Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
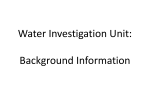
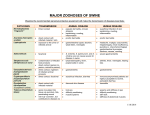
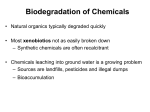
MAJOR ARTICLE Diagnostic Accuracy of Stool Assays for Inflammatory Bacterial Gastroenteritis in Developed and Resource-Poor Countries Christopher J. Gill,1,2,4 Joseph Lau,2 Sherwood L. Gorbach,3,4 and Davidson H. Hamer1,4 1 Center for International Health and Development, Boston University School of Public Health, and 2Division of Clinical Care Research, 3Department of Family Medicine and Community Health, and 4Division of Geographic Medicine and Infectious Diseases, Tufts–New England Medical Center, Boston, Massachusetts Because acute bacterial gastroenteritis is often inflammatory, rapid stool assays that detect intestinal inflammation might be used to distinguish between bacterial and nonbacterial gastroenteritis. We performed metaanalyses to determine the discriminatory power, in developed and in resource-poor countries, of rapid stool assays that test for lactoferrin, fecal leukocytes, fecal erythrocytes, and occult blood. In developed countries, the area under the summary receiver operating characteristic curve (AUC/SROC) was 0.89 for fecal leukocytes and 0.81 for occult blood. In resource-poor countries, the AUC/SROC was 0.79 for lactoferrin, 0.72 for fecal leukocytes, 0.63 for occult blood, and 0.61 for fecal erythrocytes. In developed countries, positive and negative likelihood ratios (LR+ and LR⫺, respectively) for fecal leukocytes were 4.56 and 0.32 when a threshold of 15 cells/high-power field was used, compared with 2.94 and 0.6 in resource-poor countries; for lactoferrin, LR+ was 1.34 and LR⫺ was 0.17 in resource-poor countries when the threshold was an agglutination rating of “+” and a dilution of 1:50. In developing countries, rapid stool assays performed poorly, whereas in developed countries, tests for fecal leukocytes, lactoferrin, and occult blood were moderately useful and could identify patients who were more likely to benefit from empirical antibiotic therapy. More than 1 billion cases of acute diarrhea occur worldwide each year [1, 2]. Given the limited availability of rapid pathogen-specific tests and the 24–48 h required to process stool cultures, patients with acute community-acquired gastroenteritis are often treated empirically with antibiotics. However, most acute diarrhea is caused by pathogens or agents that do not respond to antibiotics, such as viruses, preformed bacterial entero- Received 14 January 2003; accepted 28 March 2003; electronically published 22 July 2003. Financial support: Agency for Healthcare Research and Quality (National Research Service Award training grants 5T32AI0738 and T32 HS00060-09). Reprints or correspondence: Dr. Christopher J. Gill, Center for International Health and Development, Boston University School of Public Health, 710 Albany St., Boston, MA 02118 ([email protected]). Clinical Infectious Diseases 2003; 37:365–75 2003 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2003/3703-0008$15.00 toxins, and most parasites [1]. Misapplied antibacterial therapy places patients at risk of medication-related adverse events, contributes to the emergence of antimicrobial resistance, and represents a needless expenditure of limited resources in poorer countries. Reliable identification of patients with acute gastroenteritis that would be amenable to antibacterial therapy at time of first contact remains a formidable but worthy clinical challenge. Invasive forms of bacterial gastroenteritis often cause intestinal inflammation, whereas most forms with viral, parasitic, and toxin-mediated etiologies do not [3]. Consequently, rapid stool assays that identify by-products of intestinal inflammation in stool might identify patients who are more likely to benefit from antibiotics. Rapid stool assays currently available include microscopic examination for leukocytes and erythrocytes, guaiac-based fecal occult blood tests, and a rapid im Stool Assays for Bacterial Gastroenteritis • CID 2003:37 (1 August) • 365 munologic assay for fecal lactoferrin (Leukotest; Techlabs) [3–5]. Published estimates of the diagnostic accuracy of these tests vary considerably. Although an earlier meta-analysis concluded that the lactoferrin assay was the preferred test [6], this analysis did not provide summary estimates of the various assays’ sensitivities and specificities or the area under the summary receiver operating characteristic curve (AUC/SROC), both of which are needed to judge the overall value of diagnostic tests. Perhaps more important, this analysis combined studies from both resource-poor and developed countries without considering how the disease spectrum prevalent in each setting might influence the diagnostic performance of the tests. Accordingly, we conducted meta-analyses of studies that have evaluated the diagnostic accuracy of rapid stool assays for distinguishing bacterial from nonbacterial gastroenteritis. In addition to determining the most accurate test, we wished to understand how the performance of these assays varied with the prevailing epidemiologic setting in which the study was conducted. METHODS Search strategy. We sought studies that measured the diagnostic accuracy of tests for lactoferrin and occult blood and microscopy for fecal leukocytes and erythrocytes for patients who presented with acute, community-acquired bacterial gastroenteritis of ⭐7 days’ duration. We searched the MEDLINE database and the Cochrane Database of Abstracts of Reviews of Effectiveness for studies published from 1966 through 2002 and conducted secondary and tertiary searches for additional articles within the bibliographies of retrieved articles [6]. Relevant studies were evaluated using the criteria listed below. Failure to satisfy any of the inclusion criteria resulted in exclusion from our analysis. Inclusion criteria were the following: 1. Peer-reviewed journal article 2. Published in English 3. Primary data study (i.e., no review articles, meta-analyses, systematic reviews, or expert opinion papers, except as sources for additional bibliographic references) Exclusion criteria were the following: 1. Published only in abstract form 2. Published only as a letter to the editor 3. Personal communication 4. Study of patients with autoimmune inflammatory bowel disease 5. Study of Clostridium difficile colitis 6. Limited to specific pathogens 7. Did not include cultures for