Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
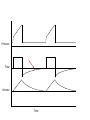
MANAGEMENT OF SEVERE OBSTRUCTIVE LUNG DISEASE Craig Rackley, MD Assistant Professor of Medicine Duke University Medical Center Faculty Disclosures •None Objectives • Understand the anatomy of COPD • Understand GOLD classification of COPD • Understand basic pharmacologic treatment targets and goals • Understand when to use non-invasive ventilation for acute exacerbations of COPD/Asthma • Understand how to manage a patient with COPD or asthma requiring invasive ventilation Clinical case 69 yo man with a 90 pk-yr smoking history, FEV1/FVC ratio of .48 and an FEV1 of 26% predicted comes in for an initial evaluation in pulmonary clinic. Anatomy of obstructive lung disease www.nhlbi.nih.gov Causes of Airflow Obstruction • Increased resistance and narrowing of airways due to • Airway smooth muscle hypertrophy and contraction • Mucous cell hypertrophy, increased mucous production and impaction • Airway inflammation • Airway fibrosis • External compression from hyper-inflated alveoli Hyperinflation and Air Trapping Treatment goals • Decrease resistance and narrowing of airways by reversing • Airway smooth muscle hypertrophy and contraction • Inhaled beta agonists, anticholinergics, Magnesium, theophylline • Mucous cell hypertrophy, mucous production and impaction • Inhaled anticholinergics, corticosteroids • Airway inflammation • Corticosteroids, antibiotics if indicated • Airway fibrosis • Irreversible • External compression from hyper-inflated alveoli • Allow for effective exhalation Airway response to therapy What do we use to guide therapy? GOLD classification of severity of airflow limitation in COPD Global Initiative for Chronic Obstructive Lung Disease FEV1≥50% FEV1<50% Combined Assessment of COPD Global Initiative for Chronic Obstructive Lung Disease Clinical case cont. He had an FEV1/FVC ratio of .48 and an FEV1 of 26% predicted. He had 2 exacerbations last year, one required hospitalization, and he is short of breath with minimal activity. He is on no medications other than prn albuterol, which he uses 5+ times/day.. GOLD recommended first choice therapy Global Initiative for Chronic Obstructive Lung Disease Clinical case cont. Patient is started on an ICS + LABA and a LAMA with recommendation to use albuterol as needed. He has a walk in clinic that demonstrates he needs 2 LPM oxygen via nasal cannula with exertion, he is given appropriate immunizations, and he is referred to pulmonary rehab. Clinic template Chronic Obstructive Pulmonary Disease: • Based on the Global Initiative for Chronic Obstructive Lung Disease Combined Assessment of COPD, the patient is in risk category: – – – – • A: FEV1 >/= 50% and </=1 exacerbation/yr and minimal/no symptoms or dyspnea B: FEV1 >/= 50% and </=1 exacerbation/yr and moderate/severe symptoms or dyspnea C: FEV1 <50% or >1 exacerbation/yr and minimal/no symptoms or dyspnea D: FEV1 <50% or >1 exacerbation/yr and moderate/severe symptoms or dyspnea Recommendation: -Tobacco dependence: -No longer smoking. Encouraged continued abstinence. -Currently smoking. Extensively discussed need for smoking cessation. Provided information on 1-800Quit Now. Offered nicotine replacement and pharmacotherapy. We will *** -Pulmonary rehab/exercise: -Patient currently in rehab or exercising regularly. Encouraged continued lifelong exercise. -Patient currently not exercising adequately. We discussed options for exercise and pulmonary rehab. We will *** -Oxygen: -Patient has an oxygen sat >/=88% on RA at rest and with walking. Therefore, supplemental oxygen is not indicated. -Patient has an oxygen sat <88% on RA at rest and/or with walking. Therefore, supplemental oxygen is required at *** LPM at rest, *** LPM with sleep, and *** LPM with exertion. -Pharmacotherapy: -GOLD A: Short acting bronchodilator as needed -GOLD B: Long acting bronchodilator -GOLD C: ICS + long acting bronchodilator -GOLD D: ICS + long acting beta agonist and/or long acting anticholinergic Clinical case cont. He does well over the next 6 months until he gets an upper respiratory infection. This leads to significant increase in his shortness of breath and cough. His symptoms progress to where he is so short of breath he calls EMS and is taken to the ED. Clinical case cont. On initial evaluation he has a temp of 38.2 C, HR of 108, BP of 95/60, RR of 26, and O2 sat on RA of 87%. He is alert and oriented, but speaking in 2-3 word sentences. He is using accessory muscles to breath and has very poor air movement. ABG on RA: pH: 7.30 pCO2: 64 pO2: 53 When to consider ventilatory support • Evidence of respiratory muscle fatigue (clinical work of breathing, serum lactate) • Hypercarbia • Respiratory acidosis What is the “best” way to provide ventilatory support? or NIV reduces need for intubation in COPD exacerbations Cochrane Database Syst Rev. 2004;(3):CD004104. NIV reduces mortality in COPD exacerbations Cochrane Database Syst Rev. 2004;(3):CD004104. NIV for life‐threatening asthma attacks 18% Respirology. 