Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
British Journal of Anaesthesia 1993; 71: 814-817
ORAL BROMFENAC 10 AND 25 MG COMPARED WITH
SUBLINGUAL BUPRENORPHINE 0.2 AND 0.4 MG FOR
POSTOPERATIVE PAIN RELIEF
D. CARROLL, T. FRANKLAND, C. NAGLE AND H. McQUAY
SUMMARY
The aim of this single-dose, randomized, positive
control, double-dummy,
double-blind, parallel
group study was to compare oral bromfenac 10 and
25 mg with sublingual buprenorphine 0.2 and
0.4 mg for treatment of postoperative pain. We
studied 91 patients with moderate or severe pain
after general surgical or orthopaedic operations,
using pain intensity, pain relief, adverse effect,
mood and sedation outcomes. There was a significant analgesic dose-response for buprenorphine, showing study sensitivity, but not for
bromfenac. The two bromfenac treatments were
significantly superior to the two buprenorphine
treatments. Significantly more patients reported
nausea with buprenorphine. There was evidence of
a ceiling effect for analgesia with bromfenac. (Br. J.
Anaesth. 1993; 7 1 : 814^817)
KEY WORDS
Analgesics, non-opioid: bromfenac. Analgesics, opioid: buprenorphine. Pain: postoperative.
The precise roles of the two drug classes, opioids and
non-steroidal anti-inflammatory drugs (NSAID), in
the management of postoperative pain remain contentious. For many years opioids were the only
injectable analgesics available, but the introduction
of injectable NSAID has encouraged wider use of
NSAID immediately after surgery. Oral opioids
have a poor reputation for postoperative pain control
[1], but there is strong evidence from randomized
controlled trials for the effectiveness of oral NSAID
in treating postoperative pain [2, 3].
The evidence from single-dose randomized controlled trials suggests that injectable NSAID can
provide analgesia indistinguishable from that obtained with injected opioids [4], and that oral
NSAID can also match the effect of an injected
opioid [5]. However, a ceiling effect has been
demonstrated for NSAID analgesic effect [5, 6] by
both oral [6] and injected routes [7].
This study was designed to compare oral
bromfenac, a new 2-amino-3-benzoylphenylacetic
acid derivative NSAID, with an opioid, sublingual
buprenorphine, for the treatment of postoperative
pain.
Bromfenac has anti-inflammatory, antipyretic and
analgesic properties. In a previous study of pain after
dental extraction, bromfenac in doses of 5, 25 and
50 mg was significantly better than placebo and the
25- and 50-mg doses were also significantly superior
to aspirin 650 mg [8]. Bromfenac 5, 10 and 25 mg
was also compared with paracetamol 1 g and placebo
for pain relief after orthopaedic surgery; the 5-mg
dose of bromfenac was superior to placebo and the
10-mg dose was equivalent to paracetamol 1 g [2].
PATIENTS AND METHODS
This was a double-blind, double-dummy, parallel
group, single-dose study, comparing oral bromfenac
10 or 25 mg with sublingual buprenorphine 0.2 or
0.4 mg. It was approved by the Central Oxford
Research Ethics Committee. Men and women were
eligible for the study if they were to undergo
orthopaedic or general surgery. Patients were excluded if they had a history of peptic ulcer disease,
hepatic or renal disease, intolerance to aspirin,
buprenorphine or NSAID, respiratory disease sufficient to contraindicate the use of buprenorphine, or
if they were taking coumarin-type anticoagulants or
oral hypoglycaemic agents. Women were excluded if
they were pregnant or breast feeding.
Patients experiencing moderate or severe pain
(verbal rating scale) within 72 h of surgery were
included if they had recovered sufficiently from
surgery, were capable of taking oral medication, and
if more than 3 h had elapsed since they had received
any analgesic, tranquillizing or sedative drug. They
were allocated to one of four groups: sublingual
buprenorphine 0.2 mg (one buprenorphine 0.2 mg
tablet, one placebo sublingual tablet and one placebo
oral capsule); sublingual buprenorphine 0.4 mg (two
buprenorphine 0.2 mg tablets and one placebo oral
capsule); oral bromfenac 10 mg (two placebo sublingual tablets and one bromfenac 10 mg capsule);
oral bromfenac 25 mg (two placebo sublingual
tablets and one bromfenac 25 mg capsule).