Campylobacter species Although most of these criteria are self-explanatory, several 366 • CID 2003:37 (1 August) • Gill et al. require clarification. Studies that focused on C. difficile were excluded because the vast majority of cases of C. difficile enteritis are hospital rather than community acquired. Campylobacter species are common causes of inflammatory enteritis in both developed and resource-poor countries [7–10]. Recent statistics show that Campylobacter species cause 38%–50% of all cases of culture-positive community-acquired gastroenteritis in the United States [11–14]; however, surprisingly, campylobacters were not recognized as enteric pathogens before the late 1970s [15]. Consequently, many early rapid stool assay studies were conducted before Campylobacter cultures became routine and risked misclassifying the positive assay results for the substantial proportion of patients who had campylobacteriosis as false positive, resulting in inaccurate estimates of sensitivity and specificity. Studies retained after application of inclusion and exclusion criteria were next evaluated using the following validity criteria. These were designed to select studies with a focus on community-acquired gastroenteritis that were amenable to metaanalysis and to minimize the potential for bias: 1. Data collection was prospective. 2. Case definition was provided. 3. Case definition was compatible with our case definition (acute-onset diarrhea of ⭐7 days’ duration). 4. Study focused on community-acquired diarrhea. 5. Study provided either sensitivities and specificities or raw data allowing these to be calculated. 6. Case and control subjects all had diarrhea and were drawn contemporaneously from the same source population. 7. Stool culture was used as the reference standard. 8. Test thresholds for positivity were defined for each assay. (For fecal WBCs and RBCs, this is the number of cells per high-power field [HPF]. For lactoferrin, the test threshold is varied both by adjusting the ratio of stool to saline [dilution range, 1:50 to 1:200] and by judging the subjective intensity of the agglutination [rated “+,” fine agglutination visible against a milky background; “++,” agglutination visible against a white background, with a visible rim; or “+++,” agglutination visible against a clear background, with a clear rim]. Occult blood tests are assumed to provide dichotomous results: any color change vs. no color change.) Reference standard. To learn which stool assays are useful for identifying cases of diarrhea that are theoretically amenable to empirical antibiotic therapy, we defined our “disease-positive” reference standard as a stool culture on which any of the following pathogens grew: Campylobacter species, Shigella species, Salmonella species, Yersinia enterocolitica, non-cholerae Vibrio species, Plesiomonas shigelloides, Aeromonas hydrophila, and diarrheagenic Escherichia coli (these were enterotoxigenic E. coli [ETEC] in almost all cases). Stool assays demonstrating viruses, C. difficile toxin, or parasites or parasite ova or which had no growth were classified as “disease negative.” Patients coinfected with pathogens from “disease-positive” and “disease-negative” categories were excluded from our analysis, because which pathogen is responsible for a positive test result cannot be determined (!1% of subjects were excluded from our study for this reason); patients infected with multiple pathogens from the “disease-positive” category were considered to be disease positive. Sensitivity analysis for ETEC. The fact that some forms of bacterial enteritidis are noninflammatory and some forms of nonbacterial enteritidis are highly inflammatory may cause assays to misclassify certain pathogens. ETEC cause acute antibiotic-treatable diarrhea that is noninflammatory and hence unlikely to cause a positive assay result [3]. Because ETEC are common agents of bacterial gastroenteritis, we did analyses in which cases caused by ETEC were categorized alternately as disease positive and disease negative to see how this affected test performance. Statistical analysis. True-positive, false-positive, true-negative, and false-negative values were used to calculate sensitivities, specificities, and likelihood ratios (LRs). We calculated 95% CIs according to Fleiss’ method [16]. For studies that provided only summarized sensitivity and specificity data but no raw data, we used the cohort size and culture-positivity rate to back-calculate true-positive, false-positive, true-negative, and false-negative values. Positive LR values (LR+) were calculated using the formula [sensitivity/(1 ⫺ specificity)]; negative LR values (LR⫺) were calculated using the formula [(1 ⫺ sensitivity)/specificity]. Multiplying pretest odds for a disease by LR+ or LR⫺ (depending on whether the test result was positive or negative) yields posttest odds for that disease. By definition, a test with an LR+ or LR⫺ of 1.0 is worthless, because it does not alter posttest odds. Although there is no absolute threshold, an LR+ of 2.0 and an LR⫺ of 0.5 are considered the minimum useful values [17]. We only performed meta-analysis when ⭓3 data points existed for a test in a given epidemiologic setting. Using the MetaTest software program [18], we grouped studies for analysis depending on whether they were conducted in a developed or a resource-poor country, and all summary analyses were confined to one or the other classification. The SROC method was our primary analytic tool. We calculated AUC/SROCs according to Moses’ method, by extrapolating curves to the corners of the SROC [19]. As with LRs, there is no absolute AUC/ SROC threshold that defines a “good” test. However, an AUC/ SROC of 1.0 defines a “perfect” test, and an AUC/SROC of 0.5 defines a “useless” test [20]. To reduce the influence of studies that reported multiple cutoff points, we plotted unweighted curves [19, 21]. Where possible, we calculated com- bined sensitivities and specificities independently, using random effects [22], on the basis of the most commonly used test thresholds, and we calculated summary LRs using these pooled sensitivities and specificities. RESULTS From 13000 screened abstracts, we identified 49 candidate studies. Of these, we excluded 27 a priori, including 11 [23–33] from the earlier meta-analysis [6]. Reasons for exclusion were as follows: 11 studies tested assays against single pathogens [7, 23, 29–31, 34–39], 11 did not include Campylobacter cultures [24–28, 