Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
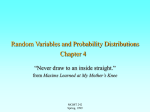
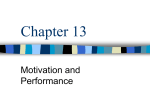
Oncogene (2004) 23, 1–8 & 2004 Nature Publishing Group All rights reserved 0950-9232/04 $25.00 www.nature.com/onc REVIEW Generating mutations but providing chemosensitivity: the role of O6-methylguanine DNA methyltransferase in human cancer Manel Esteller*,1 and James G Herman2 1 Cancer Epigenetics Laboratory, Molecular Pathology Program, Spanish National Cancer Center (CNIO), Melchor Fernandez Almagro 3, Madrid 28029, Spain; 2Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Johns Hopkins School of Medicine, Bunting-Blaustein Cancer Research Building, 1650 Orleans, Room 543, Baltimore, MD 21231, USA O6-methylguanine DNA methyltransferase (MGMT) is a key enzyme in the DNA repair network. MGMT removes mutagenic and cytotoxic adducts from O6-guanine in DNA, the preferred point of attack of many carcinogens (i.e. methylnitrosourea) and alkylating chemotherapeutic agents (i.e. BCNU, temozolamide, etc.). Hypermethylation of the CpG island located in the promoter region of MGMT is primarily responsible for the loss of MGMT function in many tumor types. The methylation-mediated silencing of MGMT has two consequences for cancer. First, tumors with MGMT methylation have a new mutator phenotype characterized by the generation of transition point mutations in genes involved in cancer etiology, such as the tumor suppressor p53 and the oncogene K-ras. Second, MGMT hypermethylation demonstrates the possibility of pharmacoepigenomics: methylated tumors are more sensitive to the killing effects of alkylating drugs used in chemotherapy. These recent results underscore the importance of MGMT in basic and translational cancer research. Oncogene (2004) 23, 1–8. doi:10.1038/sj.onc.1207316 Keywords: O6-methylguanine DNA methyltransferase; MGMT; CpG island hypermethylation; transition mutations; alkylating agents Understanding MGMT function DNA repair is an important area of research in cancer biology. Most attention has been focused on the mismatch, recombination and excision repair pathways. While these pathways are of clear importance to the development and progression of human cancer, other important mechanisms of DNA repair have not been as extensively studied. The O6-methylguanine DNA methyltransferase (MGMT) gene is one such less studied pathway affecting DNA repair capacity and involved in the biology of cancer formation and behavior. *Correspondence: M Esteller; E-mail: [email protected] or [email protected] MGMT (EC2.1.1.64, also known as O6-alkylguanine DNA alkyltransferase) is a DNA repair protein that removes mutagenic and cytotoxic adducts from O6-guanine in DNA (Pegg, 1990; Pegg et al., 1995). Alkylation of DNA at the O6 position of guanine is an important step in the formation of mutations in cancer, primarily due to the tendency of the O6-methylguanine to pair with thymine during replication, resulting in the conversion of guanine– cytosine to adenine–thymine pairs in DNA (Coulondre and Miller, 1977). Furthermore, the O6-alkylguanineDNA adduct (especially the O6-chloroethylguanine) may crosslink with the opposite cytosine residues, blocking DNA replication (Erickson et al., 1980). MGMT protects cells against these lesions, transferring the alkyl group from the O6-guanine in DNA to an active cysteine within its own sequence in a reaction that inactivates one MGMT molecule for each lesion repaired (Pegg, 1990). The alkylated MGMT protein then becomes detached from DNA and is targeted for degradation by ubiquitination (Srivenugopal et al., 1996). Thus, the ability of a cell to withstand such damage is directly related to the number of MGMT molecules that it contains and to the rate of de novo synthesis of MGMT. Although MGMT can act at different rates on a wide variety of O6-alkyl groups (and even in a minor degree over the O4-methylthymine), the majority of studies have focused on the endogenous substrate O6-methylguanine. Of the more than 12 different types of nitrogen and oxygen adducts of purine and pyrimidine bases produced by alkylating agents, O6-methylguanine is, in fact, one of the least abundant, but of most importance. O6-methylguanine affects cytosine methylation (Hepburn et al., 1991), the binding of transcription factors (Bonfanti et al., 1991), the recombinogenic capacity (White et al., 1986) and may inhibit DNA replication or cleavage if located in replication origins (Ceccotti et al., 1993) or topoisomerase-I sites (Pourquier et al., 2001). This review will focus particularly on how MGMT prevents the formation of transition mutations in DNA in human tumorigenesis and its role in modulating the sensitivity of neoplasms to the alkylating agents used in current chemotherapy. Role of MGMT in cancer M Esteller and JG Herman 2 Promoter hypermethylation of MGMT causes its loss in human cancer The amounts of MGMT protein differ according to cellular type (Gerson et al., 1986). The levels and activity of MGMT in healthy cells are regulated by its protein phosphorylation status (Srivenugopal et al., 2000), the binding of the E6 papillomavirus oncoprotein (Srivenugopal and Ali-Osman, 