2010 May;15(4):714-20. 4% NIV for life‐threatening asthma attacks Respirology. 2010 May;15(4):714-20. How to initiate NPPV • Initiate with oronasal facemask. If patients cannot tolerate then consider full face mask. • Settings are adjusted to • • • • Achieve adequate oxygenation Reduce work of breathing Maintain “adequate” pH Provide tolerable pressure that does not lead to worsened hyperinflation • Maximize patient-ventilator synchrony Clinical case cont. The patient is placed on bipap 12/5 and 40% FiO2. His RR decreased to 20 and his work of breathing improved. However, over the next several hours his work of breathing increased, and he became less alert despite adjustments to his bipap settings. A repeat ABG was sent. ABG on RA: pH: 7.22 pCO2: 74 pO2: 65 Indications for intubation • • • • Respiratory arrest Altered level of consciousness Extreme exhaustion Inability to adequately ventilate with NPPV After the tube goes in… Success vs failure Remember the problems Remember the problems Normal COPD How to initiate mechanical ventilation • Respiratory rate: adjusted to a rate that allows expiratory flow to reach zero prior to next breath • Tidal Volume: approximately 6-8 cc/Kg ideal body weight • Inspiratory time(PAC): adjusted to allow for adequate volume and to continue delivering breath with patient effort (i.e. inspiratory flow does not stop while patient is still wanting more air.) • Inspiratory flow rate(VAC): adjusted to give adequate flow and allow for adequate exhalation (I:E ratio) • PEEP: adjusted to the lowest level needed to ensure patient is able to trigger all breaths • Plateau pressure: <30 cm H2O • Appropriate level of sedation is key to ensure adequate patient-ventilator synchrony Clinical case cont. He is sedated, paralyzed, and placed on mechanical ventilation: VAC with a Vt of 6 cc/kg, RR of 24, PEEP of 5, and an FiO2 of 40 %. After 20 min his HR is 120, BP is 80/45, and his sat is 90%. You send a stat ABG. ABG: pH: 7.18 pCO2: 82 pO2: 58 Our Patient’s Waveforms Pressure Flow Volume Time Dynamic Hyperinflation Chest. 2015;147(6):1671-1680. Air Trapping Consequences of hyperinflation or air trapping • Barotrauma/volutrauma • Decreased venous return, preload, and cardiac output How to reduce hyperinflation or air trapping • Reduce respiratory rate • Reduce tidal volume • Increase expiratory time • Increase inspiratory flow rate (VAC) • Decrease inspiratory time (PAC) • Tolerate increased PCO2 Clinical case cont. The patient’s RR is decreased to 16. His new settings are VAC with a Vt of 6 cc/kg, RR of 16, PEEP of 5, and an FiO2 of 40 %. After 30 min his HR is 80, BP is 110/65, and his sat is 98%. You send a repeat ABG. ABG: pH: 7.32 pCO2: 56 pO2: 84 Our patient after the vent changes Pressure Flow Volume Time Clinical case cont. He remains stable overnight, so the paralytics are discontinued and his sedation is lightened. When you come back the next morning he is awake, alert, and following commands, but just doesn’t quite look comfortable. Pressure Flow Volume Time Information from an end expiratory pause Flow (L/s) Volume (L) Airway pressure (cm H2O) PEEPi = 10 “Clamp” circuit Intrinsic PEEP is end expiratory alveolar pressure PEEP can be increased until all patient efforts trigger the ventilator in assisted modes Hyperinflation will lead to increased Pplat in VAC or reduced tidal volumes with PAC Why not increase extrinsic PEEP to match intrinsic PEEP? Regional effects of positive pressure ventilation in obstructive lung disease Regional over-distention can lead to worsened V/Q matching, increased dead space ventilation, and increased lung injury. Clinical case cont. His PEEP is increased to 8 cm H2O, and he is successfully triggering all breaths. Over the next 24 hours his sedation is further reduced, and the next morning he passes an SBT, but at the end of 30 min he appears to have a slight increase in his work of breathing. He is alert, cooperative and following all commands. What do you do?? NIV decreases extubation failure in COPD Patients RR for extubation failure 95% CI COPD 0.33 0.16-0.69 Mixed MICU population 0.66 0.25-1.73 Heart Lung. 2015 Mar-Apr;44(2):150-7. Clinical case cont. He is extubated directly to bipap, does well for 6 hours, and is successfully weaned from bipap with improved work of breathing. He transfers out of the ICU the next morning. Summary • Airflow obstruction has multiple components that should be adequately treated pharmacologically • NPPV reduced mortality and reduces need for intubation in patients with COPD exacerbations • Understanding intrinsic PEEP and allowing for adequate exhalation are key to mechanical ventilation in obstructive lung disease • Extubation to NIV may reduce risk of reintubation Questions? Information from an end inspiratory pause Peak and Plateau similar No obstruction Large difference between Peak and Plateau Flow stops prior to next breath Flow does not reach zero prior to next breath Inhaled volume = exhaled volume Inhaled volume > exhaled volume Obstruction