33, 40–44], and 5 were abstracts or letters to the editor [32, 45–48]. Of the remaining 22 studies, 8 violated validity criteria, including 4 [4, 49–51] from the 1996 meta-analysis [52]: sensitivities and specificities could not be obtained from 5 [4, 50, 53–55], 5 lacked a case definition [51, 53–56], 3 included cases and controls from separate populations [4, 49, 53], 2 analyzed experimentally induced diarrhea [4, 49], and 1 was a retrospective analysis [51] (several studies violated multiple criteria). The remaining 14 studies [52, 57–69] included 1 article that contained 2 distinct data sets, on pediatric and adult cohorts, collected in different years [65]. We analyzed both cohorts separately, bringing the total to 15 studies and 7161 patients (table 1). Lactoferrin assay. In the only study that focused on a developed country and included lactoferrin assays [62], lactoferrin assays provided useful diagnostic information, particularly when the results were negative (table 2). In studies that focused on resource-poor countries, LR+ values were all !2.0 at the +/1:50 dilution threshold. At the +++/1:50 dilution threshold, the LR+ of 11.32 from the study by Ruiz-Pelaez and Mattar [69] was the highest LR obtained for studies in either epidemiologic setting, although the 95% CIs were wide and the sensitivity was low (7%). SROC analysis could not be performed, because only a single study that focused on a developed country included lactoferrin assays. In resource-poor countries, the overall AUC/SROC for lactoferrin was 0.79 (figure 1), compared with 0.51 at the common +/1:50 threshold (curve not shown). At the common +/1:50 threshold, a positive test result provided little diagnostic information, although a negative test result substantially decreased the odds that the diagnosis would be bacterial gastroenteritis (table 3). Fecal occult blood tests. In studies that focused on developed countries, all LR+ values for occult blood tests were 12.0, and all LR⫺ values were !0.5. Conversely, in studies that focused on resource-poor countries, all LR+ values were !2.0, and all LR⫺ values were 10.5 (table 4). The combined sensitivities and specificities and the LRs were also superior in studies conducted in developed countries (table 3). Similarly, the AUC/ Stool Assays for Bacterial Gastroenteritis • CID 2003:37 (1 August) • 367 Table 1. analysis. Overview of rapid stool assays used to diagnose inflammatory bacterial gastroenteritis in studies included in a meta- Type of rapid stool assay performed Setting, reference Year Country Alvarado [59] 1983 United Kingdom Thorson et al. [60] 1985 United States DeWitt et al. [70] 1985 Loosli et al. [57] 1985 Age range FLT OBT Lacto FEM All ages MB — — — All ages MB — — — United States !4 years MB — — — Switzerland 115 years NAa HEMO — — ⭓18 years Developed countries Siegel et al. [58] 1987 United States GS HEMO — — Silletti et al. [62] 1996 United States NS MB SER LEUK — Savola et al. [63] 2001 United States NS MB — — — 1983 Bangladesh SWM — — SWM Resource-poor countries Stoll et al. [66] 50% of subjects were ⭐3 years old; 70% were ⭐14 years old Ascher and Edusada-Corpus [67] 1991 Philippines ⭐6 years MB — — — Huicho et al. [52] 1993 Peru ⭐2 years MB HEMO — — Scerpella [64] 1994 Mexico “Adults attending summer school” TS HEMO LEUK — McNeely et al. [65] 1996 Mexico “Adult college students” MB HEMO — — 3 months–7 years TS HEMO — — Huicho et al. [68] 1997 Peru ⭐2 years MB HEMAS LEUK — Ruiz-Pelaez and Mattar [69] 1999 Colombia 6 months–13 years MB NS LEUK — NOTE. FEM, fecal erythrocyte microscopy; FLT, fecal leukocyte test; GS, Gram stain; HEMAS, Hemascreen (Alpha Laboratories); HEMO, Hemoccult (Smith Kline Diagnostics); Lacto, lactoferrin assay; LEUK, Leukotest (Techlabs); MB, methylene blue; NA, not applicable; NS, not stated; OBT, occult blood test; SER, Seracult (Propper Manufacturing); SWM, saline wet mount; TS, trichrome stain. a No threshold was defined for the FLT, and therefore we only analyzed OBT data from that study. SROC for occult blood tests in studies from developed countries greatly exceeded that in studies from resource-poor countries (figure 2). Microscopy for fecal leukocytes. In developed countries, there was substantial heterogeneity in the distribution of sensitivities and specificities of microscopy for fecal leukocytes (table 5). No consistent trend emerged that related the test threshold (cells/HPF) to any of the diagnostic parameters. However, the diagnostic accuracy of microscopy for fecal leukocytes tended to be higher in studies from developed countries than in studies from resource-poor countries. In the study conducted in Bangladesh [66], the LR+ and LR⫺ at the 11-cell/HPF cutoff point were 1.0 and 1.0, respectively, which means that the test provided literally no diagnostic information at this threshold. Of 3558 patients in that study, at least 1 leukocyte/HPF was found in samples from 3487 (98%), which shows that intestinal inflammation may be ubiquitous in some cohorts and some epidemiologic settings. The study by Ascher and Edusada-Corpus [67] generated an LR+ of 26.0, almost 8-fold higher than the next highest LR+. It may be relevant that this study also had the lowest culture- 368 • CID 2003:37 (1 August) • Gill et al. positivity rate of studies from resource-poor countries, a feature that lowers the potential for false-negative results and thus increases the test’s specificity and LR+. In addition, the study population may not have been truly representative of resourcepoor countries, because it consisted of children of US military personnel stationed at a US base in the Philippines. As can be seen in figure 3, the AUC/SROCs for studies from developed countries greatly exceeded those for studies from resource-poor countries (0.89 vs. 0.72). This trend persisted at the most common threshold of 15 cells/HPF (AUC/SROC, 0.85 and 0.78, respectively). Pooled sensitivities and specificities were also higher in studies from developed countries than in studies from resource-poor countries (table 3). Notably, the largest study—and the one that found the lowest diagnostic power for microscopy for fecal leukocytes—did not test at the 15-cell/ HPF threshold, and thus it is not included in this calculation, which will be biased upward as a result [66]. The Bangladesh study of 3558 mostly pediatric patients accounted for 62% of all patients from studies from resourcepoor countries and 50% of patients from studies in both