Tablets and capsules were identifiable only by
treatment number. Randomization was stratified at
entry by initial pain intensity ("moderate" or
DAWN CARROLL, R.G.N.; THERESA FRANKLAND, R.G.N.; CHRIS
NAGLE, M.B., B.CH., F.R.C.A.; HENRY M C Q U A Y * , D.M., F.R.C.A.J
Oxford Regional Pain Relief Unit, Churchill Hospital, Oxford &
Nuffield Department of Anaesthetics, University of Oxford,
Oxford. Accepted for Publication: June 7,1993.
*Address for correspondence: Oxford Regional Pain Relief
Unit, Churchill Hospital, Oxford OX3 7LJ.
POSTOPERATIVE BROMFENAC AND BUPRENORPHINE
"severe") and by type of surgery (general or
orthopaedic). Randomization was in blocks of four,
organized by random number generation.
A nurse observer administered all the study
treatments. The oral capsule was given first and
swallowed with water 100 ml, which was followed
immediately by the two sublingual tablets, which
were allowed to dissolve under the tongue. Patients
were then assessed for up to 6 h after receiving the
study treatment. If pain relief was inadequate after
the first 1 h, patients were free to request further
analgesia and standard postoperative analgesia was
given.
Baseline assessments of patients were made for
pain intensity, vital signs, mood and sedation. All
assessments were made by one nurse observer (T.F.).
Patients were reassessed at 0.5, 1, 1.5, 2, 3, 4, 5 and
6 h. Pain intensity, vital signs, mood and sedation
assessments were repeated, together with assessments for pain relief and adverse effects. At the end
of the 6-h study period, or at the time of remedication, an overall rating of the treatment was made by
the nurse and by the patient.
Current pain intensity was measured by a categorical verbal rating scale (0 = none; 1 = mild; 2 =
moderate; 3 = severe) using the question "how
intense is the pain at the moment?"; by an eightword scale (randomly placed words ranging from
"no pain" to "excruciating", scored 0-7) [9], by a
visual analogue scale (100-mm line, left end labelled
"no pain" and right end labelled "worst possible
pain") and by the McGill Pain Questionnaire using
78 descriptors in 20 groups.
Pain relief was measured by a categorical verbal
rating scale (0 = none; 1 = slight; 2 = moderate; 3
= good; 4 = complete) using the question "How
much pain relief have you got at the present time?";
and by a visual analogue scale (100-mm line, left end
labelled "no relief of pain" and right end labelled
" complete relief of pain ").
Mood was measured with a visual analogue scale
(100-mm line, left end labelled "worst I could feel"
and right end labelled "best I could feel"). Sedation
was measured by a categorical verbal rating scale (0
= alert; 1 = mildly drowsy; 2 = moderately drowsy;
3 = asleep). If patients were asleep, they were
wakened for assessments. Systemic arterial pressure,
heart rate and ventilatory frequency were measured
by the nurse observer.
At the end of the 6-h study period, or at the time
patients asked to withdraw from the study, both the
nurse observer and the patient made a global rating
of the study treatment (0 = poor; 1 = fair; 2 =
good; 3 = very good; 4 = excellent). The nurse
made her evaluation first, to avoid bias. Adverse
effects, both volunteered and observed, were
recorded, with scoring of intensity (0 = none; 1 =
mild; 2 = moderate; 3 = severe).
Statistical analysis
It was estimated that 20 patients per group would
be necessary to achieve power of 90 % with an alpha
level of 0.05 (one-tailed) to detect a difference
between the four treatments of 1.5 on the categorical
pain relief with SD of 0.3 [2].
