Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
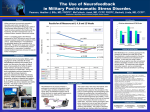
Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 1 of 10 Software and Accessories for Biofeedback and Neurofeedback Professionals from "A Matter of Mind" www.growing.com/mind, (408) 984-3333 / [email protected] Neurofeedback Low Frequency Protocol / Infra-Slow Frequency Protocol Frequently Asked Questions Please submit questions and comments to [email protected] Most recently added Q&As: Are you teaching the Othmer Protocol? Can I do the Othmer Protocol with these screens? How then does your protocol differ from the Othmers'? What is the "red thread" that you discuss? Archives: What is low frequency neurofeedback and how does it differ from other types of neurofeedback? Why would anyone want to train the cortex at infra-slow frequencies? Is there a theoretical rationale for this type of training? Are some people harmed by low frequency neurofeedback training? Is this a "one size fits all" approach? Is there a single low frequency protocol or many? How can I learn more, or get training? What type of equipment and software is required for low frequency neurofeedback? Why are multiple inhibits used? Is the Nexus (with Biotrace) a good system for low-frequency neurofeedback? How do I install the Nexus Low Frequency neurofeedback module on my computer? Why are there 7 different screens in the Nexus low frequency neurofeedback module? During a neurofeedback session can I alternate other screens with the low frequency screens? How do I fine tune my low frequency screens during a session? How do I know what training frequency to select? How do I know when to change it? Does the Nexus Low Frequency module work with the Audio-Visual Library for Biofeedback? How do I select video and audio files to use for feedback? Why do you discuss a connection between low frequency neurofeedback and mindfulness meditation? Is their a connection between low frequency neurofeedback, slow cortical potential training, and transcranial direct current stimulation (tDCS)? Where can I find a bibliography about low-frequency neurophysiology so I can read and make up my own mind? Is there a role for low frequency neurofeedback in the treatment of post-traumatic stress disorder (PTSD)? Are you teaching the Othmer Protocol? Can I do the Othmer Protocol with these screens? How then does your protocol differ from the Othmers'? What is the "red thread" that you discuss? Note: These answers occasionally refer to the color markings on Nexus electrodes and may not be applicable to other systems. Q: What is low frequency neurofeedback and how does it differ from other types of neurofeedback? [ Top ] A: Neurofeedback is a form of biofeedback. Information about the electrical activity of the brain, measured at the scalp, is fed-back to the client in a meaningful way so that the client can observe and learn to control his or her own brain activity. Since the 1970s much of neurofeedback has been done using a ground electrode (white) on a spot such as the right ear, a reference electrode (black) on a cortically quiet location such as the left ear, and an exploratory electrode (red) on the scalp over the region of interest. This is called a single channel referential montage. Usually the trainer has a range of frequencies whose amplitudes are to be increased, and one or two other ranges of frequencies whose amplitudes are to be decreased at a particular location. http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 2 of 10 Since the advent of affordable quantitative electroencephalography, practitioners of neurofeedback have been able to observe anomalous relationships of amplitude, coherence and other measures and then train the brain accordingly using one or several channels. QEEG interpretation is a specialty taking many years of study and practice. Obtaining a QEEG is especially important when there has been head trauma, stroke, epilepsy, anomalous development, or failure to respond to a therapeutic trial of neurofeedback. Despite the availability of QEEG, many neurofeedback practitioners still practice with general gentle training designed to encourage self-regulation, self-awareness, and relaxation, or they choose their sites and frequencies based on an understanding of the correlations between neurophysiology and behavior. Among an early group of pioneers were Siegfried and Sue Othmer and their many students, such as John Anderson. Twenty years ago it was observed that the exploratory electrode (red) could be placed over an area of migraine pain and often the pain would dissolve. Sometimes the reward frequency had to be shifted up or down, otherwise the client would become groggy, agitated, or uncomfortable. Sometimes the pain would move to the other side; the trainer would follow the pain with the red exploratory electrode, train at the new location and extinguish the pain. Eventually, rather than chase the pain from side to side, the black reference electrode was taken off the ear and placed on one side and the red exploratory electrode was placed on the homologous site on the opposite hemisphere. This resulted in more effective migraine management but resulted in an unexpected discovery - clients became more sensitive to reward frequency and often had interesting and important responses to experimental alterations in reward frequency over a wide range including low frequency (0.01 - 0.10 Hz). This electrode setup (ground on one ear, and red and black electrodes both on the scalp) is called a "single channel bipolar montage." This differs dramatically from the "single channel referential montage" described above. In the "referential" montage all electrodes are cortically quiet except the exploratory (red) electrode. You can be certain during training that you are primarily measuring and rewarding an actual increase in the chosen frequency band at the chosen site. In a "bipolar" montage you can not be certain if the cortical activity is increasing under one site or the other, or if the two sites are just becoming more different. This is because of the way EEG amplifiers work. When there are two scalp electrodes (red and black) and a ground (white), the amplifier circuitry always subtracts the activity of the black electrode from the red electrode. This is by design. In a referential montage the black electrode is cortically quiet, so there is nothing to subtract - the red electrode is measuring the amplitude of activity at that site. But in a bipolar montage, both the red and the black electrodes are measuring brain activity. If the cortex under both electrodes is behaving similarly (e.g., if there is hypercoherence), the "difference" (red minus black) will cancel out and be small. If both sites