Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
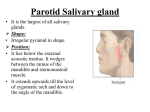
630 CHAPTER 11 The Head and Neck TA B L E 1 1 . 9 Muscles of the Soft Palate Muscle Origin Insertion Nerve Supply Action Tensor veli palatini Spine of sphenoid, auditory tube With muscle of other side, forms palatine aponeurosis Nerve to medial pterygoid from mandibular nerve Tenses soft palate Levator veli palatini Petrous part of temporal bone, auditory tube Palatine aponeurosis Pharyngeal plexus Raises soft palate Palatoglossus Palatine aponeurosis Side of tongue Pharyngeal plexus Pulls root of tongue upward and backward, narrows oropharyngeal isthmus Palatopharyngeus Palatine aponeurosis Posterior border of thyroid cartilage Pharyngeal plexus Elevates wall of pharynx, pulls palatopharyngeal folds medially Musculus uvulae Posterior border of hard palate Mucous membrane of uvula Pharyngeal plexus Elevates uvula The Salivary Glands Parotid Gland The parotid gland is the largest salivary gland and is composed mostly of serous acini. It lies in a deep hollow below the external auditory meatus, behind the ramus of the nasal septum mandible (Fig. 11.85), and in front of the sternocleidomastoid muscle. The facial nerve divides the gland into superficial and deep lobes. The parotid duct emerges from the anterior border of the gland and passes forward over the lateral surface of the masseter. It enters the vestibule of the mouth upon a small papilla opposite the upper second molar tooth (Fig. 11.72). superior concha middle concha inferior concha communication between nasal and mouth cavities palatal process of maxilla mouth cavity mouth cavity tongue 1 2 3 palatal process of maxilla A primary palate palatal processes of the maxilla 1 primary palate primary palate incisive foramen future hard palate 2 nasal septum B nasal cavity nasal cavity formation of secondary palate 3 4 soft palate uvula FIGURE 11.82 A. The formation of the palate and the nasal septum (coronal section). B. The different stages in the formation of the palate. Basic Anatomy 631 C L I N I C A L N O T E S Parotid Duct Injury A B The parotid duct, which is a comparatively superficial structure on the face, may be damaged in injuries to the face or may be inadvertently cut during surgical operations on the face. The duct is about 2 in. (5 cm) long and passes forward across the masseter about a fingerbreadth below the zygomatic arch. It then pierces the buccinator muscle to enter the mouth opposite the upper second molar tooth. C L I N I C A L C D N O T E S Parotid Salivary Gland and Lesions of the Facial Nerve The parotid salivary gland consists essentially of superficial and deep parts, and the important facial nerve lies in the interval between these parts. A benign parotid neoplasm rarely, if ever, causes facial palsy. A malignant tumor of the parotid is usually highly invasive and quickly involves the facial nerve, causing unilateral facial paralysis. Parotid Gland Infections E FIGURE 11.83 Different forms of cleft palate: cleft uvula (A), cleft soft and hard palate (B), total unilateral cleft palate and cleft lip (C), total bilateral cleft palate and cleft lip (D), and bilateral cleft lip and jaw (E). Nerve Supply Parasympathetic secretomotor supply arises from the glossopharyngeal nerve. The nerves reach the gland via the tympanic branch, the lesser petrosal nerve, the otic ganglion, and the auriculotemporal nerve. The parotid gland may become acutely inflamed as a result of retrograde bacterial infection from the mouth via the parotid duct. The gland may also become infected via the bloodstream, as in mumps. In both cases, the gland is swollen; it is painful because the fascial capsule derived from the investing layer of deep cervical fascia is strong and limits the swelling of the gland. The swollen glenoid process, which extends medially behind the temporomandibular joint, is responsible for the pain experienced in acute parotitis when eating. Frey’s Syndrome Frey’s syndrome is an interesting complication that sometimes develops after penetrating wounds of the parotid gland. When the patient eats, beads of perspiration appear on the skin covering the parotid. This condition is caused by damage to the auriculotemporal and great auricular nerves. During the process of healing, the parasympathetic secretomotor fibers in the auriculotemporal nerve grow out and join the distal end of the great auricular nerve. Eventually, these fibers reach the sweat glands in the facial skin. By this means, a stimulus intended for saliva production produces sweat secretion instead. Submandibular Gland FIGURE 11.84 Cleft hard and soft palate. (Courtesy of R. Chase.) The submandibular gland consists of a mixture of serous and mucous acini. It lies beneath the lower border of the body of the mandible (Fig. 11.86) and is divided into superficial and deep parts by the mylohyoid muscle. The deep part of the gland lies beneath the mucous membrane of the mouth on the side of the tongue. The submandibular 632 CHAPTER 11 The Head and Neck temporalis zygomatic arch superficial parotid gland temporal vein accessory part of parotid gland posterior parotid duct auricular vein external jugular vein orbicularis oris angle of mandible buccinator sternocleidomastoid masseter A superior constrictor of pharynx carotid sheath vagus nerve internal carotid artery internal jugular vein styloglossus auriculotemporal nerve glossopharyngeal nerve accessory nerve fascial capsule fibrous capsule stylomandibular ligament hypoglossal nerve stylopharyngeus styloid process stylohyoid division of external carotid artery posterior auricular artery posterior belly of digastric medial pterygoid formation of retromandibular vein mastoid process ramus of mandible masseter skin deep part of parotid gland facial nerve sternocleidomastoid parotid lymph nodes B great auricular nerve superficial part of parotid gland FIGURE 11.85 Parotid gland and its relations. A. Lateral surface of the gland and the course of the parotid duct. B. Horizontal section of the parotid gland. Basic Anatomy 633 deep part of submandibular gland tongue submandibular duct stylohyoid opening of submandibular duct central incisor tooth sublingual gland mylohyoid posterior belly of digastric body of mandible anterior belly of digastric A super ficial part of submandibular gland fibrous band mouth cavity styloglossus hyoid bone muscles of tongue fibrous septum vestibule genioglossus geniohyoid deep part of submandibular gland mylohyoid mylohyoid super ficial part of submandibular gland anterior belly of digastric submandibular duct inferior alveolar nerve B buccinator C sublingual gland FIGURE 11.86 A. Submandibular and sublingual salivary glands (lateral view). B. Coronal section through the superficial and deep parts of the submandibular salivary glands. C. Coronal section (anterior to B) through the sublingual salivary glands and the ducts of the submandibular salivary glands. duct emerges from the anterior end of the deep part of the gland and runs forward beneath the mucous membrane of the mouth. It opens into the mouth on a small papilla, which is situated at the side of the frenulum of the tongue (Fig. 11.72). Nerve Supply Parasympathetic secretomotor supply is from the facial nerve via the chorda tympani, and the submandibular ganglion. The postganglionic fibers pass directly to the gland. C L I N I C A L N O T E S Submandibular Salivary Gland: Calculus Formation The submandibular salivary gland is a common site of calculus formation. This condition is rare in the other salivary glands. The presence of a tense swelling below the body of the mandible, which is greatest before or during a meal and is reduced in size or absent between meals, is diagnostic of the condition. Examination of the floor of the mouth will reveal (continued) 634 CHAPTER 11 The Head and Neck absence of ejection of saliva from the orifice of the duct of the affected gland. Frequently, the stone can be palpated in the duct, which lies below the mucous membrane of the floor of the mouth. Enlargement of the Submandibular Lymph Nodes and Swelling of the Submandibular Salivary Gland The submandibular lymph nodes are commonly enlarged as a result of a pathologic condition of the scalp, face, maxillary sinus, or mouth cavity. One of the most common causes of painful enlargement of these nodes is acute infection of the teeth. Enlargement of these nodes should not be confused with pathologic swelling of the submandibular salivary gland. nasal part of pharynx oral part of pharynx laryngeal part of pharynx Sublingual Gland The sublingual gland lies beneath the mucous membrane (sublingual fold) of the floor of the mouth, close to the frenulum of the tongue (Fig. 11.86). It has both serous and mucous acini, with the latter predominating. The sublingual ducts (8 to 20 in number) open into the mouth on the summit of the sublingual fold (Fig. 11.72). Nerve Supply Parasympathetic secretomotor supply is from the facial nerve via the chorda tympani, and the submandibular ganglion. Postganglionic fibers pass directly to the gland. C L I N I C A L N O T E S Sublingual Salivary Gland and Cyst Formation The sublingual salivary gland, which lies beneath the sublingual fold of the floor of the mouth, opens into the mouth by numerous small ducts. Blockage of one of these ducts is believed to be the cause of cysts under the tongue. The Pharynx The pharynx is situated behind the nasal cavities, the mouth, and the larynx (Fig. 11.87) and may be divided into nasal, oral, and laryngeal parts. The pharynx is funnel shaped, its upper, wider end lying under the skull and its lower, narrow end becoming continuous with the esophagus opposite the 6th cervical vertebra. The pharynx has a musculomembranous wall, which is deficient anteriorly. Here, it is replaced by the posterior openings into the nose (choanae), the opening into the mouth, and the inlet of the larynx. By means of the auditory tube, the mucous membrane is also continuous with that of the tympanic cavity. Muscles of the Pharynx The muscles in the wall of the pharynx consist of the superior, middle, and inferior constrictor muscles (Fig. 11.80A), whose fibers run in a somewhat circular FIGURE 11.87 Sagittal section through the nose, mouth, pharynx, and larynx to show the subdivisions of the pharynx. direction, and the stylopharyngeus and salpingopharyngeus muscles, whose fibers run in a somewhat longitudinal direction. The three constrictor muscles extend around the pharyngeal wall to be inserted into a fibrous band or raphe that extends from the pharyngeal tubercle on the basilar part of the occipital bone of the skull down to the esophagus. The three constrictor muscles overlap each other so that the middle constrictor lies on the outside of the lower part of the superior constrictor and the inferior constrictor lies outside the lower part of the middle constrictor (Fig. 11.88). The lower part of the inferior constrictor, which arises from the cricoid cartilage, is called the cricopharyngeus muscle (Fig. 11.88). The fibers of the cricopharyngeus pass horizontally around the lowest and narrowest part of the pharynx and act as a sphincter. Killian’s dehiscence is the area on the posterior pharyngeal wall between the upper propulsive part of the inferior constrictor and the lower sphincteric part, the cricopharyngeus. The details of the origins, insertions, nerve supply, and actions of the pharyngeal muscles are summarized in Table 11.10. Interior of the Pharynx The pharynx is divided into three parts: the nasal pharynx, the oral pharynx, and the laryngeal pharynx. Nasal Pharynx This lies above the soft palate and behind the nasal cavities (Fig. 11.87). In the submucosa of the roof is a collection of lymphoid tissue called the pharyngeal tonsil (Fig. 11.89). The pharyngeal isthmus is the opening in the floor between the soft palate and the posterior pharyngeal wall. On the lateral wall is the opening of the auditory tube, the elevated ridge of which is called the tubal elevation (Fig. 11.89).