815
Patients who were remedicated within the 6-h
study period were given initial values of pain
intensity and a pain relief score of zero for assessment
times after remedication [10]. The McGill pain
questionnaire was scored both for number of words
chosen and for sum rank score. The sum of the pain
intensity difference (four word SPID) and total pain
relief (TOTPAR) scores were calculated [11], to
produce an area under the curve of effect against
time. The same calculation was used for the visual
analogue equivalents (VASSPID for pain intensity
and VASPR for pain relief), the eight-word verbal
rating for pain intensity (WORD SPID) and the
McGill word and total scores (McGill wordSPID
and McGill scoreSPID, respectively). The overall
sedation and mood scores (AUCSEDATION and
AUCMOOD) were calculated by use of a trapezoidal
formula.
Analysis of variance was used on the scores for the
four treatments groups, and the Student's t test was
used for comparisons of pairs—one-tailed within
drug between doses and two-tailed between drug.
The incidence of adverse effects and time to
remedication were compared using the chi-square
test. All tests were performed using Statview 4 on a
Macintosh Ilci. Results are presented as mean (SEM).
RESULTS
We studied 91 patients between November 1989 and
February 1991. Three patients did not fulfil the
study design. Of these three, one was excluded from
the final analysis, because she received additional
analgesia at the 0.5-h assessment. Two were included: one developed a headache, thought to be
caused by a dural tap, and was given paracetamol;
the other inadvertently received an NSAID during
the study. Their results to the time of remedication
were included in the analysis (i.e. the same strategy
as for other patients who were remedicated during
the 6-h study period).
Details of the patients are shown in table I; there
were no significant differences between the four
groups in age, sex, height, weight or duration of
surgery (ANOVA).
Analgesic measures (table II)
There were statistically significant differences
between the four groups for all analgesic outcome
measures (ANOVA). Sublingual buprenorphine
0.4 mg gave significantly better analgesia than 0.2 mg
on all analgesic outcome measures except for the
patient and nurse global rating (one-tailed t test);
there were no significant differences between the 10and 25-mg doses of oral bromfenac (one-tailed t
test).
Bromfenac 10 mg provided significantly better
analgesia than both doses of buprenorphine on all
analgesic measures (two-tailed t test). Bromfenac
25 mg provided significantly better analgesia than
buprenorphine 0.2 mg on all measures, but was
significantly better than buprenorphine 0.4 mg only
for SPID, WORDSPID and patient global rating.
The rank order was thus buprenorphine 0.2 mg <
buprenorphine 0.4 mg < bromfenac 10 and 25 mg.
BRITISH JOURNAL OF ANAESTHESIA
816
TABLE I. Patient characteristics, and duration and nature of surgical procedure {mean (range or SEM)). No significant
difference between treatments overall (ANOVA)
Buprenorphine
0.2 mg
No. patients
Age (yr)
Sex (F:M)
Height (cm)
Weight (kg)
Surgery time (min)
Surgical procedure
Orthopaedic
General surgery
Bromfenac
10 mg
0.4 mg
25 mg
22
24
23
21
41 (18-61)
13:9
170(2)
69(2)
68(8)
38 (19-63)
12:12
170(2)
69(3)
79 (10)
43 (23-69)
16:7
168 (2)
68(3)
62(7)
43(20-65)
9:13
173(2)
75(3)
73(7)
15
7
15
7
16
7
14
7
TABLE II. Analgesic outcome measures (mean (SEM)). Significant differences: *overall between the four treatment groups
(ANOVA);
^between 0.2 and 0.4 mg buprenorphine (one-tailed t test); ^between bromfenac 10 mg and buprenorphine