start behaving differently then they will not cancel out as much and your reward instrument will measure an increase. In bipolar neurofeedback you can reduce hypercoherence between two sites. This is usually a good thing. Hypercoherence is more common than hypocoherence. Creating an enduring asymmetry in amplitude between two sites with bipolar training is not likely, but it is theoretically possible. That is why this software has an "asymmetry instrument". Over the last decade practitioners using bipolar montage (Othmers, Anderson, et al) have found interesting and often very clinically useful results as they included progressively lower frequencies for training. Currently frequencies as low as 0.01-0.10 Hz are being rewarded. A characteristic of low frequency bipolar protocol is that the trainer tunes the reward frequency band based on moment to moment responses by the client. Q: Why would anyone want to train the cortex at infra-slow frequencies? [ Top ] A: Generally, if one were using a single channel referential montage it is unlikely that anyone would train at delta or lower frequencies. Delta waves are associated with sleep, coma, brain injury, developmental insult, etc. However, in bipolar training the operator is, in general, training the brain to be more different between two sites at a particular frequency, regardless of frequency. Siegfried Othmer has provided a statistical analysis [ 1 ] that shows that rewarding a bipolar low frequency "difference" amplitude, it is more likely that the brain has created the increased reward amplitude by shifting phases between sites rather than by increasing the amplitude at one of the sites. As will be described below, the ability to phase shift at infra-slow frequencies is an important component of cognitive flexibility and sensory discrimination. When doing bipolar training at low frequencies it is often observed that, as the trainer raises and lowers the reward frequency, the client experiences an alternation between arousal and relaxation. The client then seems to learn improved control of state. It is also common that shortly after a shift of reward frequency, the client will re-experience a state associated with a previous injury or issue, or may reexperience a previously forgotten perceptual skill. Such situations provide an opportunity for clients to re-acquaint themselves with states of mind that contain useful information and resources. [ See the discussion about mindfulness training and neurofeedback. ] Q: Is there a theoretical rationale for this type of training? [ Top ] A: The best rationale would be that the data shows it works. The next best thing is for you to prove it to yourself. Neurofeedback needs much more research, not just to prove that it is a powerful tool for well-being, but to help elucidate its mechanisms. There is an abundant literature emerging about the importance of robust infra-slow cortical activity. Here is a particularly interesting quote from Monto, et al, in Finland [ 2 ], printed in The Journal of Neuroscience, August 2008. “We examined the dynamics of human behavioral performance and its correlation with infraslow (0.01–0.1 Hz) fluctuations in ongoing brain activity. …The subjects' ability to detect the sensory stimuli was strongly correlated with the http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 3 of 10 phase, but not with the amplitude of the infraslow EEG fluctuations. These data thus reveal a direct electrophysiological correlate for the slow fluctuations in human psychophysical performance. We then examined the correlation between the phase of infraslow EEG fluctuations and the amplitude of 1–40 Hz neuronal oscillations in six frequency bands. Like the behavioral performance, the amplitudes in these frequency bands were robustly correlated with the phase of the infraslow fluctuations. These data hence suggest that the infraslow fluctuations reflect the excitability dynamics of cortical networks. We conclude that ongoing 0.01–0.1 Hz EEG fluctuations are prominent and functionally significant during execution of cognitive tasks.” Or consider this statement in early 2009 by Broyd SJ, et,[ 3 ] in Neuroscience and Biobehavioral reviews 33 (2009) 279-296 “Recent research has reported reduced power in low frequency resting state networks (0.06–0.2 Hz) as measured by DC EEG in a non-clinical sample of hyperactive participants who rated themselves as inattentive." There are other fMRI studies we will be reporting on this website that suggest that low frequency training can 1) improve allocation of cortical resources and 2) improve functioning of default mode networks. One of the interesting aspects of these infra-slow and fMRI studies at this time is that they are, in general, not reproducible by the average clinician in order to assist in client evaluation. That fact, and the experimental nature of neurofeedback in general, means that careful careful client selection and informed consent are crucial. Q: Are some people harmed by low frequency neurofeedback training? [ Top ] A: Practitioners who use low frequency bipolar protocol expect to get a response, usually favorable, during the first 1 or 2 sessions. Any technology capable of such rapid change is capable of disturbing a client. According to Monto, et al, above, infra-slow phase is related to the "subject's ability to detect the sensory stimuli". In low-frequency work we often find that clients reconnect with old issues and injuries, sometimes in a visceral fashion. It the practitioner lacks skill and confidence, the client can become disturbed, frightened, even angry. Many, but not all, incidences where individuals claim to have been disturbed by low-frequency training are those who have been trained by someone with relatively little experience. If the client does experience physical, emotional, or mental distress during or after the training, our protocol guide suggests alternate placements, e.g., Fp2-T4 for emotional distress, T4-P4 for physical distress, Fp1-T3 for cognitive distress; There are also methods to help the client self-regulate more effectively during an uncomfortable reaction; This underscores the point that while learning this technique the practitioner should have access to a mentor and a good protocol guide. Always make certain you work within the limits of your professional license. Hammond and Kirk (2008) [ 4 ] present a review of adverse reactions and side effects in neurofeedback. They include, but are not limited to, anxiety, agitation, panic attacks, manic-like behavior, headaches, nausea, fatigue, sleep disturbance, anger and irritability, crying and emotional lability, incontinence, enuresis, increase in depression, decline in cognitive functioning, increase in OCD symptoms, increase