Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
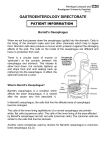
Barrett’s oesophagus What is Barrett’s oesophagus? The gullet (oesophagus) is a muscular tube that transports food from the mouth to the stomach. Barrett’s oesophagus (also known as columnar lined oesophagus) is when abnormal cells develop in the lining of the lower part of the gullet. It was first identified in the early 1950’s, by a surgeon called Norman Barrett. What causes Barrett’s oesophagus? The main cause is due to acid from the stomach splashing up into the gullet. This is called reflux. The stomach has a lining that is resistant to acid but the gullet does not. The acid may cause the lining of the gullet to become inflamed and painful (eg. heartburn). The oesophagus normally heals with time and the lining returns to normal however, sometimes it heals in a different way and this is Barrett’s oesophagus. What causes reflux? Normally a valve at the bottom of the gullet prevents reflux but sometimes it is ineffective and this can be due to: • Hiatus Hernia (when the stomach pushes up into the chest through the diaphragm causing the valve to stay open). • Some medications. • Lifestyle, for example: 1. Alcohol, nicotine, caffeine and peppermint all cause this valve to relax, allowing acid up into the gullet. 2. Fizzy drinks, large meals, fatty foods and being overweight all cause the stomach to be full for longer periods of time which encourages reflux. What are the signs and symptoms of Barrett’s oesophagus? There may be none or you may get one or more of the following: heartburn (often described as a burning sensation in the chest); indigestion; difficulty with or uncomfortable swallowing; and water brash (fluid coming up into the mouth). How is it diagnosed? It is diagnosed during a gastroscopy examination, when biopsies (small tissue samples) are taken and examined in the laboratory under the microscope. Although it is diagnosed in this way, Barrett’s oesophagus can often be seen down the gastroscope as lengths of red velvet looking lining. Why is it a concern? Over a long period of time it can occasionally lead to a pre-cancerous condition (dysplasia). This is when cells in the affected area continue to grow and reproduce and become increasingly abnormal. Approximately ½% - 1% of people in the UK have Barrett’s oesophagus, however less than 5% go on to develop gullet (oesophageal) cancer. How is it managed? This depends on several factors and needs to be discussed on an individual basis with your specialist. Regular gastroscopies may need to be carried out to monitor the condition. Reflux is treated with acid reducing medication and with lifestyle changes as relevant. An operation may be necessary, but this is in exceptional cases. Useful contacts Ann Stokes, Dyspepsia Nurse Specialist Royal Derby Hospital Uttoxeter Road Derby DE22 3NE Telephone: 01332 786754 Mobile: 07827 283089 Email: [email protected] References BRITISH SOCIETY OF GASTROENTEROLOGY (2005) Guidelines for the diagnosis and management of Barrett’s columnar-lined oesophagus. London, British Society of Gastroenterology NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE (2004) Dyspepsia: Management of dyspepsia in adults in primary care. London, National Institute for Clinical Excellence Any external organisations and websites included here do not necessarily reflect the views of the Derby Hospitals NHS Foundation Trust, nor does their inclusion constitute a recommendation. Reference Code: P0681/1352/03.2010/VERSION2 © Copyright 2010 All rights reserved. No part of this publication may be reproduced in any form or by any means without prior permission in writing from the Patient Information Service, Derby Hospitals NHS Foundation Trust. (G10263/09.2006/V1)