Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
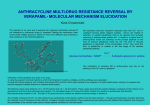
615 JACC Vol. 9,:-10 3 March 19H7:615 21 Sustained Release Verapamil, A Once Daily Preparation: Objective Evaluation Using Exercise Testing, Ambulatory Monitoring and Blood Levels in Patients With Stable Angina RAVINDER S, KOHLI, MS, MD, MNAMS, OM, ERWIN A, RODRIGUES, MS, MRCP, LIAM O. HUGHES, MS, MRCP, AVIJIT LAHIRI, MS, SS, MSc, EDWARD B, RAFTERY, SSc, MD, FACe, FRCP Harrow. Middlesex. England The efficacy of a once daily, sustained release formulation of verapamil (Verapamil SR, 360 mg) was evaluated in 19 patients with chronic angina pectoris using a double-blind placebo-controlled crossover protocol. Evaluation by exercise testing, 24 hour electrocardiographic ambulatory monitoring and blood drug level assays was performed at the end of each 2 week phase, 21 to 23 hours after the last dose. After the crossover protocol, all patients were given sustained release verapamil for 4 weeks and the evaluation was repeated. Exercise time (mean ± SEM) increased from 7.4 ± 0.6 minutes with placebo to 9.6 ± 0.8 minutes with verapamil (p < 0.001) and to 9.5 ± 0.7 minutes (p < 0.001) after 4 weeks of therapy. The mean time to I mm ST depression also increased significantly, from 4.5 ± 0.4 and 4.8 ± 0.5 minutes in bipolar leads CMs and CCs, respectively, with placebo, to 5.5 ± 0.6 (p < 0.05) and Verapamil was first introduced in 1962 as a coronary vasodilator (I) and its anti anginal effects were described by Neumann and Luisada (2) in 1966, The plasma half-life of the standard formulation is 4 hours. which necessitates administration three to four times a day, Because repeated dose regimens may compromise patient compliance, a new sustained release preparation of verapamil (Verapamil SR, 360 mg) was recently developed to maintain satisfactory blood levels of the drug over 24 hours after once daily administration. We have evaluated the efficacy of once daily therapy with this new preparation in patients with chronic stable angina pectoris. From the Department of Cardiology, Northwick Park Hospital & Chnical Research Centre, Harrow, Middlesex, England. Manuscript received November II, 1985: revised manuscript received February 19, 1986, accepted October 22, 1986. Addre" for reprint,: E.B. Raftery, MD, Department of Cardiology, Northwick Park Hospital and Clinical Research Centre, Watford Road, Harrow, Middlesex, HAl 3LJJ. England. © 1987 by the American College ot Cardiology 6.2 ± 0.5 minutes (p < 0.01) with verapamil. Maximal ST depression and rest and peak heart rates were not altered significantly. The mean rate-pressure product was 208 ± 9.9 with placebo and decreased to 189 ± 7.7 (p < 0.05) with verapamil but rose to 200.6 ± 10.4 (p = NS) after 4 weeks of therapy. The mean hourly heart rates were lower with the drug than with placebo throughout the 24 hour period but there was no significantbradycardia, arrhythmia or heart block. Episodes of ambulatory ST segment depression were also decreased by sustained release verapamil. Blood levels at 21 to 23 hours after the last dose were within the therapeutic range. The data indicate that this formulation of verapamil is effective when administered once daily. (J Am Coli Cardiol 1987;9:615-21) Methods Selection of patients. To be suitable for the trial, patients were required to have unequivocal evidence of obstructive coronary artery disease (determined by coronary arteriography), classic angina on exertion relieved by rest and sublingual administration of glyceryl trinitrate and a minimal incidence of four attacks a week. All were required to develop anginal pain