Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
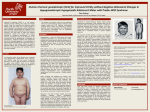
A CASE OF PRADER WILLI SYNDROME IV TH MEDICINE UNIT CHIEF DR.G.BAGIALAKSHMI M.D ASSISTANT PROFESSORS DR.N.RAGAVAN M.D DR.KRISHNASAMY PRASAD M.D PRESENTOR: DR.SREEKUMAR P.S (POST GRADUATE) • 16 yr male patient was brought to hospital with predominant complaints of INCREASED WEIGHT GAIN -10 years EXCESSIVE FOOD INTAKE - 8 years POOR SCHOLASTIC PERFORMANCE - 8 years • INCREASED WEIGHT GAIN – since childhood, associated with excess food intake • EXCESSIVE FOOD INTAKE –insidious in onset since 3 years of age gradually increasing attained the present weight H/O Poor scholastic performance + H/O day time sleepiness + H/O decreased physical activity H/O multiple meals (6-8) per day H/O developmental delay + Head Control 1 Year Of Age Standing 2 Years Walking 2 ½ Years Speech Development Delayed H/O dental caries+ • No h/o any chronic illness • No h/o constipation • No h/o head ache, visual disturbances • No h/o joint pain/ back ache • No h/o difficulty in breathing • No h/o head injury • No h/o meningitis/ encephalitis/seizures Past history • Patient had UNDESCENDED TESTIS both side for which he was operated at age of 1 ½ years of age • Evaluated for poor scholastic performance – diagnosed to have hypothyroidism at age of 11 years – started on treament T. Thyroxine 50 mic gm/day -- discontinued treatment after 3 years • Antenatal history: uneventful • Natal history:H/O BIRTH ASPHYXIA+ -no records • Post natal history: H/o feeding difficulties in infancy+ H/o poor weight gain during early infancy+ H/o floppiness during infancy+ H/o high pitched cry + H/o excessive weight gain after infancy+ Personal history Bladder bowel habits – normal • HYPERPHAGIA+ 6-8 meals /day • Excessive sleeping+ Family history Patient General examination • Conscious • Oriented • Afebrile • No pallor/icterus/cyanosis/ • No clubbing/pedal edema/lymphadenopathy. • Oral cavity: DENTAL CARIES • OBESITY: android type • No markers of congenital heart disease • No neuro cutaneous markers • Axillary & pubic hair-absent DENTAL CARIES Anthropometry Height – 150 cm Weight -84 kg BMI – 37.33 kg/m2 –OBESE Head circumference 52 cm ALMOND EYES VITAL SIGNS 110/80mm of Hg 88/min, 98%in regular Room air SYSTEMIC EXAMINATION Abdominal examination: soft no free fluid no organomegaly MICRO PENIS+ Testicular volume 2ml each Pubic hair- absent Other system examination - normal MICRO PENIS PROVISIONAL DIAGNOSIS CHILDHOOD OBESITY for evaluation ( ? Genetic /? Hormonal) Hypothyroidism INVESTIGATIONS Hb :11.1 gm% Sr. urea: 24mg% TC : 13200 cells/mm3 Sr. creatinine: 0.8mg% DC : Neutrophils-77% Urine routine Lymphocytes-10 % Albumin- Nil Monocyte -7 % Sugar- nil Platelet count- 4.76lacs/mm3 Deposits- 0-3 pus cells INVESTIGATIONS Sr calcium- 9.6 mg/dl T.CHOLESTEROL-115 RBS-118 mg/dl TRIGLYCERIDES-76 FBS- 93 mg/dl LDL-57 PPBS-129 mg/dl HDL-42 PSYCHIATRIST OPINION A c/o hypothyroidism/hypogonadotropic hypogonadism/? prader willi syndrome Advice: IQ assesment IQ TESTING done – MODERATE mental Retardation- IQ 52 OPHTHALMOLOGIST OPINION • NO squint/nystagmus • Fundus- normal • EOM – full and free OBESITY ASSOCIATED SYNDROMES WITH DEVELOPMENTAL DELAY WITHOUT DEVELOPMENTAL DELAY • • • • • • • • • • • • • • Prader-willi syndrome Fragile x syndrome Bardet biedel syndrome Wilson turner syndrome Cohen syndrome Albrights hereditary osteodystrophy • Borjesson-Forssman-Lehmann syndrome Alstrom syndrome Ulnar-mammary syndrome Simpson-golabi-mehmel syndrome Congenital leptin deficiency Leptin receptor deficiency POMC deficiency Prohormone convertase deficiency