0.2 mg (two-tailed t test); ^between bromfenac 10 mg and buprenorphine 0.4 mg (two-tailed t test); ^between bromfenac
25 mg and buprenorphine 0.2 mg (two-tailed x. test); \\between bromfenac 25 mg and buprenorphine 0.4 mg (two-tailed t test);
**(chi-square)
Buprenorphine
0.2 mg
No. patients
SPID
VASSPID
TOTPAR
VASTOTPAR
WORDSPID
McGill WORDSPID
McGill SCORESPID
Patient global
Nurse global
Completing study
AUCSEDATION
AUCMOOD
0.4 mg
Bromfenac
10 mg
25 mg
22
24
23
21
1.8(0.4)
41(13)
5.2 (0.8)
156(26)
2.9 (0.6)
1.3(0.7)
7.5 (3.6)
1.4(0.2)
1.2(0.2)
3.1(0 6)
92 (19)
8.5(1.2)
242 (34)
5.4(1)
6.3(1.9)
20.2 (4.6)
1.8 (0.2)
1.6 (0.3)
6.4 (0.9)
175 (24)
14.1(1.3)
386(33)
12(1.8)
13.6 (2.3)
34.7 (5.4)
2.9 (0.2)
2.5 (0.2)
5.5(1.0)
122 (29)
11(1.7)
317 (45)
10(1.9)
10.2 (2.6)
28.9 (7.9)
2.4 (0.3)
2.5 (0.2)
*tts«u
4
11
14
12
•*
2.6(1)
344 (43)
2.6 (0.8)
553 (61)
2.7 (0.8)
819 (54)
2.5(1.1)
697 (86)
*t«f
*t««
*tts§
*t««ll
*t*§fl
*+*§«
*ts*n
Bromfenac 10 mg provided significantly greater
mood scores than either dose of buprenorphine (twotailed t test) and AUCMOOD with bromfenac 25 mg
was significantly greater than with buprenorphine
0.2 mg, but not buprenorphine 0.4 mg. There was
no significant difference between the AUCMOOD
scores for bromfenac 10 and 25 mg.
There was no significant difference overall between
the
four
treatment
groups
for
AUCSEDATION.
4-
3-
2c
CD
a.
1-
Adverse effects
0
1
2
3
4
Time (h)
5
6
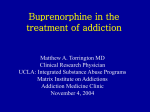
FIG. 1. Mean (SEM) pain relief against time for buprenorphine
0.2 mg (O)j buprenorphine 0.4 mg ( • ) , bromfenac 10 mg ( • )
and bromfenac 25 mg (A). Significant differences at all times after
30 min (ANOVA).
Mean categorical verbal pain relief scores against
time for the four groups reflect this rank order
(fig. 1).
Non-analgesic outcome measures
There was a significant difference overall between
the four treatment groups for AUCMOOD, with
significantly greater mood scores with buprenorphine 0.4 mg than with 0.2 mg (one-tailed t test).
More patients reported adverse effects after
buprenorphine; twice as many patients (eight) had
adverse effects with buprenorphine 0.2 mg compared
with bromfenac 25 mg. The incidence of nausea was
significantly greater with buprenorphine 0.4 mg,
with five patients affected compared with none who
received bromfenac (P < 0.02, chi-square).
Time to remedication
There was a statistically significant difference
between the treatments for the number of patients
who needed remedication before the end of the study
(P < 0.02, chi-square). Only four patients who received the smaller dose of buprenorphine completed
the 6-h study. In all but the two patients described
above, this was because of inadequate pain relief and
they were remedicated with standard analgesia.
POSTOPERATIVE BROMFENAC AND BUPRENORPHINE
DISCUSSION
The sensitivity of the study was demonstrated by
the dose-response for sublingual buprenorphine—
0.4 mg provided significantly better analgesia than
0.2 mg on all of the analgesic outcome measures
(table II). Few other randomized, controlled trials
have examined the dose-response for sublingual
buprenorphine. In one such comparison of sublingual buprenorphine 0.2, 0.4 and 0.8 mg with i.m.
morphine 4,8 and 16 mg, a significant dose-response
for sublingual buprenorphine was found, with a
potency ratio to morphine of 1:15 [12].
Oral bromfenac provided better analgesia than
sublingual buprenorphine (table II, fig. 1). Both 10and 25-mg doses of bromfenac produced significantly better analgesia than the larger dose of
buprenorphine (0.4 mg). Previous studies have suggested that oral NSAID provide better analgesia
than i.m. opioids; oral ketoprofen 75 and 225 mg was
equal to or more effective than i.m. morphine 5 and
10 mