Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
760
Alteration of the Cytosolic-Mitochondrial
Distribution of High-Energy Phosphates During
Global Myocardial Ischemia May Contribute to
Early Contractile Failure
Ursula Rauch, Karsten Schulze, Bernhard Witzenbichler, Heinz P. Schultheiss
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
M
Abstract Depending on its duration, temporary myocardial
ischemia leads to a disturbance of myocardial function before
irreversible cellular necrosis is developed. Mechanical, electrical, and metabolic disturbances were suggested to be possible
mechanisms accounting for the altered mechanical performance in ischemic hearts. To further investigate the alteration
of myocardial energy metabolism on the subcellular level, we
determined, by means of nonaqueous fractionation, the cytosolic-mitochondrial distribution of high-energy phosphates
and other metabolites (ATP, ADP, phosphocreatine, creatine,
and inorganic phosphate) in ischemic (zero-flow) guinea pig
hearts after isolated perfused working heart preparation.
Additional experiments using 31P nuclear magnetic resonance
spectroscopy were performed to determine pHi and [Mg 2+]i
changes during global ischemia. The total ATP content of
myocardial tissue dropped only slowly to 76% of control ATP
at 10 minutes and to 51% at 30 minutes and reached almost
zero at 60 minutes of ischemia. However, striking differences
were observed on the subcellular level: While cytosolic phos-
phocreatine was almost completely consumed after 3 minutes
of ischemia (from 19.1±+1.6 to 3.3+0.5 mmol/L), ATP concentration in the cytosol decreased within 30 minutes from
8.4±0.6 to only 5.4±0.9 mmol/L. Mitochondrial ATP was
rapidly and linearly reduced to 60% after 5 minutes of
ischemia and was nearly unmeasurable after a further 20
minutes. Thus, in contrast to the breakdown of phosphocreatine in cytosol, the only slight alteration of cytosolic ATP
reveals a reduction in cytosolic ATP utilization. Moreover, the
unaffected cytosolic-mitochondrial difference in the phosphorylation potential of ATP demonstrates the intact function of
the ADP/ATP carrier during early ischemia. These results
might indicate a disturbance of the functional coupling between carrier and phosphocreatine kinase (phosphocreatine
shuttle), which could be of importance for the early contractile
failure in myocardial ischemia. (Circ Res. 1994;75:760-769.)
Key Words * myocardial ischemia * early contractile
failure * compartmentation of high-energy phosphates .
ADP/ATP carrier * phosphocreatine shuttle
'yocardial ischemia leads to contractile failure
latter of these hypotheses, considering energy metabolism during ischemia. We observed changes in the
compartmentation of high-energy phosphates that occur during depletion of oxygen and substrates.
Although the mitochondrial ATP production diminishes in acute ischemia because of a lack of oxygen
supply, several investigators have shown that the ATP
content of the myocardial tissue remains nearly constant
over the first minutes of ischemia, whereas the phosphocreatine (CP) pool decreases rapidly.1'2,'5 Disturbances in energy utilization16'7 and failure in energy
transport processes have been proposed to help understand these observations.
Mainly two compartments of the myocyte have to be
considered in energy metabolism: the mitochondrial
matrix space in which ATP is produced by oxidative
phosphorylation and the cytosolic space where it is
dephosphorylated by the energy-consuming reactions.
Because of the impermeability of the inner mitochondrial membrane for these hydrophilic adenine nucleotides, a well-characterized ADP/ATP carrier imports
cytosolic ADP into the mitochondrial compartment in a
counterexchange with newly synthesized mitochondrial
ATP. A reduced function of the ADP/ATP carrier has
been suggested to contribute to the altered mechanical
performance during ischemia.18 The present study attempts to clarify the impact of ischemia on the mitochondrial energy status with special focus on the fune-
s j
before apparent cell damage and necrosis.1
The contractile function of hearts subjected
to global ischemia declines rapidly during the first few
minutes after the onset of ischemia.23 The mechanism
of this contractile dysfunction has not yet been fully
explained. Several hypotheses concerning mechanical,
electrical, and metabolic alterations have been discussed, such as (1) a decrease of perfusion pressure in
the vascular system leading to reduced myofibril length
and a decline in pressure development,3-5 (2) depression and shortening of the action potential6-8 as well as
reduced Ca'+ release from the sarcoplasmic reticulum,8'9 affecting the excitation-contraction coupling of
the heart, (3) accumulation of inorganic phosphate10'11
and protons,12 which interfere with myofilaments and
other important proteins, and (4) depletion of highenergy phosphates and changes of the free energy of
ATP hydrolysis.13'4 Our present work refers to the
Received September 23, 1993; accepted June 16, 1994.
From Medizinische Klinik B, Heinrich-Heine Universitat, Dus-
seldorf, Germany.
Presented in part at the 65th Scientific Sessions of the American
Heart Association, New Orleans, La, November 1992.
Correspondence to Heinz-Peter Schultheifi, MD, Medizinische
Klinik B, Heinrich-Heine Universitat, Moorenstr 5, 40225 Diisseldorf, Germany.
C 1994 American Heart Association, Inc.
Rauch et al High-Energy Phosphates and Myocardial Ischemia
tion of the ADP/ATP carrier. No methods are available
for direct determination of the function of the ADP/
ATP carrier in vivo. Thus, its transport activity was
assessed by measuring compartmental changes in highenergy phosphate concentration and phosphorylation
potentials.
Experiments were performed on working guinea pig
hearts, a well-characterized model to study myocardial
hypoxia and ischemia.'819 After early and advanced
periods of zero-flow ischemia up to 60 minutes, subcellular high-energy phosphate contents in the myocardial
tissue were measured by nonaqueous fractionation. The
phosphorylation potentials of ATP in mitochondria and
cytosol were calculated from these metabolic data.
Materials and Methods
Materials
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
Substrate, enzymes, and coenzymes for enzymatic analyses
were purchased from Boehringer Mannheim and from Sigma
Chemical Co. Protein was calibrated with 100% purified
bovine serum albumin from Behringwerke AG. All chemicals
used for high-performance liquid chromatography (HPLC)
were from E. Merck and from Pierce Chemical Co.
Working Heart Preparation and Perfusion
The hearts of guinea pigs with a body weight of 200 to 300
g were isolated and perfused as described in detail by Becker
et a120 and Bunger et al.21 Briefly, the thorax was opened, and
the heart was rapidly excised through median thoracotomy and
immersed in an ice-cold physiological NaCl solution. The aorta
was dissected free from surrounding tissue and connected to
the perfusion apparatus. Langendorff retrograde perfusion22
was introduced with a modified Krebs-Henseleit buffer containing (mmol/L) NaCl 127, KCl 4.7, NaHCO3 24.9, CaCl2
1.25, MgSO4 0.6, KH2PO4 1.2, pyruvate 0.3, and glucose 5.5,
along with S U/L insulin. The nonrecirculating perfusion
medium was calibrated to pH 7.4 with 94.4% 02/5.6% CO2 at
37°C. These conditions were provided to ensure adequate
substrate and oxygen availability to the myocardium.
After a first stabilization period of 20 minutes, perfusate was
applied to the left ventricle via the cannulated left auricle. All
other atrial veins were ligated except the coronary sinus, which
was drained through the pulmonary artery.
Atrial filling pressure and aortic pressure were continuously
recorded by Statham P23DB strain gauges (Gould). Heart rate
was taken from the phasic pressure signals with a heart-rate
module (HRM type 669, Hugo Sachs Elektronik). External
heart work was calculated from the pressure-volume work of
the left ventricle and acceleration work during ejection. Two
Clarke-type electrodes (Bachofer) were used to determine the
myocardial oxygen consumption, which was derived from the
difference of oxygen tension between aortic perfusate and
coronary effluent.