Melanocortin 4 receptor deficiency ENDOCRINOLOGIST OPINION • Obesity/hypogonadism/HYPERPHAGIA- PRESENT • Testicular volume- 2cm each • K/C/O Hypothroidism- not on regular treatment IMPRESSION: HYPOTHYROIDISM HYPOGONADOTROPIC HYPOGONADISM ? PRADER WILLI SYNDROME ADVICE: T4,TSH LH,FSH,PROLACTIN MS-PCR USG- ABDOMEN & PELVIS X RAY L HAND HORMONAL ASSAY HORMONE PATIENT VALUE REFERENCE VALUE T4 98 ng/ml 70-124 ng/ml TSH 6.2 mIU/ml 0.34-4.25 mIU/ml LH <0.07 mIU/ml 1.24-8.62 mIU/ml FSH <0.50 mIU/ml 1-12 mIU/ml Testosterone 35.93 ng/dl 270-1070 ng/dl GREEN- ELEVATED RED-REDUCED Usg abomen and scrotum: Abdomen: • no significant abnormality detected Scrotum : • Rt testis 4 ml • Lt testis 7 ml X ray L Wrist •Joint space normal •No lytic Lesions/fractures •Bone age <18 years X Ray LS Spine Indications for DNA testing in PWS Age at assessment Features sufficient to prompt DNA testing Birth to 2 yr Hypotonia with poor suck 2–6 yr • Hypotonia with a history of poor suck • Global developmental delay • Short stature and/or growth failure associated with accelerated weight gain 6–12 yr • Hypotonia with a history of poor suck (hypotonia often persists) • Global developmental delay • Excessive eating (hyperphagia,obsession with food) with central obesity if uncontrolled 13 yr through adulthood (OUR PATIENT) Cognitive impairment, usually mild mental retardation Excessive eating (hyperphagia,obsession with food) with central obesity if uncontrolled Hypothalamic hypogonadism and/or typical behavior problems(including temper tantrums and obsessive-compulsive features) Methylation specific polymerase chain reaction (MS-PCR) ENDOCRINOLOGIST REVIEW DIAGNOSIS: • Sub clinical hypothyroidism/ Prader Willi Syndrome Advice: Weight reduction Diet modification Inj Testosterone ½ c.c 15 days once T.Thyroxine 100 micro gm 1/2-0-0 T.Metformin 500 mg 1-0-1 Periodic monitoring of thyroid and glycaemic status FINAL DIAGNOSIS Genetic obesity PRADER WILLI SYNDROME Sub clinical hypothyroidism DISCUSSION What is prader willi Syndrome? • It was first described in 1956 by Andrea Prader, Heinrich Willi, Alexis Labhart, Andrew Ziegler, and Guido Fanconi of Switzerland • Incidence (USA) 1 IN 15000-20000 • Incidence (INDIA) NOT AVILABLE DEFINITION • PWS arises from the lack of expression of genes on the paternally derived chromosome 15q11-q13. • Candidate genes for PWS in this region are physiologically imprinted and silenced on the maternally inherited chromosome . • PWS develops if the paternal alleles are defective, missing, or silenced. Characteristics • Symptoms are believed to be caused by dysfunction of a portion of the brain called the hypothalamus. • Although hypothalamic dysfunction is believed to lead to the symptoms of PWS, it is unclear how the genetic abnormality causes hypothalamic dysfunction. There are two generally recognized stages of the symptoms associated with PWS • Stage 1 In the first stage, infants with PWS are hypotonic or "floppy", with very low muscle tone. Weak cry and a poor suck reflex are typical. Babies with PWS usually are unable to breastfeed and frequently require tube feeding. These infants may suffer from "failure to thrive" if feeding difficulties are not carefully monitored and treated. As these children grow older, strength and muscle tone generally improve. Motor milestones are achieved, but are usually delayed. Stage 2 An unregulated appetite characterizes the second stage of PWS. This stage most commonly begins between ages 2 and 6 years old. Individuals with PWS lack normal hunger and satiety cues. They usually are not able to control their food intake and will overeat if not closely