epidemiologic settings combined [66]. Exclusion of the Bangladesh Table 2. Evaluation of the lactoferrin test for diagnosis of inflammatory bacterial gastroenteritis. Setting, reference Cohort size Proportion of subjects with positive a cultures, % 416 3 121 92 Lactoferrin test Threshold, agglutination/ dilution Sensitivity (95% CI) Specificity (95% CI) LR+ (95% CI) LR⫺ (95% CI) +/1:50 0.92 (0.67–0.99) 0.79 (0.74–0.82) 4.33 (3.41–5.48) 0.10 (0.08–0.11) 24 +/1:50 0.97 (0.83–0.99) 0.15 (0.09–0.24) 1.14 (1.02–1.27) 0.23 (0.14–0.37) 59 +/1:50 0.63 (0.50–0.75) 0.47 (0.32–0.63) 1.20 (0.86–1.66) 0.78 (0.55–1.12) +/1:200 0.41 (0.29–0.54) 0.79 (0.64–0.89) 1.94 (1.03–3.63) 0.75 (0.61–0.93) Developed countries Silletti et al. [62] Total no. of subjects for this category 416 Resource-poor countries Huicho et al. [68] Scerpella et al. [64] Ruiz-Pelaez and Mattar [69] Total no. of subjects for this category NOTE. a b b 453 24 +/1:50 1.00 (0.97–1.00) 0.31 (0.26–0.36) 1.45 (1.35–1.55) 0.00 (0.00–0.00) ++/1:50 0.43 (0.34–0.52) 0.89 (0.85–0.92) 3.91 (2.86–5.36) 0.64 (0.58–0.71) +++/1:50 0.07 (0.03–0.13) 0.99 (0.98–1.00) 11.32 (2.84–45.11) 0.94 (0.90–0.99) 666 LR+, positive likelihood ratio; LR⫺, negative likelihood ratio. +, ++, and +++ indicate degree of agglutination. No. of subjects with a bacteria-positive stool culture/total no. of participants in that study. Subjects from this study were only counted once in calculating the total no. of subjects in the category. study yielded a new AUC/SROC for studies from resourcepoor countries of 0.80, dominated by the 5 data points from the study by Ruiz-Pelaez and Mattar [69]. The AUC/SROC for that study alone was 0.81, compared with 0.62 for the study by Stoll et al. [66] alone (curves not shown). Microscopy for fecal erythrocytes. All data on fecal erythrocytes came from a single study conducted in Bangladesh [66]. As shown in table 6, the diagnostic accuracy of microscopy for fecal erythrocytes was poor at all thresholds; summary sensitivity and specificity analyses could not be performed. The AUC/SROC was 0.61, which suggests that this is a poor test for identifying bacterial gastroenteritis (data not shown). Effect of reclassifying ETEC as “disease negative.” Five studies, with a total of 4257 patients, all from resource-poor countries, included patients infected with ETEC. All 5 studies tested microscopy for fecal leukocytes, 4 included occult blood tests, 1 included the lactoferrin assay, and 1 included microscopy for fecal erythrocytes. Reclassifying ETEC as “disease negative” did not have a consistent effect on the magnitude or direction of the recalculated LR+ or LR⫺ values (LR+ values increased in 3 studies and decreased in 2; LR⫺ values decreased in 3 studies and increased in 2). Most of these changes were !1.0 and thus of minimal clinical relevance. The largest changes were seen in the adult cohort of the studies by McNeely et al. [65], in which the LR+ for occult blood tests increased by 1.22, and the LR+ for microscopy for fecal leukocytes at a threshold of 15 cells/HPF increased by 1.69; by Stoll et al. [66], in which the LR+ for microscopy for fecal leukocytes at a threshold of 150 cells/HPF increased by 1.39, and the LR+ for microscopy for fecal erythrocytes at a threshold of 150 cells/HPF increased by 2.12; and by Scerpella et al. [64], in which the LR+ for microscopy for fecal leukocytes at a threshold of 11 cell/HPF decreased by 1.23. Changes in LR⫺ were !0.2 in all cases. DISCUSSION This meta-analysis demonstrates that, in developed countries, tests for fecal leukocytes, lactoferrin, and occult blood are helpful for identifying patients who are more likely to have bacterial gastroenteritis and who might, theoretically, benefit from empirical antibiotic therapy. By contrast, rapid stool assays were far less powerful when performed in resource-poor countries. Overall, microscopy for fecal leukocytes and lactoferrin tests were superior to occult blood tests and examination for fecal erythrocytes. In resource-poor countries, occult blood tests and examination for fecal erythrocytes were essentially worthless, although data on the latter came from a single study and may not be representative of resource-poor countries in general [66]. In contrast with the findings of an earlier meta-analysis [6], we were unable to conclude that the lactoferrin assay was clearly superior to examination for fecal leukocytes. However, from a practical standpoint, the relative speed and simplicity of the lactoferrin test, compared with stool microscopy, may be the deciding factor in choosing which test to adopt. This point also pertains to the use of occult blood tests in developed countries: we believe that the convenience and low cost of this test compellingly support its continued use, even though it is less powerful than either the lactoferrin test or microscopy for fecal leukocytes. Conversely, the ability to vary thresholds represents a significant advantage associated with use of the lactoferrin Stool Assays for Bacterial Gastroenteritis • CID 2003:37 (1 August) • 369 Figure 1. Summary receiver operating characteristic (SROC) curve for use of the fecal lactoferrin assay to diagnose bacterial gastroenteritis in resource-poor countries. The area under the curve is 0.79. Only a single study that focused on a developed country included lactoferrin assays, and this was insufficient for plotting an SROC curve. Reference nos. are shown in brackets, and the test threshold, expressed as agglutination (rated “+,” “++,” or “+++”)/dilution, is shown to the right. The width of the oval is proportional to the square root of the no. of persons without disease in the cohort; the height of the oval is proportional to the square root of the no. of persons with disease in the cohort. test or examination for fecal leukocytes, compared with occult blood tests, because test thresholds can be adjusted to better optimize performance on the basis of the local epidemiology of acute diarrheal disease. Table 3. There are several possible explanations for the superiority of the performance of rapid stool assays in developed countries over that in resource-poor countries. One is that technological factors reduce the diagnostic accuracy of the reference standard in resource-poor settings. The resulting misclassification due to false-negative stool culture results would likely bias any assessment of these tests’ accuracy towards the null. Spectrum bias provides another possible explanation. Spectrum