Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
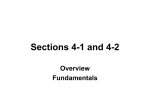
Factors Influencing Medication Assisted Treatment in Ohio Halfway Houses and Community Based Correctional Facilities Kimberly Sperber, PhD Director Amber N. Manzo, MS Senior Research Associate This research was supported by grant number 2014-JG-E01-6020, awarded by the Office of Criminal Justice Services, Edward Byrne Memorial Funding, to Talbert House. Points of view or opinions contained within are those of the authors and do not necessarily represent the official opinions or policies of the U.S. Department of Justice or the Office of Criminal Justice Services. Setting the Stage • Opiate overdose is the second leading cause of injury related death nationally, surpassed only by car accidents (Nosyk et al., 2013). • In Ohio, accidental overdoses are the leading cause of death and have been since 2007. – 472% increase in drug overdose deaths from 1999 to 2013 (Ohio Department of Health, 2015). • These deaths cost Ohio $3.6 billion annually, with nonfatal overdoses costing an additional $31.9 million. Setting the Stage • Number of Ohio substance abuse treatment clients with a primary diagnosis of opioid dependence rose from 5790 in FY01 to 24,833 in FY12. • The largest percentage of clients with this diagnosis in any county in FY01 was 14.3%; in FY12 it was 69.7%. Ohio Department of Health Increased Risk • Overall increase in persons with opioid disorders = increase in community corrections clients with opioid disorders • Increased risk to correctional programs and their clients: – – – – AWOLs Program failures Recidivism Death Investigating Barriers to MAT in Community Corrections (2015) • Study Methodology – Replication of National Institutes of Health studies conducted in private and public substance abuse programs – Replicated in Ohio halfway houses and CBCFs – Sought to examine (1) barriers to medication assisted treatment (MAT) and (2) staff attitudes toward MAT. – Funded by OCJS Data Collection • Structured, face-to-face interview with select key staff – – – – Program Director 1 Clinical Supervisor 2 Counselors 1 Medical • Use of structured interview guide to gather information on key independent variables within a number of domains. • Completed 181 key informant interviews Data Collection • Staff Surveys to all staff in each facility – Knowledge about MAT – Beliefs about the effectiveness and appropriateness of MAT for offenders – Endorsement of myths about MAT • 1876 surveys distributed • Response rate = 49% (n=910) Sample Findings INTERVIEW RESPONSES Program Characteristics • 28 halfway houses, 21 CBCFs • Estimates of opioid abuse/dependence on average of 44% for HHs and 64% for CBCFs • 61.2% had no detox services available – 34.7% had access to external detox providers, while only 4.1% provided their own detox Access to Medical Staff Item Finding physicians who are willing to contract with correctional treatment programs to provide primary care services to clients? Finding physicians or psychiatrists who are willing to contract with correctional treatment programs to provide mental health care to clients? Finding physicians with experience treating clients with substance abuse disorders? Finding nurses who are willing to contract with correctional treatment programs to provide primary care services to clients? Finding nurses who are willing to contract with correctional treatment programs to provide mental health care to clients? Finding nurses with experience treating clients with substance abuse disorders? Percent Indicating “Somewhat Easy” or “Very Easy” 51.7 50.6 46.9 38.5 51.3 46.8 Role of Single State Agency Item OHMAS is supportive of the use of medications for treating substance abuse in community corrections settings. OHMAS has adequately disseminated information about how to implement medication-assisted treatment in community corrections programs. OHMAS has offered sufficient training opportunities about using medications to treat substance abuse. Percent of PDs Indicating “Agree” or “Strongly Agree” 83.0 37.5 36.2 Accessing Info on MAT Item Journals, newsletters, or other professional (trade) publications? Percent Indicating “Moderate” to “Very Great” Extent 54.8 Contacts or promotional materials from pharmaceutical companies? 29.2 Conversations with staff of other substance abuse treatment organizations? 76.2 Ohio Mental Health and Addictions Services? 58.5 Ohio Department of Rehabilitation and Correction? 58.0 National Institute on Drug Abuse’s website and publications? 43.5 NIDA’s annual “Blending” conferences? 8.6 Your area’s Addiction Technology Transfer Center (ATTC)? Technical Assistance Publications (TAPs), Treatment Improvement Protocols (TIPs), and other publications from the Center for Substance Abuse Treatment (CSAT)? 