2002) and the action of p53 (Harris et al., 1996), glucocorticoid hormone (Biswas et al., 1999) and other transcription factors over its 50 CpG island, which includes a classical promoter without TATA and CAAT boxes and a 59 bp enhancer element located at the first exon–intron boundary (Harris et al., 1991) (Figure 1). A single report has described mutations in the MGMT gene (Wang et al., 1997). However, there are many reports of individual differences in MGMT activity in tumors. Several germline variants affecting the MGMT gene have been described (Imai et al., 1995; Rusin et al., 1999; Inoue et al., 2000; Egyhazi et al., 2002), but few studies have addressed the functional relevance of these nucleotides changes (Imai et al., 1995; Edara et al., 1996). No extensive analysis of the MGMT genotype and haplotypes distribution in healthy and cancer population exists. The MGMT protein is decreased in some tumors with respect to their normal tissue counterpart (Gerson et al., 1986, Citron et al., 1992). A subset of tumor cell lines, termed Mer, completely lack MGMT activity (Day et al., 1980). As loss of expression is not commonly due to deletion, mutation or rearrangement of the MGMT gene (Day et al., 1980, Fornace et al., 1990, Pieper et al., 1990) or mRNA instability (Kroes and Erickson, 1995), other causes for loss of activity are expected. Methylation of cytosine in CpG dinucleotides is the main epigenetic modification of DNA in normal mammalian cells (Esteller and Herman, 2002a). The human MGMT gene possesses a CpG island in the 50 portion of the gene (Harris et al., 1991). Hypermethylation of normally unmethylated CpG islands in the promoter regions of many genes, including p16INK4a, p14ARF, VHL, BRCA1, hMLH1 and E-cadherin, correlates with its loss of transcription (Esteller et al., 2001a, 2002b). Hypermethylation of the MGMT CpG island as the cause of MGMT transcriptional silencing in cell lines defective in O6-Methylguanine DNA Methyltransferase (MGMT) MGMT protein (aprox. 22 kDa) I II III IV V CpG Island: Hypermethylated in Certain Tumors Types MGMT Gene (aprox. 170 Kb) : Described Polymorphisms of Unknown Significance Figure 1 Genomic structure of the MGMT gene. Exons are indicated as gray boxes (I–V) Oncogene MGMT CpG Island Methylation Analysis NHL1 NHL2 U M U M NHL1 NHL2 Retention Loss MGMT Protein Expression Analysis MGMT mRNA (950 nucleotides) Gene Locus 10q26 O6-methylguanine repair has been demonstrated (Costello et al., 1996; Qian and Brent, 1997; Watts et al., 1997; Danam et al., 1999; Esteller et al., 1999a). As for other genes inactivated by CpG island methylation, hypermethylation of the promoter region is accompanied by histone hypoacetylation and methylation (Kondo et al., 2003), binding of specific methyl-binding proteins (Fraga et al., 2003) and loss of nucleosome positioning (Patel et al., 1997), all of these alterations rendering a ‘closed’ chromatin state that prevents gene transcription (Ballestar and Esteller, 2002). As additional proof of causality, in vitro treatment of cancer cells with demethylating drugs restores MGMT expression (Qian and Brent, 1997; Esteller et al., 2000a). To study the relevance of the promoter hypermethylation of the MGMT gene in vivo in cancer patients, we examined a large series of more than 500 primary human tumors and corresponding normal tissues for MGMT aberrant methylation using methylation-specific PCR and its relation with MGMT expression (Esteller et al., 1999a) (Figure 2). MGMT function is lost frequently in association with hypermethylation of the promoter region in a wide spectrum of human tumors (Esteller et al., 1999a). Our initial findings demonstrated a specific profile of MGMT hypermethylation in human cancer that indicated gliomas, Figure 2 MGMT promoter hypermethylation correlates with its gene silencing: an example in NHL. The CpG island methylation status of the MGMT gene was carried out by methylation-specific PCR. Briefly, DNA is modified by sodium bisulfite, which modifies the unmethylated cytosines to uracil, but it does not affect the methylated cytosines, followed by a PCR reaction using primers specific for either methylated or the modified unmethylated DNA. The presence of a visible product in lanes U indicates the presence of unmethylated genes of MGMT; the presence of a visible product in lanes M indicates the presence of methylated genes of MGMT. The analysis demonstrates that NHL1 is unmethylated and expresses MGMT determined by immunohistochemistry, while NHL2 is methylated and lacks MGMT expression Role of MGMT in cancer M Esteller and JG Herman 3 lymphomas, colon, head and neck and non-small-cell lung carcinomas as the main tumor targets for the epigenetic inactivation of MGMT (Esteller et al., 1999a). This profile, thanks to the popularization of bisulfite-PCR techniques (Fraga and Esteller, 2002), has been expanded in additional reports of MGMT inactivation in other tumor types (Toyooka et al., 2001; Virmani et al., 2001; Choy et al., 2002; Lee et al., 2002; Maruyama et al., 2002; Smith-Sorensen et al., 2002), summarized in Figure 3. This aberrant MGMT methylation has been correlated with the loss of MGMT protein (Esteller et al., 1999a, 