Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
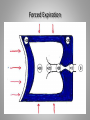
Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology • • • • The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion) Physiology • Ventilation • Perfusion • Diffusion Anatomy Inspiration/Expiration INSPIRATION Passive Expiration Forced Expiration Respiratory bronchiole Tethering Normal Conducting System Alveoli • Surface area equivalent to that of a tennis court. • Very thin. Alveolar and capillary surface Perfusion • Low pressure bed, PA pressure 30/10. • Approximately 6 billion capillaries in human lung, or about 2000 per alveolus. • Under normal (resting) conditions there is little or no flow to the apices, a waterfall effect. Ventilation/Perfusion • Under normal circumstances the V/Q (ventilation to perfusion) ratio is 1. • This is altered with decreased perfusion (PE) or decreased ventilation (obstructive lung disease or infiltrative diseases). Transportation O2 • Primarily by hemoglobulin. • Very little dissolved in plasma. Transportation of CO2 • • • • 10% dissolved in plasma. 20 % carried by Hemoglobin. 70% in form of bicarbonate. CO2 dissociation curve linear. COPD • • • • • • Chronic airflow limitation Airway inflammation Affects more than 6% of the population Third leading cause of death in US Preventable Treatable COPD • Chronic bronchitis-chronic productive cough for three months in two successive years • Emphysema-permanent enlargement of airspaces distal to the terminal bronchioles, loss of alveolar walls • “Asthma”-Reversible airflow limitation Emphysema Causes • • • • • Smoking-Duration and Amount. PACK YEARS Threshold? About 25 pack years Smoking Smoking Biomass fuel in developing countries Incidence • Overall 6.3% USA • Higher in men, lower education level and socioeconomic groups • Incidence increases with increasing age • 3rd to 6th leading cause of death RISK BY AGE Pathology • • • • • • Airway limitation-inflammation Goblet cell hyperplasia Mucus plugging Loss of airway tethering Loss of airway rigidity Bronchospasm Normal Airway Airway narrowing Symptoms • • • • Shortness of breath Cough, with or without sputum Wheezing Chest tightness Dyspnea • • • • • Lung disease Heart disease Circulatory problems Neuromuscular diseases Therefore not all dyspnea is due to lung diseases Wild Cards • ACID REFLUX • 25% of patients with significant reflux have no reflux symptoms • Another 25% underestimate the degree of reflux • Patients with symptoms have 2x rate of exacerbations • Deconditioning Physical Findings • • • • • • • Wheezing Decreased breath sounds Crackles in bases Diminished heart sounds Barrel-shaped chest Tobacco stained finger tips Clubbing is rare Chest X-ray • • • • • • Normal Hyperinflation Bullae Flattened hemi-diaphragms Basilar scarring Unexpected disease-pneumothorax, lung cancer Hyperinflation Pneumothorax Spirometry • FEV1-effort dependent • FVC-effort and time dependent, more than 6 seconds • FEV1/FVC ratio-less than 70% • Peak flow-useful for trends, very effort dependent Global initiative on chronic Obstructive Lung Disease • • • • GOLD 1: Mild (FEV1 >80% Pred.) GOLD 2: Moderate (FEV1 50-80% Pred.) GOLD 3: Severe (FEV1 30-50% Pred.) GOLD 4: Very severe (FEV1 < 30% Pred.) COPD Assessment Test OK < 10 Modified Medical Research Council Guide • Please Check Line That Applies to You • • • • • • • • Grade 0: I only get short of breath with strenuous exercise. Grade 1: Short of breath hurrying or up slight incline. Grade 2: I walk slower on level ground as similar aged individuals or I stop to rest when walking on my own. Grade 3: I stop for breath when walking 100 meters or after a few minutes. Grade 4: I am too breathless to leave the house or I am breathless dressing or undressing. ___ ___ ___ ___ ___ RISK • Related to history of exacerbations • Group A: Low risk, less symptoms - GOLD 1-2 and 0-1 exacerbations • Group B: Low risk, More symptoms – GOLD 12 and 0-1 exacerbations • Group C: High risk, Less symptoms – GOLD 34 and > 2 exacerbations • Group D: High risk, More symptoms - GOLD 34 and > 2 exacerbations Exacerbations • • • • • • Increased dyspnea Increased cough Sputum production +/- fever +/- chest pain – chest tightness Median time between onset of symptoms and onset of treatment 3.69 days Exacerbation Treatment • • • • • • • Steroids, oral or IV Antibiotics, oral or IV Additional bronchodialators Hospitalization Non-invasive ventilation Ventilation Over 7% do not return to baseline Hospitalization • Mortality > 10% • Only 75% recover to recent baseline at 5 weeks • 7% have not recovered baseline at 3 months • 63% readmitted during following year • Represents 40-60% of overall cost of care Hospitalization • Immobilization • Sedation • Hospital acquired conditions • Fragmentation of care – Medication reconciliation – cost of medications – followup • Depression - anxiety Hospital at Home • • • • • Population health strategy Competent caregiver available In a contained geographic area Dedicated team of doctor(s), nurses, etc. Daily visits, possibly including phone or telemedicine visits • Limited care time frame < 15 days Smoking Cessation • • • • • • Without help/nicotine replacement-10% With help/nicotine replacement-50-60% ASK – ADVISE – ASSESS – ASSIST- ARRANGE Chantix Nicotine, Give enough Too much nicotine causes nausea Decreased airflow + smoking • Progressive lung disease • 25 times normal risk for heart attack or stroke • 8 times risk for lung, laryngeal, esophageal, stomach, kidney, bladder, oral and pancreatic cancer • Cessation rapidly reduces the risk of cardiovascular complications Medications: Short acting Rescue • • • • • • Beta agonists, MDI or nebulizer (albuterol) Techniques Spacers Cost Intended for rescue Primary side effects cardiac arrhythmia (tachycardia) and tremor Medications: Short acting Rescue • • • • • Anticholinergics, MDI or nebulizer (Atrovent) Short acting Rescue Costs Adverse effects rare, dryness Medications: Long acting • Beta agonists, MDI and nebulizer • Foradil and Serevent are the primary single agents with MDI • Perforomist and Brovana are the nebulized forms • Almost never used alone • Increased risk of death in asthma patients when use alone (Black Box Warning) Medications: Long acting • Anticholinergics, MDI • Spiriva and Tudorza • Cost Medications: Inhaled Steroids • MDI and nebulizer • Controversy • Single agents, Flovent, Asmanex, Qvar, Pulmicort • Anti-inflammatory • Adverse effects-oral thrush, hoarseness, possible osteoporosis, increased risk of pneumonia Medications: Steroids/Beta agonists • • • • • MDIs Advair Discus and MDI Symbicort Dulera Breo, new, fluticasone and vilanterol Medication: LABA + LA Anticholinergic • Anoro, new Medications: Steroids • • • • Anti-inflammatory Oral prednisone or Medrol Dose and length of treatment controversial IV for hospitalized patients, dose and length of treatment controversial • Adverse effects – Hyperglycemia, thrush, increased risk of infection, osteoporosis, weight gain, myopathy Medications: Phosphodiesterase-4 Inhibitors • Daliresp – anti-inflammatory • Frequent side effects with nausea, vomiting, diarrhea, generalized aches, loss of appetite Medication: Theophyllins • Moderate bronchodialator • Toxicity is dose related • Adverse effects – nausea, vomiting, headaches, seizures • Blood levels altered by other medications, both up and down Special Consideration • Alpha-1 Antrypsin Deficiency • Earlier emphysema with a basilar predominance • Replacement available • Testing is free Vaccinations • Yearly flu immunization • Pneumococcal vaccine for patients 65 years and older Oxygen • • • • • Improve mortality Improve dyspnea Improve quality of life Improve cognition Cost – over $500/mo., 1 million patients in USA at a cost of over 2 billion dollars Oxygen • PaO2 , 55 mmHg or saturation, 89% at rest • PaO2 , 60 with cor pulmonale, right heart failure or HCT > 55 • O2 saturation less than 89 % for more than 5 minutes with sleep (Look for OSA) • Pao2 < 55 or saturation <88 with exercise • In COPD patients check ABGs on O2 to check PaCO2 ANN Internal Med 1980; 93:391 Lancett 11981; 1:681 Oxygen • • • • No benefit for saturations > 92% Increase in PaCO2 (Hypoventilation) Absorptive atelectasis Hyper-oxemia can result in decreased free water clearance • Facial burns especially in patients with facial hair • Fall risk with the tubing • NO SMOKING RISK • Related to history of exacerbations • Group A: Low risk, less symptoms - GOLD 1-2 and 0-1 exacerbations • Group B: Low risk, More symptoms – GOLD 12 and 0-1 exacerbations • Group C: High risk, Less symptoms – GOLD 34 and > 2 exacerbations • Group D: High risk, More symptoms - GOLD 34 and > 2 exacerbations Treatment Recommendations GOLD • • • • Group A Group B Group C Group D • Group A • Group B • Group C • Group D • • • • • • S-A Beta agonist or anticholinergic L-A Beta agonist or anticholinergic ICS + LA Beta or LA anticholinergic ICS + LA Beta +/or LA anticholinergic ALTRERNATIVE LA Beta or LA anticholinergic or SA Beta with SA anticholinergic • LA Beta with LA anticholinergic • LA Beta + LA anticholinergic or LA Beta + PD4 Inh or LA anticholinergic + PD4 Inh • ICS + LA Beta + LA Antichol. Or ICS + LA Beta + PD4 Inh, or LA Beta + LA antichol, LA antichol + PD4 inh Other Considerations • Exercise • Mucolytics • Antidepressants Comorbidities • • • • • • • Coronary artery disease Osteoporosis Peripheral vascular disease Cancer Heart failure Atrial fibrilation Interstitial lung diseases Chronic Care Management • • • • • Self Management Strategies Clinical Information Systems Delivery System Design Decision Support Community Resources Self Management Strategies • Education-Behavioral support-Motivational support – to promote behavioral changes: • 1. Improved medication adherence. • 2. Smoking cessation. • 3. Vaccinations. • 4. Regular bronchodialator use. • 5. Proper inhaler technique. • 6.Regular exercise. • 7.Supplemental Oxygen use. • 8. Increased physical activity in the home. • 9. Early reporting of exacerbations. Referrences • • • • • • • • • • • • • • Global Initiative for Chronic Obstructive lung Disease Lancet 370; 2007, p741, “International variation…” Lancet 378; 2011, p991, “Lifetime risk…” MMWR 61, 2012, p938, “COPD among adults” UpToDate Chest 130; 2006, p1096, “Role of gastroesophageal…” Am J Crit Care Med 180; 2009, p3, “The Natural History…” NEJM 365: 2011, p1184, “Changes in Forced…” Pulmonary Physiology in Clinical Medicine, Tisi Am J Respir Crit Care Med 161; 2000, p 1608, “Time course and recovery…” BMJ 1; 1977, p1645, “The natural history…” Am J Respir Crit Care Med178; 2008, p332, “Effect of pharmacotherapy…” JAMA 309;2013, p2223, “Short-term vs conventional…” Eur Respir J; 2009: 507-512. “ Discharge Planning and home care…” References, cont. • Proc Am Thor Soc; 9 (1):9-18. “Integrated care of the COPD patient” • International J of COPD 2011; 6: 605-614. “Implementing chronic care for COPD…” • Arch Int Med 2007; 167: 551-561. “Systematic Review of the Chronic Care Model in COPD…” • Health Affairs 2001; 20 (6):64-78. “Improving Chronic illness care…” • Am J Crit Care Med 2004; 169: 1298-1303. “Early Thearpy improves outcomes…”