by the study
that found improvements into two groups based on
their baseline hemodynamics and left ventricular
diastolic pressures.
Our finding that N-CPAP prevents a rise in ANP
secondary to recumbency agrees with a recent preliminary report.'1 Nasal CPAP causes an increase in
intrathoracic pressure.9'19 It is possible that the addition of N-CPAP to the supine position prevents a rise
in ANP through a reduction in preload and afterload.
The net effect decreases the volume in the central
circulation14'16"19 and reduces atrial stretch. Transmural pressure may decrease preload by impinging
on vessels returning blood to the heart. By increasing
the pressure gradient between the left ventricle and
arterial circulation, N-CPAP may reduce afterload.
Left ventricular performance may also be directly
affected by an increase in transmural pressure, that
in turn reduces heart chamber size through inwardly
directed force.9 Similar mechanisms may also explain
a possible exaggeration in the reduction of ANP seen
with the addition of N-CPAP to the upright condition.
The differences in response to N-CPAP in patients
with CHF may well be due to the underlying volume
status.12'17 Patients who are volume overloaded will
benefit from N-CPAP, as this therapy will decrease
the abnormally high venous return to the heart. Patients, however, who are euvolemic or volume depleted (preload dependent) may well suffer deterioration with N-CPAP when venous return is impaired.
In addition to atrial stretch, ANP release may also
be sensitive to changes in heart rate, blood pressure,
and oxygen saturation.20-23 During this study, these
variables did not change significantly. Circadian
variations probably had little influence on our results,
because each subject was studied at the same time
each day and ANP diurnal variation has been shown
to be blunted in CHF.24 The failure of two-way
ANOVA to demonstrate significant differences between treatment baselines suggests that the pretreatment hours successfully stabilized patients.
We have also demonstrated, with linear regression,
a previously unreported relationship between the
magnitude of the change in plasma ANP concentration seen with recumbency and LVEF (r= -0.76,
p<0.05; Fig 2). The change to the supine condition
leads to redistribution of volume into the central
circulation. In patients with a decreased LVEF, this
volume load may not be dealt with appropriately,
and atrial stretch results.
To our knowledge, there have been no studies reported in the scientific literature that describe the
effects of either posture change or N-CPAP therapy
on the recently described BNP. Brain natriuretic
peptide is secreted primarily from the left ventricle
under stretch and, while present in normal individuals at 16% of the level of ANP, increases exponentially in worsening heart failure2 such that in patients
with moderate to severe CHF (NYHA class 3 and 4),
BNP levels markedly exceed ANP levels.2 We found
baseline BNP levels in our study group (mean,
31.1 ± 13.2 pg/mL) to be 44% of baseline ANP levels (mean, 70.6±21.7 pg/mL), and approximately
two to three times the value of BNP found in our
normals (mean, 11.9 ± 6.2 pg/mL).
The relatively low levels of BNP and their lack of
change with either position or N-CPAP manipulation
can be explained in a number of ways. First, the BNP
values found may reflect a positive long-term treatment effect of our patients with CHF. Second, left
ventricular dilatation occurs only in severe CHF after the adaptive mechanism of hypertrophy has
failed, and it is possible that dilatation has not
occurred in most of the patients we studied. Third,
clearance of BNP from the circulation is markedly
slower than that of ANP (fast, 1.7±0.07 min and
slow, 13.3±1.69 min ANP component half-lives vs
fast, 3.9+0.23 min and slow, 20.7±1.87 min BNP
component half-lives) as BNP only binds clearance
receptors at 7% the affinity that ANP does.2
Limitations
Given the fact that this was the first study (to our
knowledge) of the effect of posture and N-CPAP on
ANP and BNP, and because the protocol required
measurements over 4 days in outpatients, invasive
direct measurements of central venous pressure or
pulmonary capillary wedge pressure were not performed. Further studies should employ direct hemodynamic measurements to elucidate the mechanisms
CHEST / 107/4/APRIL, 1995
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21712/ on 05/02/2017
913
involved in greater detail. In this study, the mechanism responsible for the observed improvements can
be inferred only through a number of studies previously published.8-'9 We believe that the prevention of
a rise in ANP with recumbency by N-CPAP is an
important finding, despite the lack of invasive measurements that were precluded by the 4-day protocol.