in somatic symptoms, tics, twitches, seizures, slurred speech, loss of previous symptomatic improvements, and temporary disorientation or dissociation. In fact, many of the most successful neurofeedback cases have had one or more temporary mal-adaptive reactions appear. The astute clinician manages these occurrences in such a fashion as to minimize the disturbance to the client and continue progress and consults with other professionals when necessary. The article by Hammond and Kirk's describes perhaps 50 cases and several studies indicating the ability of neurofeedback to cause client discomfort. This is a very small percentage of perhaps several hundred thousand neurofeedback sessions or more logged in clinicians' records. The list of suspected mal-adaptive reactions reminds us of a very important principle here: If you are not licensed and comfortable treating these conditions without neurofeedback, then neither will you be when using neurofeedback. If your client has not been notified of these possible side effects, then you are in violation of ethics guidelines. Q: Is this a "one size fits all" approach? [ Top ] A: Using bipolar variable frequency neurofeedback on most your neurofeedback clients is no more a "one size fits all" approach than is using single channel referential amplitude training on most your neurofeedback clients. A careful reading of your low-frequency bipolar protocol guide, or spending time at a training seminar, or speaking with an experienced user, will show that you must always be ready to treat what you find, not what you are looking for. Rigid protocols are often the reason clients don't progress. From the moment of your first interaction with a client, the client changes. This flexibility in the client must be met with flexibility in your approach. Your flexibility can be fueled by theory, experience, and intuition. There has been some misconception, for example, that the Othmers claim everyone is over-aroused and needs low frequency neurofeedback. Anyone who repeats this claim has not read their works or attended their trainings. I do believe most people are over-aroused and your reward frequency will move lower and lower with good results. Why are they over-aroused and often exhausted (appearing under-aroused)? According to Prof. Russell Blaylock, M.D., unlabeled excitotoxins are ubiquitous in the American diet and causing neurophysiological havoc. Additionally, unlike most civilized countries, Americans don't take a 2-6 week vacation every year. They push themselves and work through their rest time. Then there are the remembered and forgotten traumas (surgery under anesthesia, head injuries, bullying, abuse). Many people are a boiling cauldron of fight or flight hormones precariously balanced by pre-death (real or imaginary) opiods and endorphins. Still, some people eventually reach exhaustion, or are born under-activated. They may require an increase in reward frequency as well as serious life-style counseling. Again, work within the scope of your license. http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 4 of 10 Q: Is there a single low frequency protocol or many? [ Top ] A: It is likely that there are as many protocols as there are practitioners. Low-frequency work, whether it is low frequency neurofeedback, slow cortical potential training, or transcranial direct current stimulation (tDCS), attempts to strengthen and improve the control and functioning of these energies. Protocols are only useful as a place to start. As an analogy, we didn't learn the instruments, levers, and pedals in a car just to drive in the unoccupied parking lot. We learned them so that we could negotiate life's surprises on the freeway. This is where the real learning begins. This is why it is called a "practice". Seriously...study and practice this technique for a few months...then write your own. If not for others, then for yourself. When I started, my mantra was "where are the protocols." I think I have learned that all around there are innumerable gems of information (wisdom) that help me help my clients. I am not looking for an approach that will necessarily help me treat your clients, I just want an approach that will help me be successful with mine. Q: How can I learn more, or get training? [ Top ] A: If you are in the United States and have a Nexus, then you have probably studied with John Anderson www.neurofeedbackinstitute.com.. John has had an excellent understanding of all things neurofeedback and has used low-frequency work as part of his practice for many years. He is also a wonderful mentor and resource. John offers an advanced Nexus workshop through Stens Corporation where you can learn to develop and test your own Nexus channel sets and screens. The true pioneers in this area are the Othmers, Siegfried and Sue www.eeginfo.com. Siegfried is a physicist as well, and appears to be the theorist. Sue is a clinician. Their instructional DVDs and written materials are very useful. Take their courses, read their materials, talk to people who have tested their ideas, then test them yourself, then ask more questions. Sue Othmer has produced a wonderful Protocol Guide which she keeps updated. Her DVDs on PTSD are also very important resources especially if you intend to use both low frequency bipolar work and alpha theta in your practice. If you can't get away to courses, remember Sir William Osler's advice, "Never waste time by day listening to that which you can read by night." The internet library is open! If you cant afford $30 each for research articles of undetermined value, then get a thin portable scanner and take your laptop to the nearest university. Or find an enrolled student with internet access to the library and do some searching and downloading with him or her. I am also a BCIA certified mentor and available for consultation at [email protected]. Q: What type of equipment and software is required for low frequency neurofeedback? [ Top ] A: I believe that the Othmers did much of their early low frequency neurofeedback using Bioexplorer software and the NeuroAmp. In 2008 they released a hardware and software package, Cygnette, designed according to their specifications using a programming environment called BioEra. The complete Othmer system is very reasonably priced and has the support of the pioneers in the field. I believe, however, that it is limited to neurofeedback and does not allow extensive reconfiguration. John Anderson has used as many or more different systems than anyone. He has been using Nexus exclusively since its introduction several years ago. Both Cygnette and Nexus allow you to work down to the 0.01 - 0.10 Hz range that is described in the literature. With other systems you may not be able to work