on treadmill exercise testing in association with at least I mm ST segment depression with a slope less than 0.1 mV/s in bipolar lead CM s or CC s, or both. Only patients physically capable and mentally motivated for repeated treadmill exercise and Holter monitoring were entered into the trial. Patients older than 72 years and women of childbearing age were excluded. Myocardial infarction in the preceding 4 months, unstable angina and severe symptoms that were judged clinically to contraindicate placebo treatment, overt cardiac failure, rest blood pressure levels in excess of 1601\00 0735-1097/W$3.50 KOHLI ET AL. SUSTAINED RELEASE VERAPAMIL IN ANGINA 616 mm Hg and insulin-dependent diabetes mellitus were other exclusion criteria. All patients receiving diuretic drugs, digitalis and other cardiovascular drugs were excluded, as were those showing more than 0.5 mm ST segment depression on standing, hyperventilation or the Valsalva maneuver. All cardioactive medication (except sublingual nitroglycerin) was withdrawn for at least 7 days before entry into the trial. Patients then entered into a single-blind (patient blind) placebo washout period of 14 days and at the end of this period a maximal symptom-limited graded exercise test and 24 hour ambulatory monitoring were performed. Only patients fulfilling the entry criteria entered the next phase, which consisted of two double-blind crossover periods of 2 weeks each in which patients received either sustained release verapamil, 360 mg once daily, or placebo at approximately midday, crossing over to the alternative drug in the next period. After this phase all patients were given sustained release verapamil, 360 mg once daily, for 4 weeks when the evaluations were repeated. Exercise testing and 24 hour ambulatory electrocardiographic monitoring were carried out at the end of each double-blind phase and at the end of the open 4 week therapy period, the exercise test being timed for 21 to 23 hours after the last dose. Blood samples for drug level estimations were withdrawn at the end of each phase, just before exercise. The patients kept records of the number of anginal attacks, nitroglycerin consumption and side effects on diary cards throughout the trial. All patients gave written informed consent before entering the trial, which was approved by the Hospital Ethical Committee. Study patients. Nineteen patients were entered into the study. Eighteen were men and the mean age was 57.9 years (range 41 to 72). Eighteen completed the initial doubleblind crossover phase and 17 completed the final 4 week phase. Figure I. Mean ± SEM exercise time and time to I mm ST depression (in leads CM) and CC) with placebo (n), Verapamil SR (IIII) and medium-term (4 weeks) (~) therapy with Verapamil SR. * P < 0.05; *** P < 0.01; **** P < 0.001. ··• ·••• "1 10 '" <1> :; c: 'E 8 ·. •• ! c: <1> E ;.= 4 Exercise time 1 mm time CMS 1 mm time CCS JACC Vol. 9. No.3 March 1987:615-21 Table I. Measured Exercise Variables in 19 Patients I. Exercise time in minutes (to the nearest 0.1 minute) 2. Time to I mm ST depression in leads CM, and CC, 3. Maximal ST depression in leads CM, and CC, 4. Rest HR 5. Maximal (peak) HR 6. HR gain (maximal HR - rest HR) 7. HR unit gain (HR gain/exercise time) 8. Rest systolic BP 9. Maximal (peak) systolic BP 10. Rate-pressure ([maximal (peak) BP x maximal (peak)1 HRIlOO) BP = blood pressure; HR = heart rate. Exercise testing. A symptom (angina)-limited graded treadmill exercise test was performed at the end of each phase by means of a computer-assisted exercise system (CASE, Marquette Electronics) linked to a Quinton treadmill, using a standardized graded exercise protocol (3,4). Bipolar leads CM s and CCs were monitored continuously. Each exercise test was performed in the morning with patients in the fasting state, 21 to 23 hours after the last dose of medication, and carried out in a room with a controlled temperature of 20°C to 24°C (5), on the same equipment, between 9:00 and II :00 AM. The patients were requested to refrain from smoking on the morning of the test and had not taken sublingual nitroglycerin for at least 2 hours. The electrocardiogram was monitored continuously before, during and for 5 minutes after exercise and was analyzed by a microprocessor system that provided a continuous display of heart rate, ectopic beat count, J point level (to the nearest 0.1 mm) and ST slope (to the nearest 0.1 mV/s). The systolic blood pressure was measured by calibrated cuff sphygmomanometry and the data were fed into the computer every 3 minutes and at peak exercise. The digitized exercise test variables were stored on a cassette tape and later played back into a PDP 11/23 microcomputer for further data computing. The exercise variables measured are listed in Table I. Ambulatory monitoring. Ambulatory electrocardiographic monitoring was carried out for 24 hours using the same two leads (CM s and CCs ) used for exercise testing. A frequency-modulated tape recorder (Oxford Medilog II) with a quartz controlled time channel was used for this purpose. Visual analysis of the tapes was performed to identify any prolongation of the PR interval or other conduction defects. Mean hourly heart rates were obtained using a computer program (4). The tapes were played through an Oxford PB4 replay unit and displayed on a Path-Finder system (Reynolds Medical). The ST segment was also analyzed and episodes of ST segment depression of more than I mm at the J point with a planar or downsloping ST segment lasting at least I minute were identified. The lead analyzed for ST changes was CMs. Daytime and nighttime changes were KOHLI ET AL. SUSTAINED RELEASIo VERAPAMIL IN ANGINA lACC Vol 9. No. , March 19X7:615 21 studied separately. The computer program and methods of tape analysis have been described in detail elsewhere (6-8). Blood levels. Samples for drug blood levels were withdrawn by venipuncture 21 to 23 hours after the last dose of medication, before the patients were exercised. The blood samples were centrifuged, the plasma was frozen and analyses for verapamil and norverapamil levels using high performance liquid chromatography with ftuorometric detection were performed (9). Blood samples for biochemistry profiles were also obtained at the end of each phase as a safety measure. Statistics. Statistical analysis was carried out using Student's paired t test (two-tailed). A probability value of less than 0.05 was considered significant. Unless otherwise stated, mean values ± SEM are shown. Results Exercise data (Table 2). Double-blind crossover period. All 19 patients developed angina while receiving placebo. Two patients became free of angina and had to stop exercise because of fatigue while taking Verapamil SR. The mean exercise time (Fig. I) with placebo was 7.4 ± 0.6 minutes and this increased significantly (p < 0.001) to 9.6 ± 0.8 minutes with Verapamil SR. The mean time to I mm ST depression (Fig. I) in lead CMs increased from a placebo value of 4.5 ± 0.4 to 5.6 ± 0.6 minutes with the active drug (p < 0.05). Similarly, the time to I mm ST depression in lead ce , increased from 4.8 ± 0.5 minutes with placebo to 6.2 ± 0.6 minutes with verapamil (p < 0.01). Maximal ST depression in leads CMs and CCs showed no statistically significantalteration with placebo; the values 617 200 - 160 ~ 120 ~ I :F ~ 60 1 .] o Peak systolic BP Resting systolic BP Figure 2. Mean ± SEM rest and peak systolic blood pressure (BP) on exercise with placebo ([J), Verapamil SR (!III) and medium-term (4 weeks) (~) therapy with Verapamil SR. * p < 0.05; *** P < 0.01. in leads CM, and CCs were 2.0 ± 0.2 and 1.7 ± 0.2 mm with placebo and 2.1 ± 0.2 and 1.9 ± 0.2 mm with Verapamil SR (p = NS), respectively. Rest heart rate and peak exercise heart rate were 82.9 ± 3.3 and 128.2 ± 3.8 beats/min with placebo and 79.0 ± 3.3and 124.1 ± 3.9beats/min, respectively,withVerapamil SR (p = NS). Heart rate gain (maximal heart rate - rest heart rate) with placebo was 45.33 ± 2.66 beats/min and remained unchanged after verapamil (45.11 ± 2.91). Heart rate unit gain decreased significantly from 7.0 ± 0.9 beats/min with placebo to 5.3 ± 0.6 with verapamil (p < 0.0 I). The rest systolic blood pressure with placebo was Table 2. Results of Verapamil SR in Exercise Variables Placebo Exercise time (minutes) 1 mm Time CM, Verapanul SR Mean +SD .±.SEM 7.4 4.5 2.6 1.8 0.6 0.4 4.8 1.'1 2.0 1.7 82.9 128.2 45.3 7.0 140.0 163 208.4 0.8 0.9 14.2 16.2 11.I 3.9 19.1 24.2 42.3 Mean Therapy for 4 Week> Placebo Versus 4 Week Period (p Value) .:t.SD '-SEM '1.6 5.5 3.3 2.5 0.8 0.6 '1.5 5.4 2.8 2.2 0.7 0.5 <0.001 <.0.05 <.0.001 <' 0 .05 0.5 6.2 2.5 0.6 6.0 3.2 0.8 <. '(U)[ <'(LOS 0.2 0.2 3.3 3.8 2.6 0.9 4.5 5.7 9.9 2.1 1.9 7.9 124.1 45.1 5.3 130.2 1528 189.6 0.8 0.8 139 165 12.3 2.5 13.5 16.7 32.7 0.2 0.2 33 3.9 2.3 0.6 3.2 3.9 7.7 2.3 1.9 77.8 128.6 46.1 5.6 137.2 155.5 200.6 1.0 1.0 14.8 20.2 11.5 2.6 17.8 19.8 42.9 0.3 0.3 3.6 4.9 2.8 0.6 4.3 4.8 10.4 NS NS NS NS NS NS NS NS NS NS NS NS NS NS Mean '±'SD + SEM Placebo Versus Verapamil (p Value) (minutes) I rnrn Time CC, (minutes) Peak ST CM, (rnrn) Peak ST CC, (rnm) Re,t HR (beats/min) Peak HR (beats/min) HR (beats/min) gain HR unit gain Re,t BP (mm Hg) Peak BP (rnm Hg) Rate-pressure product/IOO BP = blood pressure: HR - heart rate. <.'(U) I «o.n: <.0.05 <'.0.05 KOHLI ET AL. SUSTAINED RELEASE VERAPAMIL IN ANGINA 618 lACC Vol. 9. No.3 March 1987:615-21 Figure 5. The mean hourly heart rate plots represent themaximal 250 minimal (8) and mean (C) heart rates over 24 hours, recorded by ambulatory electrocardiographic monitoring. The values for placebo (0), Verapamil SR (2 weeks (6) and 4 week (D) data are depicted. (A); :5 200 ~ <Xl .~ :s 120 150 VI >. A VI X Q> ... "Iii 100 110 t:: '" Q> :I: SO ~ ~ 100 'i: ~ x sys- Ul tolic blood pressure/ 100) on exercise with placebo (D), Verapamil SR (lIII) and medium-term (4 weeks) (~) therapy with Verapamil SR. <D Figure 3. Mean ± SEM rate-pressure product (heart rate 140 ± 4.5 mm Hg and this decreased to 130.2 ± 3.2 mm Hg with verapamil (p < 0.01) (Fig. 2). The peak systolic blood pressure decreased from a placebo value of 163.2 ± 5.7 mm Hg to 152.8 ± 3.9 with verapamil (p < 0.05). The heart rate-systolic pressure (Fig. 3) was 208.4 ± 9.9 with placebo and 189.6 ± 7.7 with verapamil (p < 0.05). Final 4 week phase. Seventeen of the 19 patients completed this phase, during which they received Verapamil SR, 360 mg once daily, at midday. The exercise time at the end of this period, 9.5 ± 0.7 minutes, was significantly greater than with placebo (p < 0.001) (Fig. I and 4). The time to 1 mm ST depression (Fig. I) in leads CM s and CC s , 5.4 ± 0.5 and 6.0 ± 0.8 minutes, respectively, was also significantly greater than with placebo (p < 0.05). There was no significant change in maximal ST depression compared with placebo. Rest heart rate, peak heart rate, heart rate gain, heart rate unit gain, and rest and peak systolic ~ 90 80 TIME OF DAY IN HOURS 85 80 75 70 65 60 12.00 20 M = 7.4 M = 9.7 M = 9.5 (4 18. 