2002c; Herfarth et al., 1999.), lack of mRNA expression (Esteller et al., 2000a; Yin et al., 2003) and loss of enzymatic activity (Herfarth et al., 1999). The constellation of tumor types where MGMT hypermethylation can be invoked has also been further understood with its analysis in a comprehensive panel of 70 human cancer cell lines (Paz et al., 2003). Furthermore, the CpG island hypermethylation-associated silencing of MGMT occurs very early in human tumorigenesis, such as in small colon adenomas (Esteller et al., 2000a), strongly supporting its relevant role in carcinogenesis. MGMT promoter hypermethylation has also been demonstrated in the serum DNA of lung cancer patients (Esteller et al., 1999b), and head and neck cancer patients (Sanchez-Cespedes et al., 2000) as well as other biological fluids, including sputum (Palmisano et al., 2000) and saliva (Rosas et al., 2001). Silencing of MGMT causes a new mutator pathway in human cancer The causes of mutations in oncogenes and tumor suppressor genes are multifactorial (Hussain and Harris, 1998). Exogenous and endogenous compounds are known to cause DNA damage (Hussain and Harris, 2000), including deletions, insertions and base substitutions, either transversions (change of purine to pyrimidine or vice versa) or transitions, change or purine to Pattern of Methylation-Mediated Silencing of MGMT in Human Primary Tumors 50 % 40 30 20 10 Testi cular (n=6 9 Colo n (n= 1) Retin 323) obla stom a (n= 23) Glio 3 ma ( Head n=21 and N 3) eck ( n=11 6) Cerv 5 ix (n =19) Ly m phom a (n= 61) NSC LC ( 7 n Esop hagu =83) s (n= 14) Stom ach ( 9 n=60 ) SCL C (n =43) Panc reas 11 ( n = 1 8) Mela nom Chola a (n= ngio 18) carcin oma 13 Kidn (n=79) ey( n =12 Leuk emia 15) (n=3 1) Blad der ( n=44 Men ) ingio ma ( 17 n=26 ) Brea st (n = 36) 19 Ovar y ( n=2 Endo 3) metr ium (n=1 7) Live 21 r (n= 5 9) Pros tate ( n=10 231) 0 Figure 3 Distribution of CpG island promoter hypermethylation of MGMT across human primary tumors of 23 different cell types. Y-axis, percentage of neoplasms with MGMT hypermethylation; X-axis, the tumor types studied with the total number of samples analysed between parentheses another purine or pyrimidine to another pyrimidine (Strauss, 1992). Well-known sources of the spontaneous generation of point mutations include: deamination of cytosine and 5-methylcytosine to uracil and thymine, respectively; depurination; DNA polymerase infidelity; and oxidative damage from endogenously produced free radicals (Hussain and Harris, 1998; Strauss, 1992). Abnormalities in DNA repair and replication have also long been considered as key elements in the genesis of mutations. Several mechanisms can be invoked to contribute to the infidelity of DNA synthesis, including imbalances in deoxynucleotide triphosphate pools, mutations in DNA polymerase-a and slippage of DNA polymerase at nucleotide repeats (Liu et al., 1983; Phear et al., 1987; Kunkel et al., 1993). However, the importance of each mechanism and gene(s) involved is often unknown. One such mutator pathway in human cancer has been clearly defined. Germline mutations in the two DNA mismatch repair (MMR) genes hMLH1 and hMSH2 are the genetic abnormalities responsible for the vast majority of hereditary nonpolyposis colorectal carcinoma cases (Bocker et al., 1999), where the presence of deletions and insertions in microsatellite sequences is a common hallmark. However, in the nonfamilial cases, the presence of microsatellite instability is attributable to methylation-associated silencing of hMLH1 as indicated by the extremely tight association between both phenomena (Kane et al., 1997; Esteller et al., 1998, 2000b; Herman et al., 1998; Fleisher et al., 1999), the restoration of MMR proficiency using demethylating agents (Herman et al., 1998) and the early appearance of hMLH1 hypermethylation, occurring in premalignant stages (Esteller et al., 1999c). The epigenetic silencing of hMLH1 then leads to mutations in target genes such as BAX or TGFRbII (Markowitz, 2000). Methylation-mediated silencing of MGMT causes another strong and important mutator pathway in human cancer that it is more prevalent than microsatellite instability. The persistence of O6-methylguanine adducts, resulting from alkylating agents, may cause DNA polymerase to misread the base pairing because of the altered hydrogen-bonding properties of a base that contains an additional methyl or ethyl group. Thus, O6methylguanine is read as an adenine and mispairs with thymine (Horsfall et al., 1990). Supporting these data, the most common mutations caused by alkylating agents are G : C to A : T transitions (Horsfall et al., 1990), exemplified in the frequent generation of G to A transitions in the oncogene K-ras when the carcinogen N-methylnitrosourea (that forms O6-methylguanine adducts) is used in experimentally induced tumor systems (Sukumar et al., 1983; Mitra et al., 1989). Avoidance of the mutagenic effect is directly related to the presence of a functional MGMT protein (Pegg et al., 1995). In vitro assays show that endogenous MGMT expression protects mammalian cell lines from spontaneous G : C to A : T transitions in the aprt gene (Aquilina et al., 1992). Animal models also show that transgenic mice overexpressing MGMT are protected against O6-methylguanine-DNA adducts caused by Oncogene Role of MGMT in cancer M Esteller and JG Herman 4 methylnitrosourea (Dumenco et al., 1993) and against G to A mutations in K-ras in aberrant colorectal crypt foci and lung tumors (Zaidi et al., 1995; Liu et al., 1999). This link between MGMT inactivation and K-ras transition mutations in human tumors was first observed in 2000 (Esteller et al., 2000a). Ras oncogenes acquire transforming activity following single-point mutations within their coding sequences. Mutations in naturally occurring ras oncogenes have been localized in codons 12, 13, 59 and 61. Alteration of codon 12, GGT, is the most common change. Substitution of the wild-type Glycine 12 by any other amino acid results in oncogenic activation of this molecule (Barbacid, 1987). Although ras mutation is the most common oncogenic alteration in human cancer (Barbacid, 1987; Bos, 1989), the incidence of K-ras activation varies widely among carcinomas. Kras mutation is rare in human primary breast carcinomas, but occurs in approximately half of colorectal carcinomas. This mutation distribution strongly resembles the pattern of MGMT promoter hypermethylation described (Esteller et al., 1999a): while MGMT aberrant methylation is not present in breast carcinomas where Kras mutations are extremely rare, it occurs in approximately 40% of cases of colorectal carcinomas associated with loss of MGMT expression, and is also frequent in non-small-cell lung carcinoma (Esteller et al., 1999b) where K-ras mutations are frequent. MGMT promoter hypermethylation was an early event in human colorectal tumorigenesis linked to the appearance of G to A mutations in the K-ras oncogene (Esteller et al., 2000a) (Figure 4). The association between MGMT methylation and K-ras mutations has now been reported not only in colon cancer in (Whitehall et al., 2001) but also in gastric and gall bladder cancers (Park et al., 2001; Kohya et al., 2003). How the loss of the DNA Repair Gene MGMT may lead to G to A mutations in the K-ras and p53 Genes ? NORMAL CELL CANCER CELL Unmethylated, Transcribed Methylated, Silenced MGMT Gene Wild –Type Codon Promutagenic Lesion Dietary Nitrates, Alkylating Agents ----GO6mGT----- ----GGT----MGMT Promutagenic Lesion ----GO6mGT----06mG is read as Adenine Mutant Codon ----GAT----- Figure 4 Methylation-mediated silencing of MGMT causes a mutator phenotype: a model of how the epigenetic loss of MGMT leads to the generation of transition mutations in p53 and K-ras. Left, a normal cell with a functional MGMT protein is able to repair the presence of O6-methylguanines (induced by endogenous and exogenous agents) in its DNA; right, tumors with MGMT inactivation due to promoter hypermethylation accumulate O6methylguanines that are misread as adenines, causing transition point mutations Oncogene The tumor suppressor p53 is the most commonly mutated gene in human cancer, and transition mutations constitute the most common p53 mutations (Greenblatt et al., 1994; Pfeifer, 2000). Approximately 52% of the mutational events are missense transitional changes, and, of this subset, B72% are G : C to A : T transitions (Greenblatt et al., 1994). The profile of the mutational spectrum varies according to tumor type. Lung and head and neck tumors of smokers have a higher number of transversions, whereas colorectal tumors have the highest rate of transition mutations, reaching 70% of the total number of p53 mutations (Greenblatt et al., 1994). These last mutations occur frequently in CpG dinucleotides, which are normally methylated (Pfeifer, 2000; Rideout et al., 1990; Tornaletti and Pfeifer, 1995), through increased rates of spontaneous deamination at methylcytosine, although other mechanisms are also conceivable. However, 17% of p53 mutations are transition mutations in non-CpG dinucleotides, where this causality cannot be invoked (Greenblatt et al., 1994). Thus, G : C to A : T changes in p53 in non-CpG and CpG dinucleotides could be attributable, in part, to a defect in MGMT that allows the persistence of O6methylguanine and its reading as an adenine (Figure 4). Promoter hypermethylation of MGMT was strongly linked to the presence of G : C to A : T transition mutations in p53, particularly in non-CpG dinucleotides (Esteller et al., 2001b) in colon cancer and has also been found in glioma (Nakamura et al., 2001; Yin et al., 2003), liver (Zhang et al., 2003) and non-small-cell lung carcinomas (Wolf et al., 2001). Yet to be classified is the particular source of promutagenic adducts in the O6 position of guanine not repaired by MGMT in each tumor type. For colorectal tumors, the alkylating agents causing the promutagenic lesion may be provided from dietary nitrates reduced in the proximal colon by bacteria, by nitrosation of amines and amides derived from protein catabolism (Ward et al., 1989; Bartsch et al., 1990; Rowland et al., 1991). For other cancers, these carcinogens are ever more speculative. Not all adducts are repaired with the same efficacy. O6-ethylguanine is removed faster than the O6-methylguanine, perhaps preventing ras mutations in certain tumor types more exposed to these xenobiotics (Engelberg et al., 1998). Among the glial tumors, MGMT epigenetic inactivation (Esteller et al., 1999a) and MGMT loss or reduced activity (Hongeng et al., 1997; Silber et al., 1998) are common features, and these epigenetic events associate with the presence of transition mutation in p53 (Nakamura et al., 2001; Yin et al., 2003). Yet, carcinogens exposure is not frequently associated with the development of brain tumors. Methylation-mediated silencing of MGMT marks tumors sensitive to alkylating agents Alkylating agents are among the most widely used chemotherapeutic drugs in human cancer (Colvin and Role of MGMT in cancer M Esteller and JG Herman 5 Hilton, 1981; Teicher, 1997). Several alkylation sites in DNA have been described as the targets of the action of these compounds, with the most frequent site the O6 position of guanine. This modification can produce DNA interstrand crosslinks (Teicher, 1997), and this base is the preferred point of attack in the DNA of numerous alkylating chemotherapeutic drugs, such as BCNU (1,3-bis(2-chloroethyl)-1-nitrosourea), ACNU (1-(4-amino-2-methyl-5-pyrimidinyl)methyl-3-(2-chloroethyl)-3-nitrosourea), procarbazine, streptozotocin or temozolamide. However, the toxicity of alkylating agents is reduced in the presence of MGMT by rapidly reversing the formation of adducts at the O6 position of guanine (Ludlum, 1990; Pegg et al., 1995), thereby averting the formation of lethal crosslinks. Thus, MGMT activity is a major mechanism of resistance to alkylating drugs (Ludlum, 1990; Pegg et al., 1995). In gliomas, enhanced sensitivity to the action of alkylating agents was initially suggested in the subgroup of patients with reduced MGMT activity (Silber et al., 1993, 1998; Belanich et al., 1996; Jaeckle et al., 1998; Gerson, 2002). Following the demonstration that CpG island hypermethylation of MGMT was the main cause behind its loss in gliomas (Esteller et al., 1999a), we thought that glioma tumors hypermethylated at MGMT would be more sensitive to the action of these alkylating agents, since their DNA lesions could not be repaired in the cancer cell and so this would lead to cell death. We gave proof of principle for this hypothesis and effectively MGMT promoter hypermethylation predicts a good response to chemotherapy, greater overall survival and longer time to progression in glioma patients treated with BCNU (Esteller et al., 2000c) (Figure 5). The methylation status of the MGMT promoter was more predictive of the outcome of carmustine treatment than the grade of the tumor, the Karnofsky performance status or the patient’s age (Esteller et al., 2000c). The potential of MGMT to predict the chemoresponse of human tumors to alkylating agents is not limited to BCNU-like alkylating agents, but it may extend to other drugs such as cyclophosphamide (Mattern et al., 1998; Cai et al., 1999; Friedman et al., 1999; Gamcsik et al., 1999), but not cisplatin (Mattern et al., 1998). This has been demonstrated in vivo in diffuse large-cell lymphomas treated with chemotherapeutic regimens including the alkylating agent cyclophosphamide (Esteller et al., 2002c), where MGMT hypermethylation was the strongest predictor of overall survival and time to progression, and was far superior to classical clinical factors such as the International Prognostic Index (IPI) (Esteller et al., 2002c). It is important to note that MGMT hypermethylation alone, without treatment with an alkylating agent, is not a good prognostic factor. In fact, it is a poor prognostic factor (Hayashi et al., 2002; Kohya et al., 2002; Brabender et al., 2003), probably due to the finding that patients with epigenetic silencing of MGMT accumulate more mutations (p53 and K-ras). This is an example of the difference between predictive and Figure 5 Overall survival (panel a) and time to the progression of disease (panel b) among patients with gliomas treated with carmustine, according to the methylation status of the MGMT promoter. Both overall survival and the time to the progression of disease were significantly greater in the group of patients with methylation of the MGMT promoter than in the group without methylation. The association was independent of the type of tumor, the patient’s age and the Karnofsky score for performance status prognostic markers. Prognostic markers suggest a difference in outcome that is independent of the treatment received, including the possibility of no treatment. An example of prognostic marker includes the above-mentioned IPI that summarizes variables related to tumor stage (stage itself, extranodal sites and LDH level) as well as host factors (age and performance status). Predictive markers, on the other hand, predict a response, and thereby often survival differences, related to a specific form of therapy. Thus, while both types of markers can predict differences in survival, predictive markers potentially provide information leading to treatment decisions. MGMT methylation is definitively a negative prognostic marker, but a positive predictive marker. Oncogene Role of MGMT in cancer M Esteller and JG Herman 6 ALKYLATING AGENTS (BCNU, Cyclophosphamide ) OPTION: CHEMOPROTECTION BY