9.2 35.4 Medical Staff Barriers Item Procedures to refer and approve a client for medication-assisted treatment. Time required to adequately assess and monitor clients for adherence, side effects, and progress. Additional documentation requirements. Inadequate frequency of urinalysis available to adequately monitor clients on medication-assisted treatment. Lack of knowledge by non-medical staff about the medications in use at the facility to treat substance use disorders. Line staff send provide contradictory messages to clients about the effectiveness of medications for substance abuse treatment. Percent Indicating “Moderate” to “Very Great” Extent 49.9 24.0 27.3 18.2 72.8 27.3 What Do 910 Practitioners Have to Say? SURVEY RESPONSES Staff Characteristics Characteristic Percent Female 59.3 1st Shift 72.1 At Least 4 Year Degree 54.8 Administration 20.3 Clinical 27.7 Medical 1.1 Security/Operations 40.7 Other Positions 9.2 In Recovery 9.1 Diffusion and Staff Perceptions by Medication Distribution of pharmacotherapy diffusion and staff perceptions, % or mean (SD) Variable Dependent variables Diffusion Perceived effectiveness Perceived acceptability Buprenorphine 35.1% 1.95 (.82) 2.06 (1.08) Methadone 37.2% 1.80 (.80) 1.81 (1.01) Oral Naltrexone 55.4% 2.31 (.90) 2.54 (1.20) Vivitrol 44.0% 2.74 (.99) 2.83 (1.20) Summary of Variable Impact on Odds of Endorsing an Opinion about Each Medication Injectable Naltrexone Variable Methadone Buprenorphine Oral Naltrexone Parent agency Not Significant Not Significant Increased Odds Increased Odds Female Increased Odds Increased Odds Not Significant Increased Odds Hours worked Not Significant Not Significant Not Significant Not Significant Clinical position Not Significant Not Significant Decreased Odds Not Significant Operations position Decreased Odds Decreased Odds Decreased Odds Decreased Odds Recovery status Increased Odds Increased Odds Not Significant Not Significant Level of education Increased Odds Increased Odds Not Significant Not Significant Information on MAT Increased Odds Increased Odds Increased Odds Increased Odds 12-step orientation Not Significant Decreased Odds Not Significant Not Significant Facility provides MAT Increased Odds Not Significant Increased Odds Increased Odds Increased Odds Increased Odds Increased Odds Increased Odds Not Significant Not Significant Increased Odds Increased Odds Facility provides access to MAT Works in a CBCF Summary • Sufficient information on MAT and working in a facility that provided some level of MAT was predictive of diffusion across all 4 medications • Operations status predictive across all 4 medications; negative relationship • Gender predictive across 3 of the 4 medications • 12-step orientation only predictive of Buprenorphine diffusion; negative relationship • Gender, recovery status, level of education consistent predictors of diffusion for methadone and buprenorphine Practitioner Knowledge About MAT • Operations staff provided significantly lower ratings of agreement on items that reflected benefits of MAT – – – – – – Reduces relapse Increases employment Reduces crime Reduces or blocks the effects of opioids Increases family stability Improves birth outcomes for children born to addicted mothers. • They provided significantly higher ratings of agreement to items indicating beliefs about negative outcomes of MAT – MAT rewards criminals for being drug users and interferes with the ability to drive a car. • Supervisory staff provided significantly higher ratings of agreement than both groups of line staff for two items – MAT lowers death rates and MAT increases program retention. Staff Opinions and Concerns • Operational staff were more likely to agree with negative statements associated with medicationassisted treatment. • These items were: – Using medications to treat addiction is substituting one drug for another. – Using medications to treat addiction in correctional programs causes too many problems with diversion and contraband within the facility. – Medications are drugs and you cannot be clean if you are taking drugs. – Using medication in substance abuse treatment is promoting the pharmaceutical companies. Summary of Variable Impact on Odds of Agreeing that Each Medication is Acceptable Variable Methadone Buprenorphine Oral Naltrexone Injectable Naltrexone Parent agency Not Significant Not Significant Not Significant Not Significant Female Not Significant Not Significant Not Significant Increased Odds Hours worked Not Significant Not Significant Not Significant Not Significant Recovery status Not Significant Not Significant Not Significant Not Significant Staff beliefs Not Significant Increased Odds Increased Odds Increased Odds Education level Not Significant Not Significant Not