00 21:00 00. 00 03. 00 06. 00 TIME OF OAY IN HOURS Figure 4. Individual changes in exercise time are shown for each patient (n = 14) for placebo, Verapamil SR and medium-term weeks) Verapamil SR therapy. 15dlO 100 c 90 18 VI 16 Q> 80 "5 14 c E 12 E 10 '" ~ x '" ..... 6 c VI 70 8 60 4 2 o Placebo Verapamil SR 4 weeks 50 +-~--r--'--"""--'r-"'~""-~"""~~"""~""'~"-"~~ 09.00 12.00 15.00 18.00 21:00 00.00 03.00 06.00 TIME OF DAY IN HOURS KOHLI ET AL SL:STAINED RELEASE VERAPAMIL IN ANGINA JACC Vol. 9. No.3 March 1987:615 21 blood pressures were not significantly different after 4 weeks of therapy with verapamil compared with the placebo values. The rate-pressure product at the end of this phase was 200.0 ± 10.4, which was not significantly different from the placebo value (Fig. 3). There were no significant changes between exercise indexes after the double-blind phase with verapamil and those after the final 4 week open treatment period. Ambulatory monitoring. Heart rate data. The mean hourly heart rate trends are shown in Figure 5. The heart rate with Verapamil SR remained lowe! than during placebo therapy 23 hours after the last dose. The mean minimal hourly heart rate with verapamil was consistently lower than the placebo value and the effect was more profound after the 4 week period than after the double-blind phase. However, the heart rate was never low enough to produce symptoms (the lowest mean heart rate was 56 beats/min). A similar effect on the mean maximal hourly heart rate was observed, with the rate being lower with verapamil therapy. The maximal difference in heart rates between placebo and the 4 week drug period was observed at about 10:00 AM (22 hours after the last dose), the curves diverging rapidly. The smallest difference was observed 24 hours after the last dose. ST segment data (Table 3). The number of episodes of significant ST depression averaged 2.6 ± 0.8 and 1.6 ± 0.4 in lead CM s during the day and night, respectively, with placebo. The corresponding values after the double-blind Verapamil SR phase were 1.2 ± 0.5 and 1.2 ± 0.2; after the open 4 week phase they were 1.8 ± 0.4 and 1.6 ± 0.4, respectively (p = NS). The mean duration of significant ST segment depression in lead CM s with placebo was 30.0 ± 12.6 and 31.5 ± 9.5 minutes during the day and night, respectively. This decreased to 9.3 ± 3.6 and 24.3 ± 7.6 minutes, respectively, after 2 weeks of verapamil (doubleblind phase) (p = NS). The duration of ST segment depression remained less than the placebo value after 4 weeks (open phase) of verapamil, being 12.9 ± 5.3 and 29.6 ± 9.1 minutes during the day and night, respectively; this difference was not statistically significant. Blood levels. The mean verapamil levels were 159.8 ± 68.6 ng/ml after the initial 2 week (double-blind) phase and 167.1 ± 63.4 ng/ml after the 4 week therapy period. The Table 3. Ambulatory ST Segment Variables in eM, on 619 corresponding mean norverapamillevels were 198.0 ± 63.3 and 207.2 ± 75.1 ng/rnl, respectively. Anginal attacks and sublingual nitroglycerin consumption. There was a reduction in the number of anginal episodes after Verapamil SR (81 in 2 weeks) as compared with placebo (170 in 2 weeks). Similarly, the consumption of sublingual nitroglycerin decreased from 122 tablets in 2 weeks with placebo to 53 tablets in 2 weeks after Verapamil SR therapy. Side effects and withdrawals. The drug was well tolerated. Two patients developed constipation during active treatment but this was not severe enough to warrant cessation of therapy. One patient developed palpitation during