Experimental Protocol
Retrograde Langendorif perfusion of the isolated guinea pig
hearts was maintained for an equilibration period of 20
minutes to obtain a steady state of substrate and oxygen
consumption. Perfusion was then continued in the antegrade
"working modes" with a preload of 12 mm Hg and an afterload
of 60 mm Hg. After =15 minutes, hemodynamic parameters,
coronary flow, and oxygen consumption were recorded. After
30 minutes of the heart in the working state, global ischemia
was applied to the heart by clamping atrial and aortic cannulas.15 During ischemic periods of 0.5, 1, 3, 5, 10, 20, 30, and 60
minutes, the temperature of the myocardium was kept at a
constant level by immersing it in nonoxygenated buffer at
37°C. The ischemic phase was stopped by clamping the myo-
761
cardium between aluminum blocks that had been precooled in
liquid nitrogen.
All experiments were made under steady-state conditions.
Control measurements without ischemia (n=7) were performed under stable hemodynamic conditions after 2 hours of
the heart in working state. Further investigations were carried
out to determine the concentrations of intracellular adenine
nucleotides (ATP and ADP), CP, and other substances.
Nonaqueous Fractionation of Myocardium
The frozen myocardial tissue was crushed in a mortar
containing liquid nitrogen. It was then lyophilized at -40°C
and 0.001 mm Hg for 3 days. During the lyophilization process,
all dissolved metabolites, such as proteins, enzymes, highenergy phosphates, and other substances, were fixed onto the
membranes of their respective cellular compartments. The
myocardial membranes of the freeze-dried tissue were broken
up into a homogenate of small membrane fragments by
sonicating the tissue for 4 minutes at 5-second intervals
(Sonifier 250 Branson, Sonic Power Co). Purification of the
homogenate was achieved by successive filtration through
columns filled with glass beads of different diameters (1.0 to
0.5 mm).
Because of the higher density of the cytosolic versus the
mitochondrial membrane particles, compartmental enrichment
of the purified tissue homogenate was achieved by heptane/
carbon tetrachloride density gradient centrifugation for 4 hours
at 16 00(g (Sorvall RC-SB refrigerated superspeed centrifuge
with swing-out rotor, Du Pont Instruments). The gradient yielded
eight fractions containing different proportions of cytosolic and
mitochondrial proteins. The fractions were dried in a desiccator.
In a first aliquot, the activities of the cytosolic marker enzyme
phosphoglycerate kinase (PGK), the mitochondrial marker enzyme citrate synthase (CS), and the total protein content were
analyzed. The concentrations of high-energy phosphates, creatine, and inorganic phosphate were determined in a second
aliquot. The protein content was obtained as described by Lowry
et a123 by using an Eppendorf filter photometer model 940 from
Kontron Instruments. The measurements of the activities of
PGK and CS and the determination of creatine and inorganic
phosphate were performed by enzymatic analyses.24 All enzymatic tests were performed with a dual-beam dual-wavelength
spectrophotometer (Sigma ZFP 22, Biochem) by using 366 nm as
the measuring wavelength and 405 nm as the reference wavelength. Adenine nucleotide and CP concentrations were measured with HPLC.
Measurement of Adenine Nucleotides and
CP by HPLC
Adenine nucleotides (ATP and ADP) were separated from
each other by using reverse-phase ion-pairing HPLC as described previously by Hammer et al,25 whereas CP content was
determined according to Juengling and Kammermeier.26 First,
the aliquots of the heart tissue had to be prepared for HPLC
use, which included deproteinization and extraction of the
different constituents into a solvent. Therefore, perchloric acid
(0.6N) was mixed with each sample and, after centrifugation,
was neutralized with ice-cold trioctylamine and Freon (1:4
mixture). Between each preparation step, all aliquots were
kept on ice to avoid the danger of a decay of high-energy
phosphates. The aqueous extract was then used for adenine
nucleotide and CP determination by reverse-phase ion-pairing
HPLC.
A Kontron HPLC system consisting of two pumps, a 430 UV
detector with variable wavelengths, a refrigerated automatic
injector system (autosampler 460), and a computer data system
for solvent delivery programming and peak area integration
was available. Separations were carried out with an OSD
Hypersil reversed-phase column (Hewlett Packard).
All preparations were made with highest purified water
(HPLC grade). For adenine nucleotide analysis, two different
762
Circulation Research Vol 75, No 4 October 1994
aqueous buffers were used as mobile phase: buffer A, containing 30 mmol/L KH2PO4 and 7.5 mmol/L tetrabutylammonium
phosphate at pH 5.45, and buffer B, consisting of 50%
acetonitril and 50% KH2PO4 (30 mmol/L) at pH 7.0. The
aqueous eluate for CP measurement contained 0.2% KH2PO4
and 0.3% tetrabutylammonium phosphate at pH 3.0. All
solvents were filtered through a 0.2-,um Millipore membrane
and degassed with helium before being applied to the HPLC
column. The detector wavelengths were set at 254 and 210 nm
for adenine nucleotide and CP separation, respectively.
The metabolite concentrations of each aliquot were quantified by comparison of peak area with that of commercially
available external standard. Standard curves were linear for all
concentrations examined.
Calculation of Intracellular Concentrations
The total metabolite content (Mtot) of each aliquot obtained
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
from the density gradient consists of mitochondrial and cytosolic portions (Mt and Mmit, respectively). The distribution of
marker enzymes CS and PGK in each fraction correlates with
the membrane and substrate content of the respective cellular
compartment. Since the relation between marker enzyme and
compartmental metabolite content remains constant (values of
M,/PGK and Mmit/CS are constant), calculations of mitochondrial as well as cytosolic substrate concentrations can be
obtained by linear regression by using the following formulas:
(1)
Mt.t= Mcy + Mmit
(2)
M<t/PGK=a
(3)
Mmit/CS =b
Combination and transformation of Equations 1 through 3
leads to
Mtot/CS=a(PGK/CS)+b
(4)
For the determination of the metabolite concentrations, cytosolic and mitochondrial contents were referred to the protein
content of the corresponding compartment.27 Calculation factors of 5.82 ,uL water per milligram cytosolic protein and 1.8
,uL water per milligram mitochondrial protein were used to
obtain the subcellular concentrations.27,28
Calculation of KCPK and Phosphorylation Potential
Because most of the cytosolic ADP is bound to the contractile filaments of the heart muscle, free cytosolic ADP had to be
calculated from the creatine phosphokinase reaction:
(5) [ATP]/[ADP]=[CP] x [H+]/([creatine] x KCPK)
The equilibrium constant for the creatine kinase reaction
(KCPK) changes as a function of pH and free intracellular Mg 2+
concentration as shown by Lawson and Veech29 and van der
Meer et al.30 The following empirical equation for the simultaneous pH and Mg 2+ dependence of KCPK was established by
Bunger et al.28:
(6) [H'YKCPK=antilog(7.52-0.97xpH+3.12[Mg2+]10.1)
The combination of 5 and 6 leads to
[ATP]/[ADP]=[CP]/[creatine]
antilog(7.52-0.97 x pH + 3.12[Mg2+]0'1 )
This formula allows the determination of the cytosolic free
ATP-to-ADP ratio for different intracellular free Mg2+ concentrations and any near-physiological pH values.
The phosphorylation potential of ATP (AGATP) was calcu(7)
x
lated from the free ATP-to-ADP ratio for both mitochondrial
and cytosolic compartments31:
(8)
AGATP=AGW+RT
x ln{[ATP]/([ADP] x [phosphate])}
where AG0 equals -31.9 kJ/mol under conditions prevailing
intracellularly,32 R is Faraday's constant, and T is the absolute
temperature in degrees kelvin.
Determination of Cytosolic pH and Intracellular
Free Mg 2+ by 31P Nuclear Magnetic
Resonance Spectroscopy
Additional experiments using 31P nuclear magnetic resonance (NMR) spectroscopy were accomplished to investigate
the alterations of pH, and free Mg 2+ concentration during
ischemia in order to calculate KcPK. Therefore, five guinea pig
hearts, isolated and perfused as described above, were placed
into a 20-mm NMR glass tube (Wilmad). The 31P NMR scans
were performed in a Bruker wide-bore vertical magnet (9.4-T,
7.0 -cm bore diameter) at a phosphorus resonance frequency of
162 MHz. Each scan represented the sum of 20 (ischemia
minutes 1 through 10) and 98 single-pulse acquisitions (preischemia, ischemia minutes 20 and 30). Acquisition parameters were as follows: size, 2000 (+2000 zero-fill); sweep width,
6000 Hz; pulse width, 170 microseconds; interpulse delay, 2.8
seconds; and line broadening, 5 Hz. The intracellular phosphate content was estimated from the pH-dependent split of
the phosphorus resonance into two partially merged peaks
representing the extracellular and the intracellular or cytoplasmatic fraction of inorganic phosphorus in the magnetic field.
Nevertheless, the spectral resolution was high enough to allow
an accurate separation of both peaks by application of a
Lorentzian line-fitting routine. To determine pH, the equation
for the chemical shift of inorganic intracellular phosphate as a
function of pH was used33'34:
(9)
pH=6.79-log[(6-5.75)/(3.25-8)]
where 8 is defined as the chemical shift (in parts per million)
of the resonance of intracellular inorganic phosphorus relative
to CP.
The intracellular free Mg 2+ concentration was estimated
from the difference of the chemical shift separation of the a
and , resonances of ATP (8, in parts per million) as a function
of free Mg 2+ and pH35:
(10)
[Mg2+]f[e=KDMgATP[(SATP- 8mATP)/
(8_ 3MgATP)_ 1]
with KDM9TP, 8A', and 6MgAT determined from calibration
solutions of an ionic strength of 0.18 mmol/L and a temperature of 370C.36 The Mg 2+ calibration was done in the physiologically and pathophysiologically relevant pH range of 6.0 to
7.8 at an ATP concentration of 5 mmol/L. For the dissociation
constant of the Mg-ATP complex (KDMgAl), a value of 38
gmol/L (at 37°C) was used. The pH-dependent end points of
the calibration curve (8AT and SMgA') were derived from the
formula recently developed by Mosher et al.36 &`'T is the
maximum value of 8. This largest chemical shift difference of
the a and f8 resonances of ATP is observed in the Mg 2+-free
calibration solution. SMgAT is the minimum value of 8 occurring at a pH-dependent Mg 2+ concentration.
The concentration values for Mg 2+ were obtained by dividing the metabolite amount by the wet weight of the heart and
by the intracellular space, which was 0.37 mL per gram wet
mass.20 In this manner, the alteration of pH, and free Mg2+
concentration was determined during a period of 60-minute
ischemia applied to guinea pig hearts according our experimental protocol (see above).
Statistical Evaluation
Student's t test for unpaired samples was used to analyze the
data statistically. Values are given as mean+SEM of n inde-
Rauch et al High-Energy Phosphates and Myocardial Ischemia
763
TABLE 1. Subcellular Metabolite Concentrations in Ischemic Isolated Perfused Guinea Pig Hearts
Subcellular Metabolite Concentration, mmol/L
Cytosol
Before ischemia
Ischemia, min
0.5
1
3
5
10
20
30
60
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
Mitochondria
Before ischemia
Ischemia, min
0.5
CP
ATP
ADP
Creatine
Phosphate
19.1 + 1.6
8.4±0.6
1.3±0.2
8.8±0.9
7.3±1.0
11.7±1.3
8.1±1.2
3.3±0.5
2.3±0.5
2.2±0.9
2.0±0.3
0.9±0.3
0.8±0.1
7.9±0.6
7.8±0.5
8.0±0.6
7.6+0.8
6.9±0.7
6.1±0.9
5.4±0.9
3.3±1.2
1.4±0.2
1.5+0.2
1.8±0.2
1.9±0.1
2.0±0.1
1.9±0.2
1.7±0.2
1.6±0.3
11.8±0.8
15.3±0.9
19.8±1.5
20.9±2.0
20.4±1.7
20.2±1.3
19.9±1.6
20.5±2.1
10.5±0.5
12.8±1.5
19.1±1.8
20.5±1.7
22.6±1.8
22.0±1.9
23.2±1.6
24.9±1.6
10.3±0.7
2.1±0.2
11.7±1.6
11.6±1.1
8.8±0.9
2.8±0.4
15.5±1.0
15.6±1.9
1
6.8±0.7
3.7±0.6
20.2±3.5
18.3±1.2
3
5.4±1.0
4.9±0.8
37.2±1.2
30.2±1.7
5
4.0±1.4
5.1±0.9
31.9±3.1
33.6±1.2
10
2.3±0.9
4.9±0.6
33.3±2.7
34.4+2.3
20
0.8±0.5
5.0±0.7
29.8±3.4
35.4±1.9
30
4.8±1.1
0.8±0.5
34.3±2.3
29.1±+1.9
60
0.6±0.6
4.6±1.2
29.5+2.3
38.4±2.8
CP indicates phosphocreatine. Values are mean±SEM. Seven control animals and 24 test animals were used for
the experiments; 3 test animals were subjected to each ischemic period of 0.5, 1, 3, 5,10, 20, 30, and 60 minutes.
Cytosolic and mitochondrial concentrations of high-energy phosphates, creatine, and inorganic phosphate were
obtained by fractionation of myocardial tissue through density gradient centrifugation in nonaqueous media using
known subcellular water contents for the cytosolic and the mitochondrial space.29,30
pendent experiments. Differences with P<.05 were regarded
as significant.
Results
Ischemic periods of 0.5, 1, 3, 5, 10, 20, 30, and 60
minutes were applied to hearts at 37°C before freeze
clamping. Effects of ischemia on energy metabolism
were determined by nonaqueous fractionation of these
frozen hearts, in particular the cytosolic and mitochondrial metabolite distribution. All results obtained from
ischemic hearts were compared with the data of control
animals, which were not subjected to ischemia.
A rapid loss of cytosolic CP from 19.1+1.6 to
11.7+1.3 mmol/L (P<.01), reaching 61% of control
values, was observed over the first 30 seconds of ischemia. After a further 3-minute period, values of 3.3 +0.5
mmol/L (P<.001) were obtained representing 17% of
the normal CP level (Table 1). It is a well-known fact
that high concentrations of CP are found in the cytosolic
space, whereas the mitochondria do not contain noticeable CP. Thus, the observed fall of the total CP content
during early ischemia takes place only in the cytosolic
compartment, and the mitochondrial CP remains near
zero (0.2±+1.2 mmol/L) during the entire period of
ischemia. The total creatine content increased continu-
ously during the rapid CP breakdown (Fig 1), whereby
creatine molecules accumulated in both compartments,
reaching nearly threefold normal creatine concentrations. Since mitochondria normally contain only small
amounts of creatine, it must be pointed out that during
reduced oxygen availability, as in ischemia, the creatine
levels start to increase even in the mitochondrial space
(Table 1).