monitored. Food seeking behaviors are very common. In addition, the metabolic rate of persons with PWS is lower than normal. Left untreated, the combination of these problems will lead to morbid obesity and its many complications. Other characteristics oPrader-Willi syndrome is considered a spectrum disorder, meaning not all symptoms will occur in everyone affected and the symptoms may range from mild to severe. oPeople with Prader-Willi often have some mental strengths as well, such as skills in jigsaw puzzles. oIf obesity is prevented, people with the syndrome can live a normal lifespan. oBehavioral problems, usually during transitions and unanticipated changes, such as stubbornness or temper tantrums oDelayed motor skills and speech due to low muscle tone oCognitive problems, ranging from near normal intelligence to mild mental retardation; learning disabilities are common oRepetitive thoughts and verbalizations oCollecting and hoarding of possessions oPicking at skin oLow sex hormone levels Indications for DNA testing Age at assessment Features sufficient to prompt DNA testing Birth to 2 yr Hypotonia with poor suck 2–6 yr • Hypotonia with a history of poor suck • Global developmental delay • Short stature and/or growth failure associated with accelerated weight gain 6–12 yr • Hypotonia with a history of poor suck (hypotonia often persists) • Global developmental delay • Excessive eating (hyperphagia,obsession with food) with central obesity if uncontrolled 13 yr through adulthood (OUR PATIENT) Cognitive impairment, usually mild mental retardation Excessive eating (hyperphagia,obsession with food) with central obesity if uncontrolled Hypothalamic hypogonadism and/or typical behavior problems(including temper tantrums and obsessive-compulsive features) • Because imprinted genes demonstrate differential DNA methylation dependent on parental origin , patients with PWS have a maternal-only imprint because they are lacking a paternal contribution. • DNA methylation analysis is the only technique, which can both confirm and reject the diagnosis of PWS, and therefore should typically be the initial investigation of Choice. • Fluorescence in situ hybridization (FISH) analysis will detect only 60% of interstitial chromosome Deletions • Negative FISH or karyotype analysis does not exclude the diagnosis and so if done first should be followed by DNA methylation analysis. Treatment In multiple studies, HUMAN GROWTH HORMONE (HGH) has been found to be beneficial in treating Prader-Willi syndrome. In June of 2000, HGH was officially recognized by the Federal Drug Administration (FDA) in the United States and other countries for use in patients with Prader-Willi syndrome. HGH is effective not only in increasing height, but also Decreasing body fat, increasing muscle mass Improving weight distribution Increasing stamina, Increasing bone mineral density Despite this, many difficult symptoms associated with PWS remain untreated. To date, no effective medications have been found to regulate appetite. Inability to control food intake is often the biggest obstacle keeping those with PWS from living independently. In addition, medical treatment of the psychiatric and behavioral issues associated with PWS has produced inconsistent results. Other Treatments Exercise and physical activity can help control weight and help with motor skills. Speech therapy may be needed to help with oral skills. REFERENCES: JOURNAL . Clin. Endocrinol. Metab. 2008 93:4183-4197 (originally published on Aug 12, 2008) Willliams text book of endocrinology Endocrinology adult and pediatric 6th edition STILL HUNGRY FOR A CURE??