as reliably at such low frequencies. Check with your vendor or manufacturer. Of equal importance, however, is the software. An important aspect of the low frequency protocol, as developed by the Othmers, is the use of multiple inhibits (discussed below). To summarize, you need an amplifier with a stable linear response all the way to DC, and you need software that includes the ability to probram multiple inhibit bins and coordinate their feedback. If you use other approaches in your practice, if you need complete flexibility and programmability, and especially if you want to integrate such peripheral measures as heart rate variability and GSR/EDR into your sessions, the Nexus is your best option at this time. If you have a Nexus and want to approximate the software resources used by the Othmers, then you will either have to design and test your own screen and channel set, or get the ones offered at this website. Our design was tested, used clinically, and optimized for over a year before being offered to other Nexus users. Q: Why are multiple inhibits used? [ Top ] A: The nature and purpose of multiple inhibits are often misunderstood. I would recommend you read the following 2 paragraphs, taken directly from our protocol guide, and make certain you understand it before going on. "Another feature of the low-frequency work, as originally implemented by the Othmers, is the use of multiple inhibit bins. In traditional amplitude training, it is common to have a “high inhibit” instrument to discourage excessive beta activity or EMG activity. Suppose you have a high inhibit which is set for the range of 18-30 Hz. You observe that your client has 20 Hz activity that is usually above 5 microvolts but occasionally above 10 microvolts. You could set an alarm threshold so that http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 5 of 10 any signal above 10 microvolts between 18 and 30 Hz gives a warning signal. However, your client may also have a repeated 4 microvolt activity at some other frequency, say 28 Hz, that is more clinically significant. Unfortunately, it will not trigger the “high inhibit” because the high inhibit is set to 10 microvolts across the entire 18-30 Hz range. Unfortunately, in order to capture the 28 Hz 4 microvolt signal, you can’t just lower the general 18-30 Hz threshold from 10 microvolts down to 4 microvolts because the 20 Hz signal is usually above 5 microvolts and would set off the alarm all the time." "One way to capture more rogue excursions is to have multiple inhibit bins, each spanning 4 Hz. For example, you could have an 18-22 Hz bin, a 22-26 Hz bin, and a 26-30 Hz bin. The 18-22 Hz bin could have a threshold of 10 microvolts to catch its rogue excursions, and the 26-30 Hz bin could have a threshold of 4 microvolts to catch its rogue excursions as well." In Llinas' 1999 article on thalamocortical dysrhythmia [ 5 ] he reports observations on clients with a variety of conditions including neurogenic pain, depression, tinnitus, epilepsy, obsessive-compulsive disease, dystonia and spasticity. In general he found increased cortical power expenditure across the entire spectrum in patients compared to controls. Patients also showed excessive hypercoherence across all frequencies compared to controls. This relationships are shown in the chart (after Llinas) below. Excess cortical power of patients vs controls (Left); Normal coherence 5-35 Hz in controls (Mid); Hypercoherence 5-35 Hz in patients (Right). In general, low frequency bipolar neurofeedback is designed to break apart hypercoherence (using a bipolar montage) and to reduce excessive cortical energy expenditure (using multiple inhibits). Q: Is the Nexus (with Biotrace) a good system for low-frequency neurofeedback? [ Top ] A: The Nexus is possibly the only alternative to the Othmers' system at this time. Both are DC amplifiers which means they don't block the DC and only pass alternating current the way older systems do. The Othmers's system has been designed ground-up to do this sort of work, and is very affordable. As far as I know, the ability to write your own protocols or incorporate peripheral measures is limited on their system. Still, if you need a second system and want to work with the most experienced group in low frequency protocols, their system is a good choice. If, however, you want to do other types of neurofeedback (and there are many) or biofeedback and heart rate variability, or if you just want to observe physiologic stress indicators during your low frequency work, then you have no other choice but the Nexus. It's software is fully programmable, it includes bio- and neurofeedback capability, is completely isolated from the computer by Bluetooth (for client safety), and has a variety of features you would expect from a system with such robust capabilities. In my opinion, the main weakness of the Nexus, up to now, has been its lack of clinical modules available as add-ons. The Nexus comes with a variety of screens for different modalities, and more are offered at the Stens' workshops. But if you have a particular application in mind, or a particular way you want to work, your only option has been to learn to design screens and channel sets yourself, or hire someone to make them for you. With the robust programming interface offered by Nexus you can expect to see more clinical applications and suites become available. Q: How do I install the Nexus Low Frequency neurofeedback module on my computer? [ Top ] A: This is completely described in the user guide that comes with your module. If the user guide is not yet posted on this website, it will be soon. The short, quickstart answer will be offered to your question. To install the module you need to know how to use windows to find out where your Biotrace software is installed. You will need to know how to insert a CD in your computer and look at the file directories on the CD. Finally, you will need to drag (copy) files from the CD to the correct sub-folders in your Biotrace folder. If you have not felt the need to do this type of folder based work on your computer yet, now is the time to start. If you want to be able to add your own choice of animations and sounds, this is the way. If you want to make certain that your carefully created screens, documents, patient files, etc., are all safe when the next disaster strikes, then you need this information. Ask a friend if you need to, or get a recommendation for a Windows' tutorial book. It will payoff. I promise. Your Nexus software is called BioTrace. If you installed it yourself then you know where on your computer it is located. It is usually on your main hard drive, called drive "C:". Drive C: has a number of folders in it which contain data, programs, etc. There