both placebo and active therapy; no arrhythmia was documented. One patient was taken out of the study because of a "withdrawal effect," consisting of worsening of angina and an increase in blood pressure after crossover to the placebo phase. Another patient could not complete the last 4 week phase because of other medical problems. Discussion Neumann and Luisada (2) first reported the antianginal effects of verapamil and these were later confirmed by other studies (3,10-16). All these studies used multiple daily doses of verapamil. The aim of the present study was to evaluate objectively the sustained antianginal effects of Verapamil SR, a new long-acting formulation for once daily administration in a strength of 360 mg. In this preliminary study we endeavored to minimize observer bias by performing computerized exercise testing with the end point being controlled by the patient himself (that is, the onset of angina or fatigue). The 24 hour electrocardiographic tape recordings were carried out on the day before the exercise test in order to avoid any carryover effects. We compared the efficacy of Verapamil SR with placebo and then evaluated the medium-term effects after 4 weeks of therapy. To assess the duration of effect, the exercise tests were carried out 21 to 23 hours after the last dose, which was taken between 10:00 and 12:00 AM. Samples for drug levels were similarly taken 21 to 23 hours after the last dose, and immediately before the exercise test. Verapamil SR (± SEM) Verapamil SR Placebo ST Segment Depression No. of episodes> I mm Duration (minutes) Day 2.6.± 0.8 30.0 ± 12.6 Double-Blind Phase Night 1.6 :±- 0.4 31.5 + 9.5 Day 1.2 + 0.5 9.3 + 3.6 Note: None of the VerapamiJ SR values were statistically different from the placebo values. NIght 1.2 ::+: 0.2 24.3 T 7.6 4 Week Phase Day 1.8 + 0.4 12.9 + 5.3 Night 1.6 ± 0.4 29.6 + 9.1 620 KOHLI ET AL. SUSTAINED RELEAS E VERAPAMIL IN ANGINA Pharmacokinetics. The pharmacokinetics of verapamil have been well described (17- 20). The oral dose (20 to 100 times higher than the intravenous dose) is almost completely absorbed but undergoes extensive first pass degradation in the liver. The peak plasma level with the standard formulation of verapamil is reached between 30 and 90 minutes after administration, whereas that of the once daily longacting verapamil (Verapamil SR) is reached in approximately 7.5 hours (2 1). The therapeutic plasma concentration lies between 15 and 100 nglml. In a comparative study between a single dose of standard verapamil (Cordilox, 80 mg) and Verapamil SR (240 mg) (21) the maximal plasma concentrations of verapamil and norverapamil were 78.84 ± 44.04 and 52.74 ± 14.3 ng/ml, respectively, with the former and 83.82 ± 32.87 and 69.60 ± 14.6 ng/rnl, respectively, with the latter (21) . The lowest mean levels of verapamil and norverapamil after 7 days of Cordilox (80 mg three times daily) and verapamil SR (240 mg) once daily were 42.73 and 8 1.58 and 34.84 ng/rnl. respectively. These levels were 8 and 24 hours after the last dose of Cordilox (80 rng) and Verapamil SR (240 mg), respectively. These data and those obtained in our study indicate a bioavailability profile that is adequate for a once daily regimen. Effect in exercise tests. In this study, the mean exercise time was significantly prolonged by Verapamil SR and this increase occurred in all but three patients. In one it remained unchanged and in the other two it decreased. However, two of these three patients showed an increase in exercise time at the end of the 4 week phase (Fig. 4). There was also a significant increase in the mean time to I mm ST depression. Maximal