bias refers to the ways in which the accuracy of a diagnostic test varies depending on such factors as who performs the test, where and how the study was conducted, the characteristics of the study population, disease severity, and the varying prevalence and virulence of diarrheagenic pathogens in different regions of the world [71]. Any or all of these factors may make it difficult to infer cause and effect when evaluating a test. For example, if a previously healthy child in a developed country presents with gastroenteritis and has detectable fecal leukocytes and a stool culture positive for Salmonella enterica, it is reasonable to assume that the 2 findings are linked. Ascribing this causal relationship is more difficult in settings where diarrheal illness is frequent and the causes diverse and multifactorial. Was the assay result positive because of the Shigella species found in the child’s stool culture that day? Or was it the result of the child’s preexisting vitamin A deficiency [72], protein deficiency enteropathy [73], or the Blastocystis hominis, hookworm, or Strongyloides stercoralis colonizing the child’s intestines? In situations in which cause and effect are blurred, rapid stool assays are probably too nonspecific to provide much clinically useful information. It is sadly ironic that these assays are least useful in settings where the incidence of and morbidity from diarrhea is greatest and where a rapid, inexpensive diagnostic test would, presumably, be most valuable. Even though the stool assays performed better in studies Pooled analyses of selected rapid stool assays, by epidemiologic setting. Setting, test No. of studies Test threshold Sensitivity a (95% CI) Specificity a (95% CI) LR+ b LR⫺ b Developed countries Fecal occult blood test 3 Any color change 0.71 (0.36–0.91) 0.79 (0.40–0.96) 3.38 0.37 Microscopy for fecal leukocytes 6 15 cells/HPF 0.73 (0.33–0.94) 0.84 (0.50–0.96) 4.56 0.32 Lactoferrin test 3 +/1:50c 0.95 (0.48–1.00) 0.29 (0.17–0.46) 1.34 0.17 Fecal occult blood test 6 Any color change 0.44 (0.32–0.57) 0.72 (0.60–0.82) 1.57 0.78 Microscopy for fecal leukocytes 8 15 cells/HPF 0.50 (0.33–0.67) 0.83 (0.74–0.89) 2.94 0.60 Resource-poor countries d NOTE. Pooled analysis was conducted when ⭓3 studies were present at a given threshold. HPF, high-power field; LR+, positive likelihood ratio; LR⫺, negative likelihood ratio. +, ++, and +++ indicate degree of agglutination. a Pooled sensitivity and specificity were calculated independently using a random-effects model. 95% CIs were not calculated for pooled LRs. Agglutination/dilution. d This summary LR⫺ is unrealistically low; its calculation included a study that reported a sensitivity of 100% [69], and, thus, an LR⫺ of 0.00. b c 370 • CID 2003:37 (1 August) • Gill et al. Table 4. Evaluation of fecal occult blood tests for diagnosis of inflammatory bacterial gastroenteritis. Cohort size, no. of subjects Proportion of subjects with positive a cultures, % Loosli et al. [57] 111 32 Siegel et al. [58] 113 42 Silletti et al. [62] 416 3 Setting, reference Fecal occult blood test Threshold (test) Sensitivity (95% CI) Specificity (95% CI) LR+ (95% CI) LR⫺ (95% CI) + (Hemoccult) 0.80 (0.64–0.90) 0.63 (0.52–0.73) 2.17 (1.57–3.00) 0.32 (0.25–0.39) + (Hemoccult) 0.87 (0.75–0.94) 0.58 (0.46–0.69) 2.07 (1.53–2.80) 0.22 (0.18–0.28) + (Seracult) 0.31 (0.13–0.58) 0.96 (0.94–0.98) 7.75 (4.51–13.32) 0.72 (0.56–0.93) Developed countries Total no. of subjects for this category 640 Resource-poor countries 92 59 + (Hemoccult) 0.33 (0.22–0.47) 0.82 (0.7–0.91) 1.81 (0.92–3.57) 0.82 (0.67–0.99) Huicho et al. [52] Scerpella et al. [64] 280 40 + (Hemoccult) 0.39 (0.31–0.49) 0.64 (0.56–0.71) 1.08 (0.87–1.35) 0.95 (0.82–1.10) Huicho et al. [68] 121 24 + (Hemascreen) 0.79 (0.62–0.90) 0.50 (0.40–0.60) 1.59 (1.23–2.04) 0.41 (0.32–0.53) McNeely et al. [65] Adult cohort 887 48 + (Hemoccult) 0.26 (0.22–0.31) 0.85 (0.82–0.88) 1.79 (1.43–2.24) 0.86 (0.82–0.91) Pediatric cohort 140 26 + (Hemoccult) 0.59 (0.43–0.74) 0.65 (0.55–0.74) 1.70 (1.25–2.31) 0.62 (0.50–0.77) 453 24 0.39 (0.31–0.49) 0.79 (0.74–0.83) 1.86 (1.49–2.33) 0.77 (0.69–0.86) Ruiz-Pelaez and Mattar [69] Total no. of subjects for this category NOTE. a NS 1973 LR+, positive likelihood ratio; LR⫺, negative likelihood ratio; NS, not stated. No. of subjects with a bacteria-positive stool culture/total no. of participants in that study. from developed countries, none of these tests were particularly powerful. Most LR+ values were 3–8, and most LR⫺ values were 0.5–0.1. For comparison, an earlier—and now obsolete—HIV antibody test had an LR+ of 327 and an LR⫺ of 0.014 [74]. Rapid stool assays will be most useful for clinical decision-making when the cause of the diarrhea is truly ambiguous (i.e., in situations in which the pretest probability of bacterial gastroenteritis approaches 50%, or 1:1 odds). In this situation, a 3–8-fold increase or decrease in the odds of disease usefully informs the decision to administer or withhold em- Figure 2. Summary receiver operating characteristic curve for use of fecal occult blood test to diagnose bacterial gastroenteritis in developed countries (A; area under the curve [AUC], 0.81) and resource-poor countries (B; AUC, 0.63). Reference nos. are shown in brackets. The width of the oval is proportional to the square root of the no. of persons without disease in the cohort; the height of the oval is proportional to the square root of the no. of persons with disease in the cohort. Stool Assays for Bacterial Gastroenteritis • CID 2003:37 (1 August) • 371 156 223 55 Siegel et al. [58] DeWitt [70] Savola et al. [63] Thorson et al. [60] b b 121 180 Huicho et al. [68] Ascher and Edusada-Corpus [67] b a 0.20 (0.13–0.28) 0.03 (0.01–0.08) 120 150 15 15 15 15 0.83 (0.64–0.93) 0.69 (0.51–0.83) 0.29 (0.22–0.38) 0.35 (0.22–0.51) 0.28 (0.24–0.32) 0.47 (0.38–0.56) 110 15 0.63 (0.53–0.71) 0.17 (0.15–0.20) 150 0.92 (0.85–0.96) 0.38 (0.35–0.41) 120 15 0.60 (0.57–0.63) ⭓1 0.98 (0.97–0.99) ⭓1 0.50 (0.37–0.63) 0.87 (0.71–0.95) 0.35 (0.19–0.55) 0.85 (0.68–0.94) 1.00 (0.93–1.00) 0.80 (0.74–0.86) 0.31 (0.13–0.58) 0.97 (0.93–0.99) 0.60 (0.50–0.69) 0.84 (0.78–0.89) 0.75 (0.66–0.82) 0.85 (0.82–0.88) 0.98 (0.96–0.99) 0.97 (0.95–0.98) 0.91 (0.88–0.94) 0.84 (0.80–0.88) 0.43 (0.38–0.48) 0.95 (0.94–0.96) 0.79 (0.77–0.80) 0.54 (0.52–0.56) 0.02 (0.02–0.03) 0.89 (0.76–0.96) 0.46 (0.28–0.65) 0.96 (0.92–0.98) 0.88 (0.81–0.92) 0.68 (0.56–0.78) 0.84 (0.78–0.88) 0.94 (0.91–0.96) 26.0 (10.84–62.38) 1.71 (1.27–2.32) 1.83 (1.28–2.62) 1.39 (0.97–2.01) 1.86 (1.49–2.33) 1.39 (0.67–2.89) 6.79 (3.67–12.57) 5.22 (3.68–7.39) 3.94 (3.04–5.10) 1.61 (1.45–1.79) 3.40 (2.88–4.01) 1.81 (1.67–1.96) 1.30 (1.24–1.37) 1.00 (0.99–1.01) 4.75 (1.86–12.12) 1.61 (1.09–2.37) 7.73 (3.97–15.07) 6.87 (4.26–11.07) 3.13 (2.19–4.45) 4.89 (3.59–6.66) 5.17 (3.25–8.20) LR+ (95% CI) Microscopy for fecal leukocytes Sensitivity (95% CI) Specificity (95% CI) 110 ⭓1 15 15 15 13 12 ⭓1 Threshold, cells/HPF HPF, high-power field; LR+, positive likelihood ratio; LR⫺, negative likelihood ratio. 