In contrast to the rapid decline of CP, the total ATP
pool of the myocardial tissue dropped only slowly to
76% of control ATP at 10 minutes and to 51% at 30
minutes. Fig 1 shows the decrease of the whole-tissue
ATP and, adversely, the accumulation of the wholetissue ADP and inorganic phosphate during 60-minute
ischemia. Although the total ATP content diminished
quite slowly, striking differences in ATP decrease between the mitochondrial and cytosolic compartments
were observed (Table 1). The mitochondrial ATP content was rapidly and linearly reduced to 60% after 5
minutes of ischemia, and almost no ATP (<10%) was
measurable after 20 minutes. In contrast, the cytosolic
ATP decline from 8.4±0.6 to 7.6+0.8 mmol/L was very
slow and first appeared after a 10-minute period of
ischemia. The resulting rise in ADP concentration was
highest for mitochondria after 5 minutes, whereby ADP
764
Circulation Research Vol 75, No 4 October 1994
CrP [nmollmgJ
Cr [nmollmg]
l If)L
80
1
1
T
80
60 1
60
40'
40
20
20
0
0
0
20
10
40
30
lachemia [min]
60
50
i
f
20
10
0
i
30
40
Ischemia [min]
i~~~~~~~~
50
6so
50
60
ATP [nmollmg]
50
40
30
20
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
10
0
10
0
20
30
40
lschemia [min]
ADP [nmol/mg]
60
50
Ph [nmollmg]
20
120
1
T
100*
15+
80
10-
60
1
5'
40
20
0
i
0
10
i
g
20
.
30
40
50
60
lschemia [min]
0 1
0
1
1
1
14
10
20
30
40
lschemia [min]
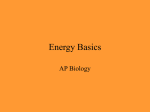
FIG 1. Graphs showing total tissue metabolite content of phosphocreatine (CrP), creatine (Cr), ATP, ADP, and inorganic phosphate (Ph)
obtained from guinea pig hearts monitored over a 60-minute period of ischemia. The amount of metabolites was determined before
submitting myocardial tissue to nonaqueous fractionation. Time zero represents the mean value of control animals (n=7) at 30 minutes
of working heart preparation before ischemia is started. All other points indicate the mean±SEM of test animals; for each ischemic
period, three test animals were used.
levels rose nearly threefold from 2.1+0.2 to 5.1+0.9
mmol/L (P<.001), as compared with normal mitochondrial ADP concentrations. In contrast to the sudden
increase of mitochondrial ADP, a moderate and advanced elevation of ADP from 1.3+0.2 to 1.9+0.1
mmol/L (P<.01) was observed after 5 minutes in the
cytosolic compartment. These findings might indicate
that during early ischemia, ADP molecules generated
within the cytosol are transported to the mitochondrial
space, resulting in an accumulation of ADP in
mitochondria.
During the breakdown of high-energy phosphates,
especially of CP and ATP, the total inorganic phosphate
pool increased rapidly within 60 minutes of ischemia,
reaching more than fourfold preischemic levels (Fig 1).
The subcellular amount of inorganic phosphate
changed during the first 5 minutes from 11.6±1.1
mmol/L in mitochondria and 7.3+ 1.0 mmol/L in cytosol
to 33.6±+1.2 and 20.5± 1.7 mmol/L (P<.01), respectively,
and remained nearly constant for a further 55 minutes.
Thus, phosphate molecules are able to reach the inside
of the mitochondrial space during short times of oxygen
depletion. Table 1 lists the subcellular metabolite concentrations for the cytosolic and mitochondrial compartment over a 60-minute period of ischemia.
Since most of the ADP molecules in myocardial
muscle are bound to proteins, the free ADP concentration cannot be estimated from the total ADP content of
the tissue. It has to be calculated from the pH- and
Mg 2+-dependent mass action ratio of the creatine kinase reaction (KCPK) as mentioned above. For this
reason, 31P NMR spectroscopy was used to obtain the
alterations of pHi and free Mg 2+ concentration during
ischemia. pHi revealed a significant decline from
7.12+0.02 to 6.81±0.03 within the first 5 minutes,
reaching a value of 6.07+0.07 after 30 minutes of
ischemia. The intracellular free Mg2+ concentration
was adversely affected. A slight increase from 0.34±0.03
to 0.49±0.07 mmol/L after a period of 5 minutes and a
further increase to 1.68+±0.24 mmol/L after 30 minutes
of ischemia were monitored. Since it was not possible to
detect a and /8 resonances of ATP after a full hour of
Rauch et al High-Energy Phosphates and Myocardial Ischemia
765
2000
7,0
-
1500
-
f
:.6.5
11000 -
-
500-
6,0
-
A
0
5
10
15
20
25
30
0
5
minus
10
15
A
A
20
25
a~~~~~~~~~
30
minuts
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
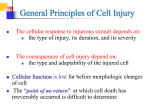
FIG 2. Graphs showing the effect of global ischemia on pH, and free Mg 2+ concentration. Data are from 31P nuclear magnetic resonance
measurements derived from five guinea pig hearts subjected to a 30-minute period of ischemia. pH was estimated from the chemical
shift of the resonance of inorganic intracellular phosphate relative to creatine phosphate. Free Mg 2+ concentration was calculated from
the shift difference between a and ,B resonances of ATP. Values are mean+SEM.
ischemia, the determination of the intracellular free
Mg 2+ was limited to the first 30 minutes. Fig 2 demonstrates the time course of pHi and free Mg 2+ concentrations during ischemia. In addition, the creatine kinase equilibrium constant and cytosolic free ATP-toADP ratio were recalculated for the different ischemic
periods by using the measured pH and Mg2+ values
according to Equations 6 and 7 (see above).
The changes of the ADP pool were opposite those of
ATP; the free ATP-to-ADP ratios dropped very quickly
from 178+20 in the cytosol and 4.4±0.5 in the mitochondria to 27±16 and 1.1±0.2 (P<.01), respectively,
during the first 3 minutes of ischemia. For the mitochondrial space, values near zero were reached after 20
minutes of ischemia (Table 2). Furthermore, the determination of free ATP-to-ADP allows the calculation of
the phosphorylation potential (AG) for both compartments. The cytosolic AG of 57.9+±1.0 kJ/mol ATP
obtained for control hearts diminished to 50.2±0.8
kJ/mol ATP (P<.05) within 5 minutes. Since an evaluation of the cytosolic AG value could only be obtained
for the first 5 minutes of ischemia, these calculations
were omitted for more extended ischemic periods (see
"Discussion"). The mitochondrial AG value declined
from 47.5±+1.2 to 40.0±0.8 kJ/mol ATP (P<.05) during
the first 5 minutes and dropped another 5 kJ/mol ATP
after a further 20 minutes of ischemia. Table 2 also lists
the mitochondrial-cytosolic difference of AGATP that is
TABLE 2. Subcellular ATP-to-ADP Ratios and Phosphorylation Potentials in lschemic Isolated
Perfused Guinea Pig Hearts
CytosolCytosol
ATP/ADPfree
Before ischemia
Ischemia, min
178±20
Mitochondria
Mitochondria
AG
57.9+1.0
ATP/ADP
AG
AG
4.4±0.5
47.5±1.2
10.5±1.0
9.4±0.8
3.0±0.2
45.6±0.7
82±12
55.0±0.7
9.2±0.8
1.8±0.3
43.7±0.9
52.9±0.8
45±10
9.4±0.7
1.1+0.2
41.2±0.9
27±16
50.5±0.9
10.2±0.9
40.0±0.8
0.8±0.2
50.2±0.8
25±18
...