is one folder called Biotrace. In that folder you will find the actually computer programs that makeup the Nexus software. Also in that folder you will http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 6 of 10 find subfolders called "Audio", "Channels", "Screens", and "Video" among others. In order to install the low frequency protocol or any of the other products on this website, you need to insert your product CD in your computers drive. On that CD you will also find folders with names "Audio", "Channels", "Screens", and "Video". Simply drag the contents of the folders on your CD into the similarly named folders on your hard drive. All your new screens from your product disk are setup to have no feedback enabled. This is to ensure that when you first run a sample file you will see feedback from your video, audio or DVD source. Then you can turn on the feedback of each instrument and adjust its effect until it is what you want. Don't forget then to save your screen, preferably under a different name. That way it will be available just the way you like it when you next need it. Q: Why are there 7 different screens in the Nexus low frequency neurofeedback module? [ Top ] A: Some people use a second monitor for patient feedback in their office. Then they may use a single screen laptop in other situations. When using a single screen setup you may need or prefer to have your client sitting to your left or to your right. The seven screens are included in order to enable you to select the one that works best for you. Furthermore, a screen with a video file playback instrument cannot be used to play a DVD for feedback, and vice versa. They require different screen instruments, i.e., they require different screens. So you have been give four screens from which to select if your computer does not have a second monitor for your client. Those four screens have 2 screens for DVD feedback, one for the client sitting to your right and one for the client sitting to your left. And there are two screens for video file playback, one for the client sitting to your right and one for the client sitting to your left. There are three screens provided for you when you use a second monitor. The main screen is to be used on your monitor. Then there is a DVD playback screen and a separate video playback screen for the client's monitor. Q: During a neurofeedback session can I alternate other screens with the low frequency screens? [ Top ] A: Not unless you have verified that each screen uses the same channel set. The low frequency neurofeedback module uses a different channel set than any other screens you might have. Remember, channel sets are lists of modifications to the raw data that your system uses to provide data to the instruments on your screen. All the screens that come with your Nexus use the same default channel set. So you can switch screens on the fly and know that each screen processes the raw data from the amplifier in the same manner. If you use a different channel set for one screen then you must have that same channel set available when you load another screen during a session. If you want to be able to "hot-swap" screens during a session, make certain the channel sets are compatible. This is an advanced topic you can explore in the Nexus user's manual, or at an advanced seminar with John Anderson. Q: How do I fine tune my low frequency screens during a session? [ Top ] A: Your new nexus screens come with each instrument set to provide no feedback. This is so that when you first replay a sample session, say John Sample, you will see the video or DVD feedback provided. Then you can right click on the reward instrument and the inhibit instruments one by one, go to feedback settings, and enable the feedback. Each of the multiple inhibits is already set up to provide (once you enable feedback) five minutes of autothresholding. The auto-threshold will be set at the amplitude where the signal in the particular bin stays below the threshold 97% of the time. That way feedback is being inhibited only when the voltage in a particular bin is higher than it usually is 97% of the time. After 5 minutes you can adjust the threshold during the session to suite the needs of you and your client. The feedback of your reward instrument also comes set to "not enabled." Again, this is so that when you replay a sample session, you will see feedback. When you are ready, right click the instrument, select feedback and thresholds, and enable the feedback. During a session you often observe that the client's reward amplitude drops down and stays down for a while. This does not mean they will not find their way back up again. In fact, often, if you watch the cascading spectral display, you will see that they appear to be discovering a new way to bring the voltage back up and get the reward. During these periods where the reward has dropped below the threshold, all feedback stops. I tell my clients early in the session that at times I will lower the threshold. I tell them that I have not lowered it because I don't think they will bring the level back up, but because when they are below threshold, all feedback stops. Thus they are not receiving feedback about rogue excursions caught by the inhibit bins. By lowering the threshold you can reinstate feedback to the point that they will be alerted when a rogue excursion occurs. You can then continue to raise the threshold as their response increases. As an alternative, you can associate a midi "chime" with each inhibit bin, so that regardless of the state of the video feedback, an alerting chime will sound when a rogue excursion occurs. Part of the learning curve with the Nexus, as with any other biofeedback device, is learning to quickly set the parameters of the instruments so that your client recieves the maximum information with the minimum distraction. Q: How do I know what training frequency to select? How do I know when to change it? [ Top ] A: This is discussed in depth in the protocol guide accompanying the low frequency neurofeedback screens. If you have not seen this protocol used at a seminar or by another clinician, then you should contact someone with whom to discuss issues both before and after they arise. In general for the average client you can start at either C3-C4 or T3-T4 and train bipolar at 12-15 Hz for several minutes. Ask http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 7 of 10 the client if anything has changed. Usually the answer is no. In the manual you will be given some advice on how to decide if your client is over- or under-aroused when they first present. Depending on your assessment you change the frequency bin by one hertz and try two more minutes of training. Continue in this manner until the client