Significant Increased Odds 12-step orientation Not Significant Not Significant Not Significant Not Significant Staff information Not Significant Not Significant Not Significant Not Significant Facility provides MAT Decreased Odds Not Significant Increased Odds Increased Odds Clinical staff Not Significant Not Significant Decreased Odds Not Significant Operations staff Not Significant Not Significant Decreased Odds Decreased Odds Works in CBCF Not Significant Decreased Odds Not Significant Not Significant Staff concerns Decreased Odds Decreased Odds Decreased Odds Not Significant Summary • • • Staff who demonstrated a higher level of agreement with statements indicating positive outcomes of MAT were significantly more likely to endorse the use of buprenorphine, oral naltrexone, and injectable naltrexone as acceptable. Higher endorsement of items reflecting concerns with MAT produced a significantly lower odds of agreeing that three of the medications were acceptable for use with correctional clients; these medications were methadone, buprenorphine, and oral naltrexone. While not statistically significant at the p=.05 level, staff concerns did approach significance as a predictor of acceptability for injectable naltrexone as well (p=06). Working in a facility that directly provided MAT was also a statistically significant predictor of endorsing the acceptability of methadone, oral naltrexone, and injectable naltrexone. it served to decrease the probability that staff would endorse methadone as acceptable, however. Summary of Variable Impact on Odds of Agreeing that Each Medication is Effective Injectable Naltrexone Variable Methadone Buprenorphine Oral Naltrexone Parent agency Not Significant Not Significant Not Significant Not Significant Female Not Significant Not Significant Not Significant Not Significant Hours worked Not Significant Not Significant Not Significant Not Significant Recovery status Not Significant Not Significant Not Significant Not Significant Staff beliefs Increased Odds Increased Odds Increased Odds Increased Odds Education level Not Significant Not Significant Not Significant Not Significant 12-step orientation Not Significant Not Significant Not Significant Not Significant Staff information Not Significant Not Significant Not Significant Not Significant Facility provides MAT Not Significant Not Significant Increased Odds Not Significant Clinical staff Not Significant Not Significant Not Significant Not Significant Operations staff Not Significant Not Significant Decreased Odds Decreased Odds Works in CBCF Decreased Odds Decreased Odds Not Significant Not Significant Staff concerns Decreased Odds Not Significant Not Significant Not Significant Summary • Endorsement of outcomes predictive across all 4 medications • MAT implementation was predictive of perceptions of effectiveness of only one medication – oral naltrexone • Working as operations staff predicted lower endorsement of effectiveness for both forms of naltrexone • Working in a CBCF predicted lower endorsement of effectiveness for methadone and buprenorphine • Higher endorsement of concerns associated with MAT was predictive of lower endorsement of effectiveness of methadone only Implications • Identification of key structural barriers to MAT adoption in community corrections settings • Overall low diffusion of knowledge about MAT • Overall low ratings of acceptability and effectiveness of MAT • A mixture of individual and organizational attributes that may be important to future efforts to change staff perceptions Practitioner Toolkit • Staff Education – Fact Sheets – Webinars • Advocacy • Implementation – Implementation Matrix • Client Education Staff Education - Sample Topics • Brain science • Addiction as a chronic care condition • Understanding the role of medication in long-term recovery • Myth busting • Scope of practice Substance Use and the Brain • Repeated use of addictive drugs eventually changes how the brain functions • These changes can last for months or even years • These changes accompany the transition from abuse to addiction and may continue to increase risk of relapse even once someone has stopped using drugs Objective Evidence NIDA (2007) Bringing the Power of Science to Bear on Drug Abuse and Addiction. Rockville, MD : U.S. Dept. of Health and Human Services, National Institutes of Health. Cognitive Deficits • Memory • Difficulty with abstraction • Diminished impulse control • Brain performs similarly to an individual with brain damage Addiction as Chronic Care Condition • Many with addiction will require multiple episodes of treatment over the course of years before demonstrating any sustained period of recovery • In one study, estimated median time from first use to at least 1 drug-free year was 27 years • Estimated