MGMT VECTORS ? NORMAL CELLS MGMT UNMETHYLATED TOXICITY (Bone Marrow) OPTIONS: OTHER DRUGS !!!! CANCER CELLS MGMT UNMETHYLATED CHEMORESISTANT TUMOR MGMT INHIBITORS: 06-BG RYBOZYMES RNAi CONSIDERATIONS: CANCER CELLS MGMT METHYLATED MMR DEFICIENT TUMORS ? SELECTION OF RESISTANT CHEMOSENSITIVE CELLS ? TUMOR Figure 6 How the different methylation backgrounds of MGMT affect the response to alkylating drugs and possible therapeutic strategies. Tumors unmethylated at MGMT are less sensitive to the action of alkylating drugs and the use of other types of chemotherapeutic agents and the inhibition of MGMT is recommended. Tumors methylated at MGMT respond well to the chemotherapy with alkylating agents. One requirement would be the necessity of a functional MMR pathway and one caveat would be the possible selection of resistant cellular subclones MGMT methylation, or lack of expression, may determine the best chemotherapy strategy, a practical example of pharmacogenomics, or, in this particular case ‘pharmacoepigenomics’ (Weinstein, 2000) (Figure 6). One might explore increasing the sensitivity of the ‘resistant’ tumors, those without MGMT inactivation, to alkylating agents (Middleton and Margison, 2003). The development of the MGMT inhibitor O6-benzylguanine (O6-BG) (Dolan et al., 1990; Dolan and Pegg, 1997) is being investigated for this purpose. O6-BG is an MGMT substrate that, by its binding to the protein in a ‘suicide’ reaction, inactivates MGMT. While this inhibitor has been found to enhance primarily the response to alkyl-nitrosoureas both in vitro and in vivo (Dolan et al., 1990; Dolan and Pegg, 1997), O6-BG has been shown to increase sensitivity to cyclophosphamide metabolites as well (Cai et al., 2001). Future studies should extend the use of determining MGMT methylation or gene expression as a marker of response to alkylating drugs in other tumor types: excellent candidates are non-small-cell lung cancer, head and neck tumors and colorectal carcinomas, where MGMT methylation is relatively frequent (Figure 3). In the case of colorectal carcinoma, MGMT methylation does not confer sensitivity to the killing action of alkylating agents if the tumor is also MMR deficient (Kawate et al., 1998, 2000). This phenomenon occurs in approximately 10% of colon tumors and in this case the presence of simultaneous methylation-mediated silencing of hMLH1 and MGMT confers resistance to cell death and may increase the mutation rate of that neoplasm. Future for MGMT In the last few years, biological and pathological data have, with the previous knowledge of the biochemistry of MGMT, raised awareness about the importance of this molecule and DNA repair of alkylation damage. The wide, but specific, spectrum of human primary tumors, having methylation-associated loss of MGMT has opened two important areas of research. Cancers with MGMT hypermethylation accumulate more point mutations than other tumors. This has been exemplified in the oncogene K-ras and the tumor suppressor gene p53, but may extend to a long list of genes yet to be discovered. Second, aberrant methylation of MGMT identifies tumors with higher sensitivity to alkylating agents. This assay may help us to design more targeted therapies and stimulate the research of new ways to overcome the resistance of the unmethylated tumors. Acknowledgements The research in Dr Esteller’s laboratory was sponsored by the Health Department of the Spanish Government, the I þ D þ I SAF 2001-0059, CAM08.1/0010.1/2001 Grants and the International Rett Syndrome Association. JGH is an Evelyn Grollman Glick scholar, whose research was supported by grants from the National Cancer Institute (CA84986 P50CA58184). References Aquilina G, Biondo R, Dogliotti E, Meuth M and Bignami M. (1992). Cancer Res., 52, 6471–6475. Ballestar E and Esteller M. (2002). Carcinogenesis, 23, 1103–1109. Barbacid M. (1987). Annu. Rev. Biochem., 56, 779–827. Bartsch H, Ohshima H, Shuker DE, Pignatelli B and Calmels S. (1990). Mutat. Res., 238, 255–267. Belanich M, Pastor M, Randall T, Guerra D, Kibitel J, Alas L, Li B, Citron M, Wasserman P, White A, Eyre H, Jaeckle K, Schulman S, Rector D, Prados M, Coons S, Shapiro W and Yarosh D. (1996). Cancer Res., 56, 783–788. Biswas T, Ramana CV, Srinivasan G, Boldogh I, Hazra TK, Chen Z, Tano K, Thompson EB and Mitra S. (1999). Oncogene, 18, 525–532. Oncogene Bocker T, Ruschoff J and Fishel R. (1999). Biochim. Biophys. Acta, 1423, O1–O10. Bonfanti M, Broggini M, Prontera C and D’Incalci M. (1991). Nucleic Acids Res., 19, 5739–5742. Bos JL. (1989). Cancer Res., 49, 4682–4689. Brabender J, Usadel H, Metzger R, Schneider PM, Park J, Salonga D, Tsao-Wei DD, Groshen S, Lord RV, Takebe N, Schneider S, Holscher AH, Danenberg KD and Danenberg PV. (2003). Clin. Cancer Res., 9, 223–227. Cai Y, Wu MH, Ludeman SM, Grdina DJ and Dolan ME. (1999). Cancer Res., 59, 3059–3063. Cai Y, Wu MH, Xu-Welliver M, Pegg AE, Ludeman SM and Dolan ME. (2001). Cancer Res., 60, 5464–5469. Ceccotti S, Dogliotti E, Gannon J, Karran P and Bignami M. (1993). Biochemistry, 32, 13664–13672. Role of MGMT in cancer M Esteller and JG Herman 7 Choy KW, Pang CP, To KF, Yu CB, Ng JS and Lam DS. (2002). Invest. Ophthalmol. Vis. Sci., 