notices a difference. Explore gently this way at first. Later, after practice, you may start at different frequencies as needed. Remember that at the first session your client is being trained at perhaps 5 or more different frequencies until they find one where there is a noticable balance between relaxation and awareness-arousal. Therefore, the remainder of that day and night they will be experiencing the sequelae of multiple trainings. Have your client keep track of any unusual cravings, moods, changes in energy, or changes in sleep and dream patterns. Next visit you will most likely start around the frequency where you left off. For starts, the protocol guide will show you the possibilities. Your attention to your client's state and your growing experience will help you determine the specifics during a session. Learning to adapt your equipment and sessions to the needs of your client is an art based on science. After reading the manual accompanying your Nexus Low Frequency Module, consult with your mentor, if he or show is familar with the low frequency work. I highly recommend carefully studying Sue Othmer's protocol guide and PTSD DVDs, and taking advantage of some of the advanced training at www.eeginfo.com Q: Does the Nexus Low Frequency module work with the Audio-Visual Library for Biofeedback? [ Top ] A: Yes. The Audio-Visual Library for Biofeedback [ located here ] comes in four versions depending on the type of equipment you use. Make certain you have the Nexus version. The AV Library (Nexus) version includes 14 custom screen designs that should meet most of your standard biofeedback and neurofeedback work. It does not contain screens for low-frequency protocol or for alpha-theta synchrony; however, with the AV-Library screens you can do one channel alpha-theta work with a single reward band (usually 5.5 - 8.5 Hz) and standard low and high inhibits. The AV LIbrary has 840 individual puzzles with audio, arranged into 14 categories. The puzzles are interesting to the client (the client chooses the category) but are not overstimulating such as games can be. There are three DVDs in the library: DVD #1 has all 840 puzzles in high resolution suitable for use on a second monitor. The second DVD has all the puzzles in medium resolution with sound, and also in medium resolution without sound in case you want to use the audio differently. The third DVD is a standard video DVD with all the puzzles available from a menu. It is to be played from your computer's DVD player during the session. Q: How do I select video and audio files to use for feedback? [ Top ] A: This is a personal decision based on your style and your client's age, cooperativeness, and interests. One of the reasons I like the "Audio-Visual Library for Biofeedback" is that it has 840 different puzzles arranged into 14 categories (such as airplanes, cars, flowers, people, space, trains, etc.). The music is interesting and of relatively constant volume which helps when you use proportional audio (i.e., the feedback information is contained in the volume of the audio). This can keep the client engaged for a number of sessions. To select video and audio files they must be in the appropriate folder, "audio" or "video" located under your main Biotrace folder on your hard drive. Once they are in the folders they will appear when you select a type of feedback for an instrument. Complete instructions are located in your Nexus user's manual which can be accessed from the biotrace program itself by looking under Help on your screentop menu bar. Video files are very large. You should never allow your hard drive space to become less than 2 times the amount of RAM in your computer or basic computer operations will become compromised. If you are short on disk space you run the A-V library from your DVD drive. You can run any other DVD as well. You may enjoy collecting a set of DVDs that work for your clients. Among my favorites are "The Dog Whisperer", "Animusic", and "Cirque de Soleil". Don't forget to make backup copies of your favorite DVDs so you will have working disks when you need them. Q: Why do you discuss a connection between low frequency neurofeedback and mindfulness meditation? [ Top ] A: This is also discussed in more detail in the accompanying protocol guide. In his important book [ 6 ] "The Mindful Brain", Daniel J Siegel, of the UCLA Mindful Awareness Research Center, defines mindfulness as awareness of the modifications of the mind accompanied by the attitudes of "curiosity, openness, acceptance, and love." With low frequency work, and with skilled guidance and mirroring, we help our clients become aware of their own modifications of mind accompanied by the very same attitudes, although we might substitute the word appreciation for love. Siegel also states "Mindfulness meditation... is thought to be especially important for training attention and letting go of a strict identification with the activities of the mind as being the full identity of the individual." It is how we pay attention to "the dance between the mind and brain." It is "the self-regulation of attention ...allowing for increased recognition of mental events in the present moment." Even in neurofeedback we often give inadequate support to the phenomena of neuroplasticity [ 7 ]. "How we focus attention helps directly shape the mind." And we may not yet realize the extent to which equilibration through feedback is essential for coordination of mind, brain, and physical reality [ 8 ]. "This form of awareness may directly shape the activity and growth of the parts of the brain responsible for our relationships, our emotional life, and our physiological response to stress." [ Siegel, op. cit. p. 6 ] "How we pay attention promotes neural plasticity." Siegel also points out that mindfulness meditation particularly affects the medial prefrontal cortex and anterior cingulate. Our protocol guide discusses the use of bipolar training at Fp2 and T4 in cases where preliminary training has lead to emotional distress. An interesting discussion of this network appeared in Dec 2007 in the journal Social Cognitive and Affective Neuroscience[9]: "Functional connectivity analyses further demonstrated a strong coupling between the right insula and the mPFC in http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 8 of 10 novices that was uncoupled in the mindfulness group. These results suggest a fundamental neural dissociation between two distinct forms of self-awareness that are habitually integrated but can be dissociated through attentional training: the self across time and in the present moment." Q: Is their a connection between low frequency neurofeedback, slow cortical potential training, and transcranial direct current stimulation (tDCS)? [ Top ] A: This has been an area of interest for at least a decade or more. I am not well familiarized with the literature. So my opinion is pure speculation. I know that neurofeedback has gone from largely medium frequency training (alpha, SMR, beta, etc.) for attentional issues to also training the infra-slow frequencies. In fact, last year Evian Gordon's Lab in Australia discovered a new biological marker for ADD in the infra-slow, 0.01 - 1 Hz range. It appears that ability to shift phase relationships at these frequencies (such as is done with bipolar low frequency training) is crucial for assembling such event related potentials (ERPs) as the P3b. The ERPs are the signatures of the progressive processing of data passing through the brain. In fact, the hallmark of successful cortical aging in the elderly is the retention of a robust P3b in response to novel stimuli. P3b has also been shown to be shaped by mindfulness training, with the result of more efficient utilization of scarce cortical resources under task. In Germany Birbaumer has for decades been employing and developing direct training of the slow cortical potentials. In my mind, the origin of these slow cortical potentials has not been completely described. Clearly there is a role played by dipoles created by neuronal activity. There is also a role played by the glial cells who direct neuronal activity through the release of ions which change the neuronal environment. Jay Gunkelman states that the neurons represent the brain, while the glial cells represent the mind. With respect to the way the mind prepares the brain for attention or intention by shifting the cortical electronegativity, research has been building in the use of transcranial Direct Current Stimulation (tDCS) to directly create similar changes. Much work recently has been undertaken at Beth Israel Hospital at Harvard. You can see about 150 interesting abstracts on tDCS at www.growing.com/mind/tDCS elsewhere on this website. Other studies using fMRI have detected electrical rhythms in the 0.10 Hz range in the brain that may be modulated by cardiac cycles. It has been suggested that cardio-respiratory resonance (e.g., from heart rate variablity training) provides a base rhythm for nesting of higher frequency activities in the brain. Q: Where can I find a bibliography about low-frequency neurophysiology so I can read and make up my own mind? [ Top ] A: I have not seen one yet myself. There are frequent discussions in the literature, but none that tie it all together at this time. I suggest you do what many of us are doing. Continue to search pubmed.gov for research dealing with infra-slow EEG, slow cortical potentials, default mode networks, glial cells, consciousness etc. Many of the neurofeedback protocols and electrode placements can in fact be derived from the recent literature. I will be posting more on this topic in the near future. Q: Is there a role for low frequency neurofeedback in the treatment of post-traumatic stress disorder (PTSD)? [ Top ] A: My opinions on PTSD are posted elsewhere on this website [ here. ] Alpha-theta training remains prominent in the minds of many neurofeedback practitioners. It is likely to become more powerful as more information on the role of the default mode network, the narrative process, memory, and self-awareness provide rationale for neurofeedback protocols. Arousal (under and over) is always an issue in PTSD. Low frequency protocol and alpha-theta protocol can work hand in hand in keeping a client within his or her window of tolerance while allowing the client to reestablish a narrative and learn self-regulation. Nexus now has an Alpha-Theta Synchrony Module with user guide [ here. ] Q: Are you teaching the Othmer Protocol? Can I do the Othmer Protocol with these screens? [ Top ] A: Many seminars, mentors, and beginners do attempt to describe the Othmer protocol. It is one thing to be comfortable dialing your software in to the infra-slow frequencies and working with your client's responses. However, if you want to say you do the Othmer protocol you must study with the Othmers. They even offer certification to their trainees www.eeginfo.com. They have contributed very much to the neurofeedback community as well as the public, and it is only they who can teach the Othmer protocol, which, by the way, continues to evolve. While I describe the Othmer protocol in my manual, only they can make certain that you know and understand it. To the best of my knowledge the Nexus screens I offer give you the same basic functionality as the Othmer's systems provide. In addition you get the peripheral measures. Recently the Othmer's have stated that they have started training at 0.001 Hz on occasion. The most current clinical fMRI, SCP and default mode network (DMN) studies rarely discuss frequencies lower than 0.01 Hz. Now, 0.01 Hz is a cycle approximately every 1.5 minutes, and 0.001 Hz is a cycle approximately every 15 minutes, much longer than the amount of time over which a client is trained in typical low frequency work. In my experience, if you go as low as 0.01 Hz and feel the client has still not achieved a stable and beneficial balance between arousal and relaxation, you can simply change your filter parameters (such as order). This will provide an additional different challenge to the nervous system. The current DC EEG literature states that it is robust phase dynamics between 0.01 and 0.10 Hz that plays a key role in cognition and sensory discrimination [ 2 ]. http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 9 of 10 Q: How then does your protocol differ from the Othmers'? [ Top ] A: My approach to low frequency work comes more from my initial study of slow cortical potentials, the infra-slow EEG and event related potential literature, and now the mounting studies on the default mode network (DMN). These studies (to be discussed later) strongly suggest that infra-slow frequency dynamics provide a crucial basis for cognition, sensory processing, and allocation of cortical resources. At this time they can not be assessed using QEEG (quantitative electroencephalogram) which is the current standard for neurofeedback protocol determination. My approach involves the use of peripheral measures, in particular heart rate variability and EDR, to monitor client reactions during the sessions and steer the protocol. Siegfried Othmer has said "I think the peripheral measures will clearly help to steer the training." [ 10 ] The importance of peripheral measures, especially the power spectral density of the heart rate variability, is that they help identify when a person exceeds his or her "window of tolerance". Because low frequency phase dynamics influence sensation as well as cognition, a client