median time from first treatment to 1 alcohol and drug-free year was 9 years with 3-4 episodes of treatment (Dennis et al., 2005) • Time to recovery is also impacted by age of first use and duration of use prior to treatment Understanding the Medications • What is the difference between an agonist, a partial agonist, and an antagonist? • How do these medications function? • How do these medications function differently from heroin? Opioid Medications High Opioid Effect Full Agonist (e.g., methadone) Activate opioid receptor in the brain; subjective feeling of “high” Block the opioid receptor; NO subjective feeling of “high” Partial Agonist (e.g. buprenorphine) Antagonist (e.g. naloxone) Low Dose of Opioid SOURCE: ATTC Developed by Dr. Erin Winstanley for Talbert House Phases of MAT • Detoxification – Weaning patients off of addictive substances and managing withdrawal – Used alone, we see high rates of relapse • Stabilization – Withdrawal management, assessment, medication induction, psychosocial counseling Phases of MAT • Maintenance – Medication maintenance and deeper counseling work • Ongoing Rehabilitation – Patient and provider might choose to wean from medication or pursue indefinite medication maintenance • SAMHSA consensus group recommended that patients never be coerced into tapering off of their medications – Decision is to be jointly made between physician and patient Myths • MAT substitutes one addiction for another • Addiction medication is a crutch that prevents true recovery • MAT should not be long term Scope of Practice • Prohibitions against MAT and implications for Americans with Disabilities Act and Rehabilitation Act of 1973 • Implications of recommendations against MAT made by non-medical professionals • Agency policy versus individual staff opinion The Opioid Crisis Continues Current CHHSR Projects Complicating Factors • The recent influx of fentanyl has served to further exacerbate the risk of overdose deaths in Ohio – Number of fentanyl overdose deaths increasing 500% from 2013 to 2014 – Ohio leads the country in the number of confiscations by law enforcement of illicit fentanyl. The second highest rate of confiscations is in Massachusetts, which is only about half that of Ohio. – According to a 2015 Center for Disease Control EpiAid report on risk factors for fentanyl-related overdose deaths in Ohio, the highest fentanyl overdose rates can be found in Hamilton, Montgomery, Summit, Butler, Cuyahoga, and Clermont Counties. Complicating Factors • Risk factors associated with an increased risk of a fentanyl-related overdose death included: – Age, gender, current mental health problem, history of a substance abuse problem, history of opioid abuse, lower education, and recent release from a correctional institution. Reentry and Risk of OD • Highest risk time for a drug overdose for individuals involved in the criminal justice system is 2 weeks postrelease from a correctional facility. • For example, a 2010 meta-analysis found that drug overdose was the cause of 59% of deaths within 3 months of release from prison and 76% of deaths within 2 weeks of release. • Research findings demonstrate that the relative risk of death post-release is 3 to 8 times higher during first 2 weeks compared with the subsequent 10 weeks postrelease. Current CHHSR Statewide Study 2016 • Factors Influencing Opioid Overdose Preventions and Response Practices in Ohio Community Corrections and Substance Abuse Programs • Includes HHs, CBCFs, OP substance abuse, residential substance abuse Methodology • Telephone interview with program director • Use of semi-structured interview guide • Anonymous, paper-and-pencil survey of staff – Random selection of half Areas of Interest • Document the prevalence of naloxone distribution (ND) programs • Document prevalence of structured overdose prevention education programs • Identify barriers to naloxone distribution programs and OD prevention programs • Examine staff attitudes toward ND programs and OD prevention programs Development of OOPP • Structured, replicable approach to education • OOPPs have been shown to: – Increase knowledge of overdose prevention and overdose risk factors – Increase application of such knowledge during overdose events – Increase the ability to respond appropriately in overdose situation Agency-Wide Initiatives • Opioid Oversight Committee • Mandatory Opioid 101 training for all staff • Community outreach • Drug lab testing for fentanyl Conclusions • We treat and supervise a population at high risk for opioid addiction, overdose, and death • We have a responsibility to deploy evidencebased practices to best of our ability • Requires an understanding of all barriers and opportunities • Requires long-term planning and advocacy Questions & Answers [email protected]