13 24 40 26 48 24 23 59 56 10 17 42 43 3 Proportion of subjects with positive cultures, %a No. of subjects with a bacteria-positive stool culture/total no. of participants in that study. Subjects from this study were only counted once in calculating the total no. of subjects in the category. NOTE. 5711 280 Huicho et al. [52] Total no. of subjects for this category 887 140 Pediatric cohort 453 3558 92 Adult cohort McNeely et al. [65] Ruiz-Pelaez and Mattar [69] Stoll et al. [66] Scerpella [64] Resource-poor countries 1339 113 Alvarado [59] Total no. of subjects for this category 416 376 Silletti et al. [62] Developed countries Cohort size, no. of subjects Evaluation of microscopy for fecal leukocytes for diagnosis of inflammatory bacterial gastroenteritis. Setting, reference Table 5. 0.17 (0.15–0.20) 0.52 (0.41–0.66) 0.84 (0.75–0.94) 0.87 (0.72–1.05) 0.85 (0.80–0.90) 0.99 (0.96–1.03) 0.83 (0.77–0.89) 0.59 (0.53–0.65) 0.44 (0.40–0.49) 0.20 (0.17–0.22) 0.87 (0.85–0.90) 0.78 (0.6–0.82) 0.74 (0.71–0.78) 1.00 (0.77–1.30) 0.56 (0.47–0.66) 0.28 (0.18–0.44) 0.68 (0.56–0.83) 0.17 (0.15–0.20) 0.00 (0.00–0.00) 0.23 (0.22–0.26) 0.74 (0.57–0.95) LR⫺ (95% CI) Figure 3. Summary receiver operating characteristic curve for use of microscopic examination for fecal leukocytes to diagnose bacterial gastroenteritis in developed countries (A; area under the curve [AUC], 0.89) and resource-poor countries (B; AUC, 0.72). Reference nos. are shown in brackets, and the test threshold, in leukocytes per high-power field (HPF), is shown to the right. The width of the oval is proportional to the square root of the no. of persons without disease in the cohort; the height of the oval is proportional to the square root of the no. of persons with disease in the cohort. pirical antibiotic therapy. Merely interpreting positive results of an assay as synonymous with bacterial gastroenteritis without first considering the pretest odds of disease is overly simplistic and likely to result in clinical errors. A meta-analysis can only provide useful insights if the studies it contains are valid and representative of the diseases and patients involved. Although we pursued a conservative approach to selecting studies for analysis, the possibility remains that our selection process resulted in a biased summary estimate. Publication bias is a prevailing threat to the validity of any meta-analysis and results when studies reporting a positive result are more likely to enter the literature than are those that find a negative result. Some authorities recommend the use of funnel plots to detect publication bias, theorizing that large studies with negative results are more likely to be published than are small ones [75]; however, the validity of this approach remains controversial [76]. We note, however, that the study with the largest sample size [66] also documented the weakest performance for rapid stool assays. If publication bias contributed to this discrepancy, then the already unimpressive performance of these tests in resource-poor countries probably overestimates their actual value. Our meta-analysis identified several areas requiring further research. First, evidence about the lactoferrin assay’s accuracy in the developed world derived from a single trial [62]. Although the assay performed well in this instance, it may be presumptuous to assume that this finding is typical and generalizable to other populations in developed countries. Studies evaluating the lactoferrin test for children living in developed countries are conspicuously absent. This is unfortunate, because children are particularly susceptible to diarrheal disease and its complications and because age also contributes to spectrum bias. Second, the optimum thresholds for the lactoferrin and fecal Table 6. Evaluation of microscopy for fecal erythrocytes for diagnosis of inflammatory bacterial gastroenteritis in 3558 subjects in Bangladesh. Threshold, cells/HPF Sensitivity (95% CI) Specificity (95% CI) LR+ (95% CI) LR⫺ (95% CI) ⭓1 0.53 (0.50–0.56) 0.64 (0.62–0.66) 1.47 (1.39–1.56) 0.73 (0.70–0.77) 110 0.22 (0.19–0.25) 0.91 (0.90–0.92) 2.44 (2.16–2.76) 0.86 (0.83–0.88) 150 0.06 (0.05–0.08) 0.98 (0.97–0.98) 3.00 (2.31–3.90) 0.96 (0.94–0.98) NOTE. Culture results were positive for 23% of subjects. HPF, high-power field; LR+, positive likelihood ratio; LR⫺, negative likelihood ratio. Data are from Stoll et al. [66]. a No. of subjects with a bacteria-positive stool culture/total no. of participants in that study. Stool Assays for Bacterial Gastroenteritis • CID 2003:37 (1 August) • 373 leukocyte tests in each epidemiologic setting could not be defined given available data. It quite possible that a uniform threshold is inappropriate. In areas where diarrheal disease is hyperendemic and where the background “noise” of weakly positive test results is high, our analysis indicates that higher thresholds are probably necessary. To define optimum thresholds, future studies should routinely evaluate multiple cutoff points, and thresholds should be optimized to suit the local epidemiology. Third, we cannot be certain that the resource-poor nations in this analysis are truly representative of resource-poor countries from other parts of the world, notably sub-Saharan Africa. Similarly, our search yielded no appropriate studies of rapid stool assays in areas that are not easily classified as either “developed” or “resource poor,” such as China, former Soviet Union nations, and the Middle East. Last, randomized trials found that empirical treatment with fluoroquinolones reduces the duration of diarrheal symptoms by ∼1–2 days [77–79]. It would be extremely helpful to know whether this modest benefit would improve if a rapid stool assay were used to identify which patients should receive antibiotics. 