Interpretation of the statistical tests applied in this
study requires the assumption of a normal distribution among the seven patients studied, and the small
sample size should also be considered in interpretation of the results.
The 1-h active study periods used in our protocol
were longer than those previously undertaken by a
similar study that looked at the effect of posture
change in normal subjects over 30 min,23 but still are
not long enough to extrapolate to an entire night.
Although a decrease in ANP concentration in the
patients with CHF we studied has been equated with
an improvement in cardiac performance, this does
not mean that simply reducing their levels is an end
unto itself. Indeed, we cannot be sure that the
changes observed were not due simply to other undefined factors that affect the release and clearance
of ANP. Atrial natriuretic peptide and BNP were
chosen because they represent a convenient way to
study the effects of posture change and the efficacy
of N-CPAP in patients with CHF.
CONCLUSIONS
We have shown that N-CPAP therapy can suppress
a statistically significant (p<0.05) rise in ANP seen
with recumbency and may prevent the worsening of
cardiac failure. The possibility exists that some
patients in heart failure could be placed on a regimen
of nocturnal N-CPAP in much the same way that
patients with obstructive sleep apnea are presently
treated.25 What has not clearly been defined, however, is in which patients N-CPAP may help and in
which the reduction of venous return may lead to
even greater cardiac impairment. This can be clarified in future studies through direct hemodynamic
measurements. We conclude that in patients with
chronic CHF (1) an increase in ANP concentration
occurs with recumbency, and this can be prevented
by N-CPAP therapy; (2) a decrease in ANP occurs
with maintenance of an upright posture, and that this
reduction may be augmented by N-CPAP; and that
(3) no net change in BNP concentration occurs with
either posture change or N-CPAP.
ACKNOWLEDGMENTS: The authors wish to thank Yvette
Perry and Irene McKenzie of the Renal Hypertension Laboratory,
Heafth Sciences Center, Winnipeg, Canada for their expert
technical assistance and conscientious sample analysis.
914
REFEREN CES
1 Needleman P. The expanding physiologic roles of atrial natriuretic factor. Nature 1986; 321:199
2 Mukoyama M, Nakao K, Hosoda K, et al. Brain natriuretic
peptide as a novel cardiac hormone in humans: evidence for an
exquisite dual natriuretic peptide system, atrial natriuretic
peptide and brain natriuretic peptide. J Clin Invest 1991;
87: 1402-12
3 Burnett J, Kao P, Hu D, et al. Atrial natriuretic peptide elevation in congestive heart failure in the human. Science 1986;
231:1145-47
4 Anderson J, Woodruff P, Bloom S. The effect of treatment of
congestive heart failure on plasma atrial natriuretic peptide
concentration: a longitudinal study. Br Heart J 1988; 59:207-11
5 Togashi K, Ando K, Hasegawa N, et al. Concentrations of brain
natriuretic peptide in treated congestive heart failure. Clin
Chem 1991; 37:765
6 Steens R, MacKenzie J, Kryger M. Atrial natriuretic peptide
levels during sleep in patients with congestive heart failure and
Cheyne-Stokes respiration. Am Rev Respir Dis 1992; 145:A445
7 Francis G, Goldsmith S, Levine T, et al. The neurohumoral axis
in congestive heart failure. Ann Intern Med 1984; 101:370-77
8 Moe G, Canepa-Anson R, Howard R, et al. Response of atrial
natriuretic factor to postural change in patients with heart
failure versus subjects with normal hemodynamics. J Am Coll
Cardiol 1990; 16:599-606
9 Buda A, Pinsky M, Ingels N, et al. Effect of intrathoracic pressure on left ventricular performance. N Engl J Med 1979;
301:453-59