ST depression did not show a signifi cant change. because of the increase in exercise time required to produce the same ST change, but there was a lesser degree of ST depression with verapamilthan with placebo therapy at comparable levels of exercise. The increase in exercise time after 4 weeks of open therapy with Verapamil SR was 23lJt. which contrasts with an increase of 40Ck previously reported in patients receiving the standard formulation for 4 weeks ( 14) . In assessing this observation, it has to be borne in mind that these were different groups of patients. Effect on Holter recordings. The 24 hour ambulatory heart rate data showed the sustained effects of Verapamil SR on heart rate, particularly in the 6 hours before the next dose. This sustained effect is consistent with the high blood levels observed. The reduction in the mean heart rate with the drug was moderate and none of the patients developed significant bradycardia or prolongation of the PR interval. The number and duration of episodes of ST segment depression were reduced by verapamil compared with placebo and this change was seen both during the day and at night. Effect on angina. Verapamil SR decreased the number of anginal attacks and sublingual nitroglycerin consumption, although only two patients became free of angina while on therapy for 4 weeks. In an earlier study (14) from our de- JACC Vol. 9. No. 3 March 1987:615- 21 partment in which 28 patients were given the standard formulation of verapamil, 120 mg three times daily for 4 weeks, II patients became free of angina on treadmill exercise. Side effects. Side effects with Verapamil SR were infrequent. Two patients developed mild constipation, which is known to occur in about 30tK of patients taking verapamil (22). One of our patients experienced a withdrawal syndrome after starting placebo therapy after 2 weeks of Verapamil SR. Withdrawal effects after sudden cessation of calcium antagonists have been recognized and have been reported with verapamil (23-26). Conclusions. Our data indicate that Verapamil SR (360 mg) is an effective antianginal agent when administered once daily and that its actions are sustained over a 24 hour period. It is also well tolerated and side effects are infrequent, the main being constipation as is the case with the standard formulation. Comparison with previous studies suggests that efficacy might be improved by using a larger dose, but this remains to be established in further trials. We are grateful to Miss B. Patel for her clerical assistance and Mr. W. Muniweera for technical help. We thank Revlon Health Care Ltd. for support and for the supply of the drugs. References I. Singh BN. Treatment of arrhythmias with verapamil. Lancet 1970;I: 563-4 . 2. Neumann M. Luisada AA. Double blind evaluation of orally administered lproveratril in patients with angina pectoris. Am J Med Sci 1966;251:552- 6. 3. Bala Subramanian V. Bowles M. Lahiri A. Davies AB. Raftery EB. Long term antianginal action of verapamil assessed with quantitated serial treadmill stress testing. Am J Cardiol 1981 ;48:529-35. 4. Khurmi NS. O'Hara MJ. Bowles MJ, Bala Subramanian V. Raftery EB. Randomized double-blind comparison of galloparnil and propranolol in stable angina pectoris. Am J Cardiol 1984;53:684- 8. 5. Ellestad MH, Blornqvist CG. Naughton JP. Standards for adult exercise testing laboratories. Circulation 1979;58:42 1A- 30A. 6. Bala Subramanian V. Lahiri A. Raftery EB, Green H. Stolt FD. Ambulatory ST segment monitoring. Problems. pitfalls. solutions and clinical application. Br Heart J 1980;44:419- 25. 