...
...
38.6±1.9
0.5±0.3
35.7±1.1
...
0.2±0.2
...
...
0.2±0.2
35.9±1.0
...
...
...
ATP/ADPI,ee indicates the free ATP-to-ADP ratio; AG, phosphorylation potential. Values are mean±SEM.
ATP/ADP#ee and AG values were determined in the cytosol and mitochondrial space during ischemia. ATP/ADP
values were calculated from the mass action ratio of the creatine kinase reaction using Equation 6 (see text). AG
values of ATP are given in kilojoules per mole ATP. The cytosolic-mitochondrial values for AG demonstrate the
amount of the cytosolic-mitochondrial potential difference over the mitochondrial membrane, which is an important
parameter for the assessment of the activity of the ADP/ATP carrier in the inner mitochondrial membrane. Before
ischemia represents the mean value of control animals (n=7) at 30 minutes in working hearts before ischemia is
induced. All other points indicate the mean±SEM of 3 test animals subjected to ischemia.
0.5
1
3
5
10
20
30
766
Circulation Research Vol 75, No 4 October 1994
=10 kJ/mol ATP and does not change within the first 5
minutes of ischemia.
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
Discussion
Subcellular Metabolite Alterations in Ischemic
Guinea Pig Hearts
The total CP pool declined rapidly to 10% of preischemic levels within the first 3 minutes of ischemia,
whereas the breakdown of total ATP of the myocardial
tissue was much slower. After 60 minutes of ischemia,
20% of the preischemic ATP pool was still detected.
During the rapid degradation of CP, creatine was
accumulated in both cytosolic and the mitochondrial
compartments, reaching threefold normal concentrations (Table 1). The flux of creatine into the mitochondrial matrix was previously described by Altschuld et
al.37 The presence of an elevated level of mitochondrial
creatine might indicate permeability changes of the
mitochondrial membrane induced by oxygen depletion.
In addition, large amounts of inorganic phosphate
were liberated from the breakdown of CP and ATP,
leading to an approximately fourfold increase in the
inorganic phosphate concentration of both compartments. Hutter et a138 showed the rise of inorganic
phosphate in the intramitochondrial space during oxygen depletion and proposed a mitochondrial ATPinorganic phosphate. The ability of phosphate to retain
calcium within the mitochondria as calcium phosphate
precipitate3940 might affect the availability of Ca21 for
contraction.10 Therefore, both cytosolic and mitochondrial metabolism were affected by the high increase in
inorganic phosphate and creatine concentrations.
A rapid initial reduction of the mitochondrial ATP
concentration was observed during early ischemia,
whereas the cytosolic ATP concentration remained
nearly constant within the first 10 minutes. This rapid
decline of ATP and the accumulation of ADP in
mitochondria during early ischemia could be explained
by a substantially unchanged activity of the nucleotide
translocator delivering the rest of the mitochondrial
ATP to the cytosol by counterexchange with ADP after
cessation of oxidative phosphorylation. However, the
significant disappearance of mitochondrial ATP within
the first minutes of oxygen depletion might not be
mediated only by the 1:1 ATP-ADP exchange via the
adenine translocator or by simple degradation of highenergy phosphates; different mechanisms have been
postulated for the pathway of mitochondrial ATP loss,
all dependent on the property of inorganic phosphate
being an easily permeable anion. Meisner and Klingenberg41 demonstrated that a specific ATP efflux driven by
inorganic phosphate uptake occurred unidirectionally
from mitochondrial to cytosolic space by the way of the
adenine translocator without counterexchange for
ADP. Other investigators proposed an ATP-inorganic
phosphate exchanging protein.3842 However, the relevance of these mechanisms for mitochondrial ATP loss
during oxygen depletion in hearts is still unknown.
Nevertheless, the significant shift of ATP from the
mitochondrial to the cytosolic space and vice versa for
ADP and inorganic phosphate leads to marked changes
in compartmentation of high-energy phosphates, an
effect that has not yet been reported for ischemic hearts.
pH- and Mg 2+-Dependent Calculation of KCPK
During Ischemia
Since most of the cytosolic ADP is bound to the
contractile filaments of the heart muscle, free cytosolic
ADP had to be calculated from the pH- and Mg2+dependent creatine kinase reaction. The time course of
pHi and free inorganic Mg 2+ concentration was determined by 3'P NMR spectroscopy during ischemia. The
pHi revealed a significant steady decline over a 30minute period, consistent with previous reports.'243,44
The free Mg 2+ concentration was elevated from the
preischemic value of 0.34±0.03 to 1.68±0.24 mmol/L
after 30 minutes of ischemia. Murphy et a145 demonstrated a similar increase in the amount of Mg 2+ during
the first 15 minutes of oxygen depletion. Changes in pH,
may modulate the free intracellular Mg 2+ concentration, probably by affecting cytosolic Mg 2+ binding.46 In
this manner, both decreased pH and elevated Mg 2+
concentration have been proposed to affect cellular
function, especially the myocardial contractility. However, it is well known that KCPK changes as a function of
pHi and free Mg 2+ concentration.29,30 Bunger's empirical formula28 was used to recalculate KCPK in view of the
ischemic-induced changes in pH and Mg 2+ concentration. Because a valid application of this equation is
justified only for near physiological pH values, KCPK
estimation was limited to the first 5 minutes of oxygen
depletion. Thereafter, the pH dropped, critically impeding further calculations of cytosolic free ATP-to-ADP
ratios and phosphorylation potentials. Furthermore, it
must be assumed that the mitochondrial creatine kinase
operates far from its equilibrium, especially under normal conditions of oxygen supply and energy demand.47
However, Saks et a148 demonstrated that the mass action
ratio of creatine kinase approached its equilibrium
value within seconds when oxidative phosphorylation
was inhibited. If this is the case, then usual equilibrium
calculations can be performed at least from 30 seconds
of ischemia on, whereas they might be erroneous in
nonischemic hearts. Our data indicate that this error
probably does not play a major role. Free ATP-to-ADP
ratios and AG values in nonischemic control hearts as
calculated from the creatine kinase reaction fit well into
the expected range when the data from 30 seconds to 5
minutes of ischemia are extrapolated.
In addition, the cytosolic phosphorylation potential
of ATP was determined according to the definition of
Gibbs' free energy change49 that is also pH and Mg 2+
dependent. Derived from Alberty's contour diagrams,
changes in pH from 7.2 to 6.6 and in magnesium
concentration from 100 to 1000 gmol/L reduce the
amount of Gibbs' free energy change <6%.49 This very
small shift in AG0 was not considered to be of significance and thus not taken into account in further
calculations.
Role of the ADP/ATP Carrier During Ischemia
The nucleotide translocator yields elevated ATP-toADP ratios and phosphorylation potentials for the
cytosolic compartment and lower ratios and potentials
for the mitochondrial space. Our nonischemic control
hearts demonstrate this typical distribution of energy
state. Marked declines in the cytosolic and mitochondrial ATP-to-ADP ratio and AGATP were obtained dur-
Rauch et al High-Energy Phosphates and Myocardial Ischemia
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
ing early ischemia as shown in Table 2. The rapid
decrease in the free ATP-to-ADP ratio and phosphorylation potential has previously been reported by Kammermeier and colleagues1450 and Gibbs,47 who suggested that free energy change of ATP hydrolysis rather
than ATP depletion seemed to account for myocardial
dysfunction during early hypoxic failure. Thereby, a
steep diminution of contractile performance was obtained after the free energy change was reduced to a
critical point of =80% normal energy levels. Our investigation supports the implication that changes in the
contractile function are far more related to the rapid
decline in the phosphorylation potential than to the
availability of ATP itself.