43, 1344–1349. Citron M, Graver M, Schoenhaus M, Chen S, Decker R, Kleynerman L, Kahn LB, White A, Fornace AJ and Yarosh D. (1992). J. Natl. Cancer Inst., 84, 337–340. Colvin M and Hilton J. (1981). Cancer Treat. Rep., 65, 89–95. Costello JF, Futscher BW, Tano K, Graunke DM and Pieper RO. (1996). Cancer Res., 271, 13916–13924. Coulondre C and Miller JH. (1977). J. Mol. Biol., 117, 577–606. Danam RP, Qian XC, Howell SR and Brent TP. (1999). Mol. Carcinogen., 24, 85–89. Day III RS, Ziolkowski CH, Scudiero DA, Meyer SA, Lubiniecki AS, Girardi AJ, Galloway SM and Bynum GD. (1980). Nature (Lond.), 288, 724–727. Dolan ME, Moschel RC and Pegg AE. (1990). Proc. Natl. Acad. Sci. USA, 87, 5368–5372. Dolan ME and Pegg AE. (1997). Clin. Cancer Res., 3, 837–847. Dumenco LL, Allay E, Norton K and Gerson SL. (1993). Science, 259, 219–222. Edara S, Kanugula S, Goodtzova K and Pegg AE. (1996). Cancer Res., 56, 5571–5575. Egyhazi S, Ma S, Smoczynski K, Hansson J, Platz A and Ringborg U. (2002). Hum. Mutat., 20, 408–409. Engelbergs J, Thomale J, Galhoff A and Rajewsky MF. (1998). Proc. Natl. Acad. Sci. USA, 95, 1635–1640. Erickson LC, Laurent G, Sharkey NA and Kohn KW. (1980). Nature (Lond.), 288, 727–729. Esteller M. (2000b). Eur J Cancer, 36, 2294–2300. Esteller M. (2002b). Oncogene, 21, 5427–5440. Esteller M, Catasus L, Matias-Guiu X, Mutter GL, Prat J, Baylin SB and Herman JG. (1999c). Am. J. Pathol., 155, 1767–1772. Esteller M, Corn PG, Baylin SB and Herman JG. (2001a). Cancer Res., 61, 3225–3229. Esteller M, Gaidano G, Goodman SN, Zagonel V, Capello D, Botto B, Rossi D, Gloghini A, Vitolo U, Carbone A, Baylin SB and Herman JG. (2002c). J. Natl. Cancer. Inst., 94, 26–32. Esteller M, Garcia-Foncillas J, Andion E, Goodman SN, Hidalgo OF, Vanaclocha V, Baylin SB and Herman JG. (2000c). N. Engl. J. Med., 343, 1350–1354. Esteller M, Hamilton SR, Burger PC and Baylin SB. (1999a). Cancer Res., 59, 793–797. Esteller M and Herman JG. (2002a). J. Pathol., 196, 1–7. Esteller M, Levine R, Baylin SB, Ellenson LH and Herman JG. (1998). Oncogene, 17, 2413–2417. Esteller M, Risques RA, Toyota M, Capella G, Moreno V, Peinado MA, Baylin SB and Herman JG. (2001b). Cancer Res., 61, 4689–4692. Esteller M, Sanchez-Cespedes M, Rosell R, Baylin SB, Sidransky D and Herman JG. (1999b). Cancer Res., 59, 67–70. Esteller M, Toyota M, Sanchez-Cespedes M, Capella G, Peinado MA, Watkins DN, Issa JP, Sidransky D, Baylin SB and Herman JG. (2000a). Cancer Res., 60, 2368–2371. Fleisher AS, Esteller M, Wang S, Tamura G, Suzuki H, Yin J, Zou TT, Abraham JM, Kong D, Smolinski KN, Shi YQ, Rhyu MG, Powell SM, James SP, Wilson KT, Herman JG and Meltzer SJ. (1999). Cancer Res., 59, 1090–1095. Fornace Jr AJ, Papathanasiou MA, Hollander MC and Yarosh DB. (1990). Cancer Res., 50, 7908–7911. Fraga MF, Ballestar E, Montoya G, Taysavang P, Wade PA and Esteller M. (2003). Nucleic Acids Res., 31, 1765–1774. Fraga MF and Esteller M. (2002). Biotechniques, 33, 632–649. Friedman HS, Pegg AE, Johnson SP, Loktionova NA, Dolan ME, Modrich P, Moschel RC, Struck R, Brent TP, Ludeman S, Bullock N, Kilborn C, Keir S, Dong Q, Bigner DD and Colvin OM. (1999). Cancer Chemother. Pharmacol., 43, 80–85. Gamcsik MP, Dolan ME, Andersson BS and Murray D. (1999). Curr. Pharmacol. Des., 5, 587–605. Gerson SL. (2002). Clinical relevance of MGMT in the treatment of cancer. J. Clin. Oncol., 20, 2388–2399. Gerson SL, Trey JE, Miller K and Berger NA. (1986). Carcinogenesis (Lond.), 7, 745–749. Greenblatt MS, Bennet WP, Hollstein M and Harris CC. (1994). Cancer Res., 54, 4855–4878. Harris LC, Potter PM, Tano K, Shiota S, Mitra S and Brent TP. (1991). Nucleic Acids Res., 19, 6163–6167. Harris LC, Remack JS, Houghton PJ and Brent TP. (1996). Cancer Res., 56, 2029–2032. Hayashi H, Yazawa T, Okudela K, Nagai J, Ito T, Kanisawa M and Kitamura H. (2002). Jpn. J. Cancer Res., 93, 184–189. Hepburn PA, Margison GP and Tisdale MJ. (1991). J. Biol. Chem., 266, 7985–7987. Herfarth KK, Brent TP, Danam RP, Remack JS, Kodner IJ, Wells Jr SA and Goodfellow P. (1999). Mol. Carcinogen., 24, 90–98. Herman JG, Umar A, Polyak K, Graff JR, Ahuja N, Issa JP, Markowitz S, Willson JK, Hamilton SR, Kinzler KW, Kane MF, Kolodner RD, Vogelstein B, Kunkel TA and Baylin SB. (1998). Proc. Natl. Acad. Sci. USA, 95, 6870–6875. Hongeng S, Brent TP, Sanford RA, Li H, Kun LE and Heideman RL. (1997). Clin. Cancer Res., 3, 2459–2563. Horsfall MJ, Gordon AJ, Burns PA, Zielenska M, van der Vliet GM and Glickman BW. (1990). Mol. Mutagen., 15, 107–122. Hussain SP and Harris CC. (1998). Recent Results Cancer Res., 154, 22–36. Hussain SP and Harris CC. (2000). Mutat. Res., 462, 311–322. Imai Y, Oda H, Nakatsuru Y and Ishikawa T. (1995). Carcinogenesis, 16, 2441–2445. Inoue R, Abe M, Nakabeppu Y, Sekiguchi M, Mori T and Suzuki T. (2000). Pharmacogenetics, 10, 59–66. Jaeckle KA, Eyre HJ, Townsend JJ, Schulman S, Knudson HM, Belanich M, Yarosh DB, Bearman SI, Giroux DJ and Schold SC. (1998). J. Clin. Oncol., 16, 3310–3315. Kane MF, Loda M, Gaida GM, Lipman J, Mishra R, Goldman H, Jessup JM and Kolodner R. (1997). Cancer Res., 57, 808–811. Kawate H, Itoh R, Sakumi K, Nakabeppu Y, Tsuzuki T, Ide F, Ishikawa T, Noda T, Nawata H and Sekiguchi M. (2000). Carcinogenesis, 