7. Bala Subramanian V. Khurmi NS. Bowles MJ. O'H ara M_ Rafter) EB. Objective evaluation of three dose levels of diltiazem in patients with chronic stable angina. J Am Coli Cardiel 1983; I:11 44 -53. 8. Khurrni NS. Bowles MJ. Bala Subramanian V, Raftery EB. Short and long term efficacy of nicardipine assessed by placebo-controlled single and double-blind crossover trials in patients with chronic stable angina. J Am Coil Cardiol 1984;4:908- 17. 9. Cole SJc. Flanagan RJ. Johnston A, Holt DW. Rapid high-performance liquid chromatographic method for the measurement of verapamil and nor-verapamil in blood. plasma or serum. J Chrornatogr 1981:2 18; 62 1-6 . 10. Sandler G, Clayton GA. Thornicroft SG. Clinical evaluation of verapamil in angina pectoris. Br Med J 1968;3:224- 7. II. Livesley B. Cauley PF. Campbell RC. Oram S. Double-blind evaluation of verapamil, propranolol and isosorbide dinitrale againvt a placebo in the treatment of angina pectoris. Br Med J 1973;I:375- 8. l ACC Vol. 9, No.3 March 1987:615-21 12, Andersson F, Boye E, Christofferson E, et al. Assessment of verapamil in the treatment of angina pectoris, Eur J Cardiol 1975;234:443- 8. 13. Bala Subramanian V, Lahiri A, Paramasivan P, Raftery EB. Veraparml in chronic stable angina: a controlled study with computerized treadmill exercise. Lancet 1980;1:841- 4. 14, Bala Subramanian V, Bowles MJ. Khurmi NS, Davies AD, Raftery EB. A randomized double-blind comparison of verapamil and nifedipine in chronic stable angina. Am J Cardiol 1982;50:696-703. 15. Bala Subramanian V, Bowles MJ, Khurmi NS, Raftery EB. Comparative evaluation of four slow channel blockers with propranolol in stable angina pectoris (abstr). Circulation 1982;66(suppl 11): 11-8 . 16. Subramanian VB, Bowles MJ. Davies AB, Raftery EB. Calciumchannel blockade as primary therapy for stable angina pectoris. A doubleblind placebo-controlled comparison of verapamil and propranolol. Am J Cardiol 1982:50:1158-63. 17. Schomerus M, Spiegelhalder B, Stieren B, Eichelbaum M. Physiologic disposition of verapamil in man. Cardiovasc Res 1976;10:605-12 . 18. McAllister RG, Kirsten EB. The pharmacology of veraparnil. IV. Kinetic and dynamic effects after single intravenous and oral doses. Clin Pharmacol Ther 1982;31 :41 8-23. 19. Eichelbaum M, Ende M, Ranberg G. Schomerus M. Dengler HJ. The metabolism of C-D-L-verapamil in man. Drug Metab Dispos 1978;7: 145-50. KOHLI ET AL. SUSTAINED RELEASE VERAPAMIL IN ANGINA 621 20. Woodcock BG, Schulz W, Kober G, Rietbrock N. Direct derermination of hepatic extraction of verapamil in cardiac patients. Clin Pharmacol Ther 1981;30:52- 6. 21 . Norris RJ. Muirhead DC, Christie RB. Devane JG. Bottini PB. The bio-availability of a slow-release verapamil formulation. Br J Clin Pract 1985;39(suppl 42):9-15 . 22. Bala Subramanian V, Bowles MJ. Penalver H, Davies AB, Raftery EB. Verapamil in ischaemic hean disease- an objective study in 100 patients. In: Zancheui A, Krikler DM, eds. Calcium Antagonists in Cardiovascular Therapy. Amsterdam: Excerpta Medica, 1981:11 8. 23. Bala Subramanian V, Bowles MJ. Khurmi NS, Davies AB, O'Hara MJ. Raftery EB. Calcium antagonist withdrawal syndrome: objective demonstration with frequency modulated ambulatory ST-segment monitoring. Br Med J 1983;286:520-1. 24. Richmond DR, Freedman B, Kelly DT. Coronary spasm effect on withdrawal of vasodilation therapy (abstr). Aust NZ J Med 1980;10: 376. 25. Raftery EB. Cardiovascular drug withdrawal syndromes. A potential problem with calcium antagonists'! Drugs 1984:28:371-4. 26. Lahiri A, Dasgupta P. Rodrigues ER, Carboni GP, Cashman PMM, Raftery EB. Acute withdrawal of therapy in patients with chronic stable angina treated with verapamil. Drugs (in press).