The mitochondrial-cytosolic difference of AGATp reflects the activity of the ADP/ATP carrier.51 Our results
do not reveal a significant change of the cytosolicmitochondrial difference of AGATP (/AGC)t-Mito) within the
first 5 minutes of ischemia (AGc,tmito 10.5-+±1.0 kJ/mol
ATP before ischemia and AGcytmito=10.2+±0.9 kJ/mol
ATP after 5 minutes of ischemia). Cytosolic and mitochondrial AGATP values were reduced in parallel. Obviously, the capacity of the nucleotide transfer is high
enough to guarantee sufficient transmembrane nucleotide transport, at least during early ischemia.
Several authors suggested that large increases of fatty
acyl coenzyme A esters, occurring in O2-deficient hearts
during nucleotide decline, lead to an inhibition of the
ADP/ATP carrier.38,52,53 The binding of fatty acyl coenzyme A esters to the nucleotide translocase was speculated to contribute to the transition from reversible to
irreversible ischemic damage.54 But most of these investigations were in vitro studies on isolated mitochondria
taken from rat hearts after advanced periods of ischemia. High contents of fatty acyl coenzyme A are not
necessarily consistent with a decrease in the function of
the ADP/ATP carrier.55 Also in agreement with our
findings were the results of Asimakis and Conti,56 who
pointed out that the dysfunction associated with myocardial ischemia cannot be attributed to a decline in the
adenine nucleotide translocase activity and that a loss of
adenine nucleotides from the mitochondrial matrix
space did not affect the integrity and the function of the
translocator protein.
In summary, it cannot be excluded that advanced
ischemia may affect the activity of the ADP/ATP carrier. During early periods of ischemia, however, a
sufficient nucleotide exchange was observed. Thus, a
disturbance in nucleotide transport mechanism caused
by the ADP/ATP carrier does not account for early
contractile dysfunction.
Early Contractile Failure
Although a marked decrease in ATP content was
recorded for the mitochondrial space during the first
minute, this decline cannot be responsible for the
contractile failure of the myocardium due to the high
cytosolic ATP concentration. Under normal energy
conditions, ATP is used in the cytosolic compartment by
contractile proteins that are involved in the forcegenerating processes. Thereby, only a relatively small
ATP concentration is required to saturate the substrate
binding sites of the energy-consuming proteins.57 Furthermore, lack of ATP as substrate for the contractile
proteins would be associated with rigor of the myo-
cytoso
energy
utilization
ZATP* Cr
outer
Inner
mitochondrial mlitochondrial
membrane
rmembrane
ATPe
-'
Cr
ATP
P1
CrP
ap-----
matrix
ATPI
L
767
A
oxidative
AADPI
phwylatlon
phoa-
Cr
ADPA
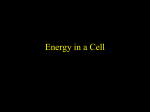
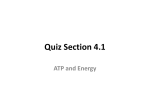
FIG 3. Diagram showing creatine (Cr)-phosphocreatine (CrP)
shuttle, an important energy transfer system in the myocardial
cell. Pi indicates inorganic phosphate; Ck, creatine kinase; myo,
myocardial; ANT, adenine nucleotide translocase (ADP/ATP
carrier); and e and i, extracellular and intracellular, respectively.
fibrils. Koretsune and Marban58 recently demonstrated
that the initiation of rigor contracture correlates closely
with the fall in ATP concentration to <10% of control
levels such that prolonged periods of oxygen depletion
are required to obtain such a pronounced ATP decrease
below the rigor threshold. Nevertheless, a decrease in
myocardial contractility can be observed during the first
few seconds and minutes of ischemia before rigor
development.10 All these arguments lead to the conclusion that the mechanism of early contractile failure
cannot be explained by the alteration in ATP content
during oxygen depletion.
Accordingly, a significant decrease of CP was monitored within the first 30 seconds of ischemia. Thus, it
seems more likely that the rapid decline in CP concentration, as observed here and elsewhere,44 may correlate
with early contractile failure. Schaefer et a159 recently
showed that changes in the CP-to-PO4- ratio are closely
associated with alterations in myocardial function during graded regional ischemia. Although a parallel diminution of CP content and contractile force can be
demonstrated, this relation does not necessarily imply
causality. CP declines as quickly as inorganic phosphate
and protons accumulate. Thus, a possible effect on
myocardial function induced by P04- and H' accumulation may also contribute to early contractile failure.
CP Shuttle
Whereas the CP content was rapidly used for energydemanding processes, no significant reduction of cytosolic ATP concentration was found during the first 10
minutes of ischemia, although CP was no longer available. A disturbance in ATP utilization during ischemia
can be proposed to explain these observations. The CP
shuttle represents the relation between CP and ATP,
and this must be taken into account.
Fig 3 shows a scheme of the PC shuttle. Energyproducing and energy-utilizing processes are linked by
this shuttle mechanism, in which CP mediates the
transfer of energy from mitochondria to cytosolic myofibrils. ATP, under normal oxygen supply produced in
the mitochondrial matrix via oxidative phosphorylation,
is delivered by the ADP/ATP carrier from the mitochondrial to the cytosolic space, where it is available for
the rephosphorylation of creatine to CP via mitochondrial creatine kinase. CP diffuses through the cytosolic
compartment to the contractile filaments, where it is
converted back to creatine by the cytosolic creatine
768
Circulation Research Vol 75, No 4 October 1994
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
kinase isoenzyme, thereby regenerating ATP, which is
then hydrolyzed by the contractile protein ATPase to
induce contraction. Normally, the rate of mitochondrial
ATP synthesis is greatly increased when ADP is generated via mitochondrial creatine kinase and is delivered
by the ADP/ATP carrier to the mitochondrial space for
rephosphorylation,60,61 supporting a functional coupling
between mitochondrial creatine kinase and the ADP/
ATP carrier. However, it is necessary that the creatine
kinase remain at the inner mitochondrial membrane for
efficient coupling, since detachment of this enzyme
completely destroys its functional relation to the ADP/
ATP carrier.61
Our investigation revealed a rapid decrease of CP,
although a sufficient activity of the ADP/ATP carrier
was observed during early ischemia. Assuming the
hypothesis that ATP, transported by the carrier from
the mitochondrial to the cytosolic space, was not used by
mitochondrial creatine kinase for CP generation, we
could explain the rapid initial reduction of CP and the
high levels of cytosolic ATP as results of an uncoupling
between mitochondrial creatine kinase and the ADP/
ATP carrier. However, the present study does not
directly provide evidence for a functional uncoupling.
This would accelerate the rapid decline in the PC
availability at the myofibrils, which may represent an
additional mechanism affecting the contractile function
in ischemic myocardium, thus strengthening the role of
the PC shuttle as an important energy transfer mechanism in the cardiac muscle. It was previously suggested
that disturbances associated with oxygen depletion affect the functional relations of creatine kinase and the
ADP/ATP carrier at the mitochondrial level.62 Furthermore, evidence was given by Vial et a163 that the
mitochondrial creatine kinase can dissociate from or
reassociate with the mitochondrial membrane depending on the height of the intracellular phosphate concentration and the decrease in pH. Such a rapid decline in
pH and a fourfold increase in inorganic phosphate
could be demonstrated for ischemic guinea pig hearts.