19. Acknowledgments 20. We thank Michael Callahan, Donald Thea, Sydney Rosen, and William MacLeod (Center for International Health and Development, Boston University School of Public Health, Boston), for offering their advice during the preparation of this manuscript. 21. 10. 11. 12. 13. 14. 15. 16. 17. 18. 22. 23. 24. References 1. Mead PS, Slutsker L, Dietz V, et al. Food-related illness and death in the United States. Emerg Infect Dis 1999; 5:607–25. 2. Bern C, Martines J, de Zoysa I, Glass RI. The magnitude of the global problem of diarrhoeal disease: a ten-year update. Bull World Health Organ 1992; 70:705–14. 3. Guerrant RL, Shields DS, Thorson SM, Schorling JB, Groschel DH. Evaluation and diagnosis of acute infectious diarrhea. Am J Med 1985; 78:91–8. 4. Guerrant RL, Araujo V, Soares E, et al. Measurement of fecal lactoferrin as a marker of fecal leukocytes. J Clin Microbiol 1992; 30:1238–42. 5. Uchida K, Matsuse R, Tomita S, Sugi K, Saitoh O, Ohshiba S. Immunochemical detection of human lactoferrin in feces as a new marker for inflammatory gastrointestinal disorders and colon cancer. Clin Biochem 1994; 27:259–64. 6. Huicho L, Campos M, Rivera J, Guerrant RL. Fecal screening tests in the approach to acute infectious diarrhea: a scientific overview. Pediatr Infect Dis J 1996; 15:486–94. 7. Black RE, Levine MM, Clements ML, Hughes TP, Blaser MJ. Experimental Campylobacter jejuni infection in humans. J Infect Dis 1988; 157:472–9. 8. Tauxe RV, Pegues DA, Hargrett-Bean N. Campylobacter infections: the emerging national pattern. Am J Public Health 1987; 77:1219–21. 9. Centers for Disease Control and Prevention. Foodborne Diseases Active 374 • CID 2003:37 (1 August) • Gill et al. 25. 26. 27. 28. 29. 30. 31. 32. 33. Surveillance Network, 1996. MMWR Morb Mortal Wkly Rep 1997; 46:258–61. Blaser MJ. Epidemiologic and clinical features of Campylobacter jejuni infections. J Infect Dis 1997; 176(Suppl 2):S103–5. Centers for Disease Control and Prevention. Incidence of foodborne illnesses—FoodNet, 1997. MMWR Morb Mortal Wkly Rep 1998; 47: 782–6. Centers for Disease Control and Prevention. Incidence of foodborne illnesses: preliminary data from the Foodborne Diseases Active Surveillance Network (FoodNet)—United States, 1998. MMWR Morb Mortal Wkly Rep 1999; 48:189–94. Centers for Disease Control and Prevention. Preliminary FoodNet data on the incidence of foodborne illnesses—selected sites, United States, 1999. MMWR Morb Mortal Wkly Rep 2000; 49:201–5. Centers for Disease Control and Prevention. Preliminary FoodNet data on the incidence of foodborne illnesses—selected sites, United States, 2000. MMWR Morb Mortal Wkly Rep 2001; 50:241–6. Altekruse SF, Stern NJ, Fields PI, Swerdlow DL. Campylobacter jejuni—an emerging foodborne pathogen. Emerg Infect Dis 1999; 5: 28–35. Fleiss JL. An introduction to applied probability: statistical methods for rates and proportions. New York: John Wiley & Sons, 1981. Jaeschke R, Guyatt GH, Sackett DL. Users’ guides to the medical literature. III. How to use an article about a diagnostic test. A. Are the results of the study valid? Evidence-based Medicine Working Group. JAMA 1994; 271:703–7. Lau J. MetaTest version 0.6. Boston: Tufts–New England Medical Center, 1997. Moses LE, Shapiro D, Littenberg B. Combining independent studies of a diagnostic test into a summary ROC curve: data-analytic approaches and some additional considerations. Stat Med 1993; 12:1293–316. Walter SD. Properties of the summary receiver operating characteristic (SROC) curve for diagnostic test data. Stat Med 2002; 21:1237–56. Irwig L, Tosteson AN, Gatsonis C, et al. Guidelines for meta-analyses evaluating diagnostic tests. Ann Intern Med 1994; 120:667–76. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986; 7:177–88. Ronsmans C, Bennish ML, Wierzba T. Diagnosis and management of dysentery by community health workers. Lancet 1988; 2:552–5. Harris JC, Dupont HL, Hornick RB. Fecal leukocytes in diarrheal illness. Ann Intern Med 1972; 76:697–703. Peirce JE, DuPont HL, Lewis KR. Acute diarrhea in a residential institution for the retarded: usefulness of fecal leukocyte examination. Am J Dis Child 1974; 128:772–5. Guerrant RL, Moore RA, Kirschenfeld PM, Sande MA. Role of toxigenic and invasive bacteria in acute diarrhea of childhood. N Engl J Med 1975; 293:567–72. Pickering LK, DuPont HL, Olarte J, Conklin R, Ericsson C. Fecal leukocytes in enteric infections. Am J Clin Pathol 1977; 68:562–5. Korzeniowski OM, Barada FA, Rouse JD, Guerrant RL. Value of examination for fecal leukocytes in the early diagnosis of shigellosis. Am J Trop Med Hyg 1979; 28:1031–5. Stoll BJ, Glass RI, Huq MI, Khan MU, Banu H, Holt J. Epidemiologic and clinical features of patients infected with Shigella who attended a diarrheal disease hospital in Bangladesh. J Infect Dis 1982; 146:177–83. Speelman P, McGlaughlin R, Kabir I, Butler T. Differential clinical features and stool findings in shigellosis and amoebic dysentery. Trans R Soc Trop Med Hyg 1987; 81:549–51. Hossain MA, Albert MJ. Effect of duration of diarrhoea and predictive values of stool leucocytes and red blood cells in the isolation of different serogroups or serotypes of Shigella. Trans R Soc Trop Med Hyg 1991;85: 664–6. Paccagnini S, Fontana M, Ceriani R, et al. Occult blood and faecal leucocyte tests in acute infectious diarrhoea in children. Lancet 1987;1: 442. Jindal N, Arora R, Bhushan B, Arora S. A study of infective aetiology 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. of chronic diarrhoea in children in Amritsar. J Indian Med Assoc 1995; 93:169–70. Maki M, Maki R, Vesikari T. Faecal leucocytes in campylobacterassociated diarrhoea in infants. Acta Paediatr Scand 1979; 68:271–2. Yong WH, Mattia AR, Ferraro MJ. Comparison of fecal lactoferrin latex agglutination assay and methylene blue microscopy for detection of fecal leukocytes in Clostridium difficile–associated disease. J Clin Microbiol 1994; 32:1360–1. Iida T, Naka A, Suthienkul O, Sakaue Y, Guerrant RJ, Honda T. Measurement of fecal lactoferrin for rapid diagnosis of enterohemorrhagic Escherichia coli infection. Clin Infect Dis 1997; 25:167. Cimolai N. Fecal leukocytes in Escherichia coli O157:H7 enteritis. J Clin Pathol 1990; 43:347. Bouckenooghe AR, Dupont HL, Jiang ZD, et al. Markers of enteric inflammation in enteroaggregative Escherichia coli diarrhea in travelers. Am J Trop Med Hyg 2000; 62:711–3. Tarr PI, Neill MA, Clausen CR, Watkins SL, Christie DL, Hickman RO. Escherichia coli O157:H7 and the hemolytic uremic syndrome: importance of early cultures in establishing the etiology. J Infect Dis 