21, 301–305. Kawate H, Sakumi K, Tsuzuki T, Nakatsuru Y, Ishikawa T, Takahashi S, Takano H, Noda T and Sekiguchi M. (1998). Proc. Natl. Acad. Sci. USA, 95, 5116–5120. Kohya N, Kitajima Y, Kitahara K and Miyazaki K. (2003). Int. J. Mol. Med., 11, 65–69. Kohya N, Miyazaki K, Matsukura S, Yakushiji H, Kitajima Y, Kitahara K, Fukuhara M, Nakabeppu Y and Sekiguchi M. (2002). Ann. Surg. Oncol., 9, 371–379. Kondo Y, Shen L and Issa JP. (2003). Mol. Cell. Biol., 23, 206–215. Kroes RA and Erickson LC. (1995). Carcinogenesis (Lond.), 16, 2255–2257. Kunkel TA. (1993). Nature (Lond.), 362, 709–715. Lee S, Kim WH, Jung HY, Yang MH and Kang GH. (2002). Am. J. Pathol., 161, 1015–1022. Oncogene Role of MGMT in cancer M Esteller and JG Herman 8 Liu L, Qin X and Gerson SL. (1999). Carcinogenesis, 20, 279– 284. Liu PK, Chang CC, Trosko JE, Dube DK, Martin GM and Loeb LA. (1983). Proc. Natl. Acad. Sci. USA, 80, 797–801. Ludlum DB. (1990). Mutat. Res., 233, 117–126. Markowitz S. (2000). J. Clin. Oncol., 18, 75S–80S. Maruyama R, Toyooka S, Toyooka KO, Virmani AK, Zochbauer-Muller S, Farinas AJ, Minna JD, McConnell J, Frenkel EP and Gazdar AF. (2002). Clin. Cancer Res., 8, 514–519. Mattern J, Eichhorn U, Kaina B and Volm M. (1998). Int. J. Cancer, 77, 919–922. Middleton MR and Margison GP. (2003). Lancet Oncol., 4, 37–44. Mitra G, Pauly GT, Kumar R, Pei GK, Hughes SH, Moschel RC and Barbacid M. (1989). Proc. Natl. Acad. Sci. USA, 86, 8650–8654. Nakamura M, Watanabe T, Yonekawa Y, Kleihues P and Ohgaki H. (2001). Carcinogenesis, 22, 1715–1719. Palmisano WA, Divine KK, Saccomanno G, Gilliland FD, Baylin SB, Herman JG and Belinsky SA. (2000). Cancer Res., 60, 5954–5958. Park TJ, Han SU, Cho YK, Paik WK, Kim YB and Lim IK. (2001). Cancer, 92, 2760–2768. Patel SA, Graunke DM and Pieper RO. (1997). Mol. Cell. Biol., 17, 5813–5822. Paz MF, Fraga MF, Avila S, Guo M, Pollan M, Herman JG and Esteller M. (2003). Cancer Res., 63, 1114–1121. Pegg AE. (1990). Cancer Res., 50, 6119–6129. Pegg AE, Dolan ME and Moschel RC. (1995). Prog. Nucl. Acid Res. Mol. Biol., 51, 167–223. Pfeifer G P. (2000). Mutat. Res., 450, 155–166. Phear G, Nalbantoglu J and Meuth M. (1987). Proc. Natl. Acad. Sci. USA, 84, 4450–4454. Pieper RO, Futscher BW, Dong Q, EllisTM and Erickson LC. (1990). Cancer Commun., 2, 13–20. Pourquier P, Waltman JL, Urasaki Y, Loktionova NA, Pegg AE, Nitiss JL and Pommier Y. (2001). Cancer Res., 61, 53–58. Qian XC and Brent TP. (1997). Cancer Res., 57, 3672–3677. Rideout WM, Coetzee GA, Olumi AF and Jones PA. (1990). Science (Wash., DC), 249, 1288–1290. Rosas SL, Koch W, da Costa Carvalho MG, Wu L, Califano J, Westra W, Jen J and Sidransky D. (2001). Cancer Res., 61, 939–942. Rowland IR, Granli T, Bockman OC, Key PE and Massey RC. (1991). Carcinogenesis, 12, 1395–1401. Rusin M, Samojedny A, Harris CC and Chorazy M. (1999). Hum. Mutat., 14, 269–270. Oncogene Sanchez-Cespedes M, Esteller M, Wu L, Nawroz-Danish H, Yoo GH, Koch WM, Jen J, Herman JG and Sidransky D. (2000). Cancer Res., 60, 892–895. Silber JR, Bobola MS, Ghatan S, Blank A, Kolstoe DD and Berger MS. (1998). Cancer Res., 58, 1068–1073. Silber JR, Mueller BA, Ewers TG and Berger MS. (1993). Cancer Res., 53, 3416–3420. Smith-Sorensen B, Lind GE, Skotheim RI, Fossa SD, Fodstad O, Stenwig AE, Jakobsen KS and Lothe RA. (2002). Oncogene, 21, 8878–8884. Srivenugopal KS and Ali-Osman F. (2002). Oncogene, 21, 5940–5945. Srivenugopal KS, Mullapudi SR, Shou J, Hazra Tka and AliOsman F. (2000). Cancer Res., 60, 282–287. Srivenugopal KS, Yuan XH, Friedman HS and Ali-Osman F. (1996). Biochemistry, 35, 1328–1334. Strauss BS. (1992). Cancer Res., 52, 249–253. Sukumar S, Notario V, Martin-Zanca D and Barbacid M. (1983). Nature, 306, 658–661. Teicher BA. (1997). Cancer: Principles and Practice of Oncology, DeVita VT, Hellman S and Rosenberg SA (eds). Lippincott-Raven Publishers: Philadelphia, pp. 405–418. Tornaletti S and Pfeifer GP. (1995). Oncogene, 10, 1493–1499. Toyooka S, Toyooka KO, Maruyama R, Virmani AK, Girard L, Miyajima K, Harada K, Ariyoshi Y, Takahashi T, Sugio K, Brambilla E, Gilcrease M, Minna JD and Gazdar AF. (2001). Mol. Cancer Ther., 1, 61–67. Virmani AK, Muller C, Rathi A, Zoechbauer-Mueller S, Mathis M and Gazdar AF. (2001). Clin. Cancer Res., 7, 584–589. Wang L, Zhu D, Zhang C, Mao X, Wang G, Mitra S, Li BF, Wang X and Wu M. (1997). Int. J. Cancer, 71, 719–723. Ward FW, Coates ME and Walker R. (1989). Food Chem. Toxicol., 27, 445–449. Watts GS, Pieper RO, Costello JF, Peng Y-M, Dalton WS and Futscher BW. (1997). Mol. Cell. Biol., 17, 5612–5619. Weinstein JN. (2000). N. Engl. J. Med., 343, 1408–1409. White GR, Ockey CH, Brennand J and Margison GP. (1986). Carcinogenesis, 7, 2077–2080. Whitehall VL, Walsh MD, Young J, Leggett BA and Jass JR. (2001). Cancer Res., 61, 827–830. Wolf P, Hu YC, Doffek K, Sidransky D and Ahrendt SA. (2001). Cancer Res., 61, 8113–8117. Yin D, Xie D, Hofmann WK, Zhang W, Asotra K, Wong R, Black KL and Koeffler HP. (2003). Mol. Carcinogen., 36, 23–31. Zaidi NH, Pretlow TP, O’Riordan MA, Dumenco LL, Allay E and Gerson SL. (1995). Carcinogenesis, 16, 451–456. Zhang YJ, Chen Y, Ahsan H, Lunn RM, Lee PH, Chen CJ and Santella RM. (2003). Int. J. Cancer, 103, 440–444.