In conclusion, our results indicate a disturbance of
ATP utilization in the cytosolic compartment that may
play a role in the impairment of mechanical performance in ischemia. The function of the ADP/ATP
carrier per se seems not to be altered during the first 5
minutes of ischemia. However, the rapid decrease of
cytosolic CP on one hand and the only slight loss of
cytosolic ATP on the other suggests that during myocardial ischemia the functional coupling between the
ADP/ATP carrier and phosphocreatine kinase is altered. An imbalance between the PC shuttle and the
ADP/ATP carrier might reduce the PC supply during
early ischemia. This could be a substantial contribution
for the processes leading to early ischemic contractile
failure.
Acknowledgment
This study was supported by the Deutsche Forschunsgemeinschaft.
References
1. Jennings RB, Steenbergen C. Nucleotide metabolism and cellular
damage in myocardial ischemia. Annu Rev Physiol. 1985;47:
727-749.
2. Allen DG, Orchard CH. Myocardial contractile function during
ischemia and hypoxia. Circ Res. 1987;60:153-168.
3. Kuretsune Y, Corretti MC, Kusuoka H, Marban E. Mechanism of
early ischemic contractile failure: inexcitability, metabolite accumulation, or vascular collapse? Circ Res. 1991;68:255-262.
4. McFalls EO, Pantely GA, Anselone CG, Bristow DJ. Importance
of vasomotor tone to myocardial function and regional metabolism
during constant flow ischaemia in swine. Cardiovasc Res. 1990;24:
813-820.
5. Arnold G, Kosche F, Miessner E, Neitzert A, Locher W. The
importance of the perfusion pressure in the coronary arteries for
the contractility and the oxygen consumption of the heart. Pflugers
Arch. 1968;299:339-356.
6. Carmeliet E. Cardiac transmembrane potentials and metabolism.
Circ Res. 1978;42:577-587.
7. Noma A. ATP regulated K' channels in cardiac muscle. Nature.
1983;305:147-148.
8. Stern MD, Silverman HS, Houser SR, Josephson RA, Capogrossi
MC, Nichols CG, Ledere WJ, Lakatta EG. Anoxic contractile
failure in rat heart myocytes is caused by failure of intracellular
calcium release due to alteration of the action potential. Proc Natl
Acad Sci USA. 1988;85:6954-6958.
9. Zhu Y, Nosek TM. Intracellular milieu changes associated with
hypoxia impair sarcoplasmic reticulum Ca 2+ transport in cardiac
muscle. Am J Physiol. 1991;261:H620-H626.
10. Kubler W, Katz AM. Mechanism of early "pump" failure of the
ischemic heart: possible role of adenosine triphosphate depletion
and inorganic phosphate accumulation. Am J Cardiol. 1977;40:
467-471.
11. Kusuoka H, Weisfeldt ML, Zweier JL, Jacobus WE, Marban E.
Mechanism of early contractile failure during hypoxia in intact
ferret heart: evidence for modulation of maximal Ca2+-activated
force by inorganic phosphate. Circ Res. 1986;59:270-282.
12. Dennis SC, Gevers W, Opie LH. Protons in ischemia: where do
they come from; where do they go to? J Mol Cell Cardiol. 1991;23:
1077-1086.
13. Jennings RB, Reimer KA, Hill ML, Mayer SE. Total ischemia in
dog hearts, in vitro, 1: comparison of high energy phosphate production, utilization, and depletion, and of adenine nucleotide
catabolism in total ischemia in vitro vs. severe ischemia in vivo. Circ
Res. 1981;49:892-900.
14. Kammermeier H, Schmidt P, Jungling E. Free energy change of
ATP-hydrolysis: a causal factor of early hypoxic failure of the
myocardium? J Mol Cell Cardiol. 1982;14:267-277.
15. Neely JR, Rovetto MJ, Whitmer JT, Morgan HE. Effects of
ischaemia on function and metabolism of the isolated working rat
heart. Am J Physiol. 1982;225:651-658.
16. Greenfield RA, Swain JL. Disruption of myofibrillar energy use:
dual mechanisms that may contribute to postischemic dysfunction
in stunned myocardium. Circ Res. 1987;60:283-289.
17. Witzenbichler B, Rauch U, Schultheiss HP. Alteration of the
cytosolic-mitochondrial distribution of high-energy phosphates
during global myocardial ischemia in isolated perfused guinea pig
hearts. Circulation. 1992;86(suppl I):I-827. Abstract.
18. La Noue KF, Watts JA, Koch CD. Adenine nucleotide transport
during cardiac ischemia. Am J Physiol. 1981;241(Heart Circ Physiol
5):H663-H671.
19. De Leiris J, Harding DP, Pestre S. The isolated perfused rat heart:
a model for studying myocardial hypoxia or ischaemia. Basic Res
Cardiol. 1984;79:313-321.
20. Becker BF, Gerlach E. Acute effects of nicotine on hemodynamic
and metabolic parameters of isolated, perfused hearts of guinea
pigs and rats. Klin Wochenschr. 1984;62(suppl 2):58-66.
21. Bunger R, Sommer 0, Walter G, Stiegler H, Gerlach E. Functional
and metabolic features of an isolated perfused guinea pig heart
performing pressure-volume work. Pflugers Arch. 1979;380:
259-266.
22. Bunger R, Haddy FJ, Querengaesser A, Gerlach E. An isolated
guinea pig heart preparation with in vivo like features. Pflugers
Arch. 1975;353:317-326.
23. Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with the Folin phenol reagent. J Biol Chem. 1951;193:
265-275.
24. Bergmeyer HU. Methoden der Enzymatischen Analyse. 2nd ed.
Weinheim, Germany: Verlag Chemie; 1970.
25. Hammer DF, Unverferth DV, Kelley RE, Harvan PA, Altschuld
RA. Extraction and measurement of myocardial nucleotides,
nucleosides and purine bases by high-performance liquid chromatography. Anal Biochem. 1988;169:300-305.
26. Juengling E, Kammermeier H. Rapid assay of adenine nucleotides
or creatine compounds in extracts of cardiac tissue by paired-ion
Rauch et al High-Energy Phosphates and Myocardial Ischemia
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
reverse-phase high-performance liquid chromatography. Anal
Biochem. 1980;102:358-361.
27. Soboll S, Bunger R. Compartmentation of adenine nucleotides in
the isolated working guinea pig heart stimulated by noradrenalin.
Hoppe Seylers Z Physiol Chem. 1981;362:125-132.
28. Bunger R, Mallet RT, Kang YH. Guinea-pig cardiac free, bound
and interstitial adenylates: energy-linked and energy-independent
adenosine release. In: Imai S, Nakazanwa M, eds. Role of
Adenosine and Adenine Nucleotides in the Biological System.
Amsterdam, Netherlands/New York, NY: Elsevier Science Publisher BV; 1991:337-353.
29. Lawson JWR, Veech RL. Effects of pH and free Mg 2+ on the Keq
of the creatine kinase reaction and other phosphate hydrolyses and
phosphate transfer reactions. J Biol Chem. 1979;254:6528- 6537.
30. van der Meer R, Akerboom TPM, Groen AK, Tager JM. Relationship between oxygen uptake of perfused rat-liver cells and the
cytosolic phosphorylation state calculated from indicator metabolites and a redetermined equilibrium constant. Eur J Biochem.
1978;84:421-428.