10 Krieger J, Grucker D, Sforza E, et al. Effects of treatment with
nasal continuous positive airway pressure on atrial natriuretic
peptide and arginine vasopressin release during sleep in patients
with obstructive sleep apnoea. Clin Sci 1991; 80:443-49
11 Naughton M, Rahman M, Hara K, et al. Acute effect of CPAP
on hemodynamics and atrial natriuretic peptide in humans
with and without heart failure. Am Rev Respir Dis 1993;
147:A610
12 Fewell J, Abendschein D, Carlson J, et al. Continuous positivepressure ventilation decreases right and left end-diastolic volumes in the dog. Circ Res 1980; 46:125-32
13 Takasaki Y, Orr D, Popkin J, et al. Effect of nasal continuous
positive airway pressure on sleep apnea in congestive heart
failure. Am Rev Respir Dis 1989; 140:1578-84
14 Bradley D, Holloway R, McLaughlin P, et al. Cardiac output
response to continuous positive airway pressure in congestive
heart failure. Am Rev Respir Dis 1992; 143:377-82
15 Jardin F, Farcot J-C, Boisante L, et al. Influence of positive
end-expiratory pressure on left ventricular performance. N
Engl J Med 1981; 304:387-92
16 Pinsky M, Summer W, Wise R, et al. Augmentation of cardiac
function by elevation of intrathoracic pressure. J Appl Physiol
1983; 54:950-55
17 Pinsky M, Matuschak G, Klain M. Determinants of cardiac
augmentation by elevations in intrathoracic pressure. J Appl
Physiol 1985; 58:1189-98
18 Davies R, Harrington K, Ormerod 0, et al. Nasal continuous
positive airway pressure in chronic heart failure with sleepdisordered breathing. Am Rev Respir Dis 1993; 147:630-34
19 Buckle P, Millar T, Kryger M. The effect of short-term nasal
CPAP on Cheyne-Stokes respiration in congestive heart failure.
Chest 1992; 102:31-5
20 Tan S, Nolan J, Craig K, et al. Supraventricular tachycardia,
right atrial pressure, atrial natriuretic peptide and polyuria-a
necessary sequence? J Intern Med 1993; 233:415-17
21 Portaluppi F, Montanari L, Ferlini M, et al. Differences in blood
pressure regulation of congestive heart failure before and after
Effects of Posture Change and CPAP on Cardiac Natriuretic Peptides in CHF (Wilkins et a)
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21712/ on 05/02/2017
treatment, correlate with changes in the circulating pattern of
atrial natriuretic peptide. Eur Heart J 1992; 13:990-96
22 Partinen M, Telakivi T, Kaukianin A, et al. Atrial natriuretic
peptide in habitual snorers. Ann Med (Finland) 1991; 23:147-51
23 Oie B, Skadberg B, Myking 0, et al. The influence of supine
relaxation on blood pressure, heart rate and atrial natriuretic
peptide in normal subjects. Scand J Clin Lab Invest 1991;
51:329-33
24 Yoshino F, Sakuma N, Date T, et al. Diurnal change of plasma
atrial natriuretic peptide concentrations in patients with congestive heart failure. Am Heart J 1989; 117:1316-19
25 Sullivan C, Berthon-Jones M, Issa F, et al. Reversal of obstructive sleep apnea by continuous positive airway pressure applied
through the nares. Lancet 1981; 1:862-65
More Study Opportunities in Cardiovascular Disease
{1995}
October 29 - November 2, 1995 * New York, New York
CHEST 1995* offers you thought-provoking sessions on
current issues in chest medicine, presented by world-renowned
experts-the same quality science found each month in Chest.
If this article on cardiovascular disease was beneficial, you will
want to take advantage of the educational opportunities at
CHEST 1995-where cardiovascular disease will be one of four
study tracks offered. For more information, call ACCP Product
and Registration Services: 800-343-2227 or 708-489-1400.
*
formerly Annual International Scientific Assembly
CHEST /107/4 J APRIL, 1995
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21712/ on 05/02/2017
915