can develop a perception or mind set associated with a previous trauma. The client can begin an autonomic shift into hypersympathecotonia (fight or flight and the low frequency component of the HRV spectrum) or shift into hyper-parasympathecotonica (dissociation, the higher frequency components of the HRV spectrum). Even with the additional instrumentation, the observation and management of client intolerance is an art which must be studied and practiced. The re-establishment of the client within his or her window of tolerance can be most easily achieved through attention to functioning of the ventral myelinated vagus (cf. S Porges). The ventral myelinated vagus serves the social engagement system, in particular, facial expression, vocal expression, ventilation-perfusion balance in the lung, and even the mechanical properties of the middle ear and the ability to tune into the human voice. I discuss this more fully in my section on PTSD. Q: What is the "red thread" that you discuss? [ Top ] A: I noticed that infra-slow frequency neurofeedback and alpha-theta synchrony neurofeedback were very different than standard amplitude or coherence neurotherapy. As Hammond and Kirk pointed out [ 4 ], they were where most of the uncomfortable neurofeedback reactions occurred. As I investigated and worked with these reactions I realized that most of them were related to prior traumatic events. Usually there was some aspect of the trauma which had not been integrated into the client's narrative memory. As the network dynamics were gently stressed with neurofeedback exercises, partial awareness of a component of traumatic memory would come into focus. This vaguely perceived threat can cause a client to revert to a previous primitive (non-executive) pattern that had been ingrained as an essential survival resource. The "red thread" refers to the persistence of reactions to events that were overwhelming. Obviously, what overwhelms an infant and what overwhelms a resourceful adult are magnitudes apart. Nonetheless, unless the person knows, or is shown, self-regulation, the self becomes disorganized [ 11 ]. Current literature on default mode networks and the anti-correlated attentional networks (citations to come) suggests that T3-T4 bipolar infra-slow training can regain dissociated sensations and memories, and alpha-theta synchrony training (Fz-Pz) can integrate the phenomena into the self narrative. Thus I believe there are two broad types of neurofeedback practices and protocols. In one type we may be dealing with epilepsy, traumatic brain injury, ADD, and the EEG phenotypes that have been popularized by Jay Gunkelman, et al. In these cases appropriate protocol selection is based on EEG or QEEG evaluation. In another type of case we may be dealing with a "red thread" phenomena. The client approaches traumatic memory and unintegrated aspects of self, and the therapist facilitates self-regulation. Schore described the mother teaching self-regulation to the overwhelmed infant by acting as an auxiliary cortex. Could the neurofeedback process act as an "auxiliary cortex?". Could it be in these "red thread" cases that the moment-by-moment compassion and skill of the operator is as important as the protocol itself? Learning to handle a "red thread" reaction requires skills beyond what are needed to merely hook up an amplifier and select a protocol. The initial reactions of the client are minimal and require a trainer who is paying attention. This may be the biggest hurdle. Peripheral instruments help. Initially there is instrumental sign of autonomic change, then subtle changes in facial and vocal expression, breathing pattern, postural bracing, and social engagement. These are all phenomena that are normally mediated by the myelinated ventral vagus nerve (cf. Porges polyvagal theory). When a client goes beyond his window of tolerance, executive control of the ventral vagus gives way to reactions by the paleo-mammalian limbic (herd) brain, or the more archaic reptilian reflexive (ritual) brain (cf. McLean's Triune Brain). Both these latter brains operate without the executive control and hemispherical specialization that mark the network architecture and resources of healthy humans and great apes. These states are severely reactive and archaic. Their automatic persistence in any form marks a potentially devastating loss of human capacity, as we often see so clearly in the victims of torture and disaster. The crux of my method is to facilitate the client observing these reactions with attitudes of curiosity, acceptance and openness. At the same time effort is made to re-engage the ventral vagal social engagement system. At the same time it is important to recapture the resources of the hardwired action-behavior systems such as curiosity, play, bonding, exploration, care, etc. The astute clinician can mirror subtle aspects of the client's behavior, thus facilitating empathy and engagement. These and other techniques for neurotherapists are discussed elsewhere [ 12 ]. http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012 Neurofeedback - Low Frequency Protocol Frequently Asked Questions Page 10 of 10 Please submit questions and comments to [email protected] References: 1. Othmer SE & Othmer S. Interhemispheric EEG Training: Clinical Experience and Conceptual Models. In Evans JR (Ed) - Handbook of Neurofeedback. Haworth Press, NY, 200, p. 109-136. 2. Monto S, et al Very Slow EEG Fluctuations Predict the Dynamics of Stimulus Detection and Oscillation Amplitudes in Humans The Journal of Neuroscience, August 13, 2008, 28(33):8268-8272 3. Broyd SJ, et al. Default-mode brain dysfunction in mental disorders - A systematic review. Neuroscience and Biobehavioral Reviews 33 (2009) 279-296 4. Hammond DC, Kirk L. First, do no harm. Adverse effects and the need for practice standards in neurofeedback. Journal of Neurotherapy. Vol 12(1) 2008. 78-88. 5. Llinas R. Thalamocortical dysrhythmia: A neurological and neuropsychiatric syndrome characterized by magnetoencephalography. Proc. Natl. Acad. Sci. 96, 15222-15227. 6. Siegel DJ. The Mindful Brain. W.W. Norton Company, NY, 2008. 7. Doidge N. The Brain that Changes Itself. Penguin Books, NY, 2007. 8. Buzsaki G. Rhythms of the Brain. Oxford University Press, NY, 2006 9. Farb NA, et al. Attending to the present; mindfulness meditation reveals distinct neural modes of self-reference. Social Cognitive and Affective Neuroscience, 2007 Dec;2(4):313-322 10. Personal communication, Dec 16, 2008. 11. Schore AN. Affect dysregulation and disorders of the self. W.W. Norton & Company, NY 2003 12. Dailey D. Networks and Neurofeedback: Mechanisms or Metaphors? Unpublished manuscript. 2009. http://www.growing.com/mindware/nexus/lowfrequency/NXLFFAQ.htm 6/20/2012