31. Veech RL, Lawson JWR, Cornell NW, Krebs HA. Cytosolic phosphorylation potential. J Biol Chem. 1979;254:6538-6547.
32. Guynn R, Veech RL. The equilibrium constants of the adenosine
triphosphate hydrolysis and the adenosine triphosphate-citrate
lyase reactions. J Biol Chem. 1973;248:6966-6972.
33. Moon RB, Richards JH. Determination of intracellular pH by 31P
magnetic resonance. J Biol Chem. 1973;248:7276-7278.
34. Gard JK, Kichurcha GM, Acherman JHH, Eisenberg JD, Billadello JJ, Sobel BE, Gross RW. Quantitative 31P nuclear magnetic
resonance analysis of metabolite concentrations in Langendorff
perfused rabbit hearts. Biophys J. 1985;48:803-813.
35. Gupta RK, Benovic JL, Rose ZB. The determination of the free
magnesium level in human red blood cells by 31P NMR. J Biol
Chem. 1978;253:6172-6176.
36. Mosher TJ, Williams GD, Doumen C, LaNoue KF, Smith MB.
Error in the calibration of the MgATP chemical-shift limit: effects
on the determination of free magnesium by 31P NMR spectroscopy.
Magn Reson Med. 1992;24:163-169.
37. Altschuld RA, Merola AJ, Brierly GP. The permeability of heart
mitochondria to creatine. J Mol Cell Cardiol. 1975;7:451-462.
38. Hutter JF, Alves C, Soboll S. Effects of hypoxia and fatty acids on
the distribution of metabolites in rat heart. Biochim Biophys Acta.
1990;1016:244-252.
39. Hagler HK, Schwerin L, Buja LM. Effect of different methods of
tissue preparation on mitochondrial inclusions of ischemic and
infarcted canine myocardium: transmission and analytic electroscopic study. Lab Invest. 1979;40:529-544.
40. Lehninger AL, Carafoli E, Rossi CS. Energy-linked ion
movements in mitochondrial systems. Adv Enzymol. 1967;29:
259-320.
41. Meisner H, Klingenberg M. Efflux of adenine nucleotides from rat
liver mitochondria. J Biol Chem. 1968;243:3631-3639.
42. Aprille J, Austin JL. Regulation of the mitochondrial adenine
nucleotide pool size. Arch Biochem Biophys. 1981;212:689-699.
43. Tosaki A, Braquet P. DMPO and reperfusion injury: arrhythmia,
heart function, electron spin resonance, and nuclear magnetic
resonance studies in isolated working guinea pig hearts. Am Heart
J. 1990;120:819-830.
44. Neubauer S, Hamman BL, Perry SB, Bittl JA, Ingwall JS. Velocity
of the creatine kinase reaction decreases in postischemic myocardium: a 31P-MNR magnetization transfer study of the isolated
ferret heart. Circ Res. 1988;63:1-15.
45. Murphy E, Steenbergen C, Levy LA, Raju B, London RE.
Cytosolic free magnesium levels in ischemic rat heart. J Biol Chem.
1989;264:5622-5627.
769
46. Freudenreich CC, Murphy E, Levy LA, London RE, Lieberman
M. Intracellular pH modulates cytosolic free magnesium in
cultured chicken heart cell. Am J PhysioL 1992;262:C1024-C1030.
47. Gibbs C. The cytoplasmic phosphorylation potential: its possible
role in the control of myocardial respiration and cardiac contractility. J Mol Cell Cardiol. 1985;17:727-731.
48. Saks V, Kuznetsov AV, Kupriyanov VV, Miceli MV, Jacobus WE.
Creatine kinase of rat heart mitochondria. J Biol Chem. 1985;260:
7757-7764.
49. Alberty RA. Standard Gibbs free energy, enthalpy, and entropy
changes as a function of pH and pMg for several reactions
involving adenosine phosphate. J Biol Chem. 1969;12:3290-3302.
50. Griese M, Perlitz V, Juengling E, Kammermeier H. Myocardial
performance and free energy of ATP-hydrolysis in isolated rat
hearts during graded hypoxia, reoxygenation and high Ke+perfusion. J Mol Cell Cardiol. 1988;20:1189-1201.
51. Klingenberg M. The ADP/ATP carrier in mitochondrial membranes. In: Martonosi AN, ed. The Enzymes of Biological Membranes. New York, NY/London, England: Plenum Press; 1985;4:
511-533.
52. Paude SV, Goswami T, Parvin R. Protective role of adenine
nucleotide translocase in O2-deficient hearts. Am J Physiol. 1984;
247:H25-H34.
53. Shug A, Shrago E, Bittar N, Folls JD, Koke JR. Long chain fatty
acyl CoA inhibition of adenine nucleotide translocation in the
ischemic myocardium. Am J Physiol. 1975;228:689- 692.
54. Fenvray D, Plonet J. Relationship between structure and fatty acid
metabolism in mitochondria isolated from ischemic rat hearts. Circ
Res. 1981;48:740-747.
55. Lochner A, Van Viekerk I, Kotze JCN. Mitochondrial acyl-CoA,
adenine nucleotide translocase activity and oxidative phosphorylation in myocardial ischaemia. JMol Cell Cardiol. 1981;13:991-997.
56. Asimakis GK, Conti VR. Myocardial ischemia: correlation of mitochondrial adenine nucleotide and respiratory function. J Mol Cell
Cardiol. 1984;16:439-448.
57. Katz AM. Contractile proteins of the heart. Physiol Rev. 1970;50:
63-158.
58. Koretsune Y, Marban E. Mechanism of ischemic contracture in
ferret hearts: relative roles of [Ca 2+]j elevation and ATP depletion.
Am J Physiol. 1990;258:H9-H16.
59. Schaefer S, Schwartz GG, Gober JR, Wong AK, Camacho SA,
Massie B, Weiner MW. Relationship between myocardial metabolites and contractile abnormalities during graded regional
ischemia. J Clin Invest. 1990;85:706-713.
60. Jacobus WE. Respiratory control and the integration of heart
high-energy phosphate metabolism by mitochondrial creatine
kinase. Annu Rev Physiol. 1985;47:707-725.
61. Saks VA, Vasil'eva E, Belikova YO, Kuznetsov AV, Lyapina S,
Petrova L, Perov NA. Retarded diffusion of ADP in cardiomyocytes: possible role of mitochondrial outer membrane and creatine
kinase in cellular regulation of oxidative phosphorylation. Biochim
BiophysActa. 1993;1144:134-148.
62. Toleikis AI, Kalvenas AA, Dzheia PP, Praskhiavichius AK, Iasaitis
AA. Functional changes in the mitochondrial site of adenylate
kinase and creatine kinase system of energy transport induced by
myocardial ischemia and adriablastin. Biokhimiia. 1988;53:
649-654.
63. Vial C, Font B, Goldschmidt D, Gautheron DC. Dissociation and
reassociation of creatine kinase with heart mitochondria: pH and
phosphate dependence. Biochem Biophys Res Commun. 1979;88:
1352-1359.
Alteration of the cytosolic-mitochondrial distribution of high-energy phosphates during
global myocardial ischemia may contribute to early contractile failure.
U Rauch, K Schulze, B Witzenbichler and H P Schultheiss
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
Circ Res. 1994;75:760-769
doi: 10.1161/01.RES.75.4.760
Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1994 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7330. Online ISSN: 1524-4571
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circres.ahajournals.org/content/75/4/760
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further information
about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation Research is online at:
http://circres.ahajournals.org//subscriptions/