1990; 162:553–6. Koplan JP, Fineberg HV, Ferraro MJ, Rosenberg ML. Value of stool cultures. Lancet 1980; 2:413–6. Nelson JD, Haltalin KC. Accuracy of diagnosis of bacterial diarrheal disease by clinical features. J Pediatr 1971; 78:519–22. Jonas A, Yahav J, Soudry A. Clinical features of viral and bacterial gastroenteritis in hospitalized children. Isr J Med Sci 1982; 18:753–9. Beltinger J, Walther R, Bardhan P, Mahalanabis D, Gyr K. Immunological testing for occult blood in patients with acute infectious diarrhea: can it improve the specificity of the guaiac test? Dig Dis Sci 1997; 42:366–71. Patwari AK, Deb M, Dudeja M, Jayasheela M, Agarwal A, Singh P. Clinical and laboratory predictors of invasive diarrhoea in children less than five years old. J Diarrhoeal Dis Res 1993; 11:211–6. Vogtlin J, Stalder H, Hurzeler L, et al. Modified guaiac test may replace search for faecal leukocytes in acute infectious diarrhea. Lancet 1983; 2:1204. Quiroga T, Garcia P, Goycoolea M, Potin M, Rodriguez L, Vial P. Fecal lactoferrin as a marker of fecal leukocytes. J Clin Microbiol 1994; 32: 2629–30. Vaishnavi C, Bhasin DK, Singh K. Fecal lactoferrin assay as a costeffective tool for intestinal inflammation. Am J Gastroenterol 2000; 95:3002–3. Guyot J, Gonvers JJ, Pyndiah N, Heitz M. Which screening test in acute diarrhea [abstract]? Gastroenterology 1985; 88:1408. Miller JR, Barrett LJ, Kotloff K, Guerrant RL. A rapid test for infectious and inflammatory enteritis. Arch Intern Med 1994; 154:2660–4. Fontana M, Zuin G, Paccagnini S, et al. Simple clinical score and laboratory-based method to predict bacterial etiology of acute diarrhea in childhood. Pediatr Infect Dis J 1987; 6:1088–91. Choi SW, Park CH, Silva TM, Zaenker EI, Guerrant RL. To culture or not to culture: fecal lactoferrin screening for inflammatory bacterial diarrhea. J Clin Microbiol 1996; 34:928–32. Huicho L, Sanchez D, Contreras M, et al. Occult blood and fecal leukocytes as screening tests in childhood infectious diarrhea: an old problem revisited. Pediatr Infect Dis J 1993; 12:474–7. Mikhail IA, Fox E, Haberberger RL Jr, Ahmed MH, Abbatte EA. Epidemiology of bacterial pathogens associated with infectious diarrhea in Djibouti. J Clin Microbiol 1990; 28:956–61. McIver CJ, Hansman G, White P, Doultree JC, Catton M, Rawlinson WD. Diagnosis of enteric pathogens in children with gastroenteritis. Pathology 2001; 33:353–8. Echeverria P, Sethabutr O, Pitarangsi C. Microbiology and diagnosis of infections with Shigella and enteroinvasive Escherichia coli. Rev Infect Dis 1991; 13(Suppl 4):S220–5. Bardhan PK, Albert MJ, Alam NH, Faruque SM, Neogi PK, Mahal- 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. anabis D. Small bowel and fecal microbiology in children suffering from persistent diarrhea in Bangladesh. J Pediatr Gastroenterol Nutr 1998; 26:9–15. Loosli J, Gyr K, Stalder H, et al. Etiology of acute infectious diarrhea in a highly industrialized area of Switzerland. Gastroenterology 1985; 88:75–9. Siegel D, Cohen PT, Neighbor M, et al. Predictive value of stool examination in acute diarrhea. Arch Pathol Lab Med 1987; 111:715–8. Alvarado T. Faecal leucocytes in patients with infectious diarrhoea. Trans R Soc Trop Med Hyg 1983; 77:316–20. Thorson SM, Lohr JA, Dudley S, Guerrant RL. Value of methylene blue examination, dark-field microscopy, and carbol-fuchsin Gram stain in the detection of Campylobacter enteritis. J Pediatr 1985; 106: 941–3. DeWitt TG. Acute diarrhea in children. Pediatr Rev 1989; 11:6–13. Silletti RP, Lee G, Ailey E. Role of stool screening tests in diagnosis of inflammatory bacterial enteritis and in selection of specimens likely to yield invasive enteric pathogens. J Clin Microbiol 1996; 34:1161–5. Savola KL, Baron EJ, Tompkins LS, Passaro DJ. Fecal leukocyte stain has diagnostic value for outpatients but not inpatients. J Clin Microbiol 2001; 39:266–9. Scerpella EG, Okhuysen PC, Mathewson JJ, et al. Evaluation of a new latex agglutination test for fecal lactoferrin in travelers’ diarrhea. J Travel Med 1994; 1:68–71. McNeely WS, Dupont HL, Mathewson JJ, Oberhelman RA, Ericsson CD. Occult blood versus fecal leukocytes in the diagnosis of bacterial diarrhea: a study of US travelers to Mexico and Mexican children. Am J Trop Med Hyg 1996; 55:430–3. Stoll BJ, Glass RI, Banu H, Huq MI, Khan MU, Ahmed M. Value of stool examination in patients with diarrhoea. Br Med J (Clin Res Ed) 1983; 286:2037–40. Ascher DP, Edusada-Corpus R. Clinical and laboratory predictors of bacterial diarrhea in a tropical environment. Mil Med 1991; 156:74–6. Huicho L, Garaycochea V, Uchima N, Zerpa R, Guerrant RL. Fecal lactoferrin, fecal leukocytes and occult blood in the diagnostic approach to childhood invasive diarrhea. Pediatr Infect Dis J 1997; 16:644–7. Ruiz-Pelaez JG, Mattar S. Accuracy of fecal lactoferrin and other stool tests for diagnosis of invasive diarrhea at a Colombian pediatric hospital. Pediatr Infect Dis J 1999; 18:342–6. DeWitt TG, Humphrey KF, McCarthy P. Clinical predictors of acute bacterial diarrhea in young children. Pediatrics 1985; 76:551–6. Boyd JC. Mathematical tools for demonstrating the clinical usefulness of biochemical markers. Scand J Clin Lab Invest Suppl 1997; 227:46–63. Bloem MW, Wedel M, Egger RJ, et al. Mild vitamin A deficiency and risk of respiratory tract diseases and diarrhea in preschool and school children in northeastern Thailand. Am J Epidemiol 1990; 131:332–9. Patwari AK. Diarrhoea and malnutrition interaction. Indian J Pediatr 1999; 66(Suppl):S124–34. Matter L, Germann D. Detection of human immunodeficiency virus (HIV) type 1 antibodies by new automated microparticle enzyme immunoassay for HIV types 1 and 2. J Clin Microbiol 1995; 33:2338–41. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315:629–34. Tang JL, Liu JL. Misleading funnel plot for detection of bias in metaanalysis. J Clin Epidemiol 2000; 53:477–84. Wistrom J, Jertborn M, Ekwall E, et al. Empiric treatment of acute diarrheal disease with norfloxacin: a randomized, placebo-controlled study. Swedish Study Group. Ann Intern Med 1992; 117:202–8. Pichler HE, Diridl G, Stickler K, Wolf D. Clinical efficacy of ciprofloxacin compared with placebo in bacterial diarrhea. Am J Med 1987; 82(Suppl 4A):329–32. Goodman LJ, Trenholme GM, Kaplan RL, et al. Empiric antimicrobial therapy of domestically acquired acute diarrhea in urban adults. Arch Intern Med 1990; 150:541–6. Stool Assays for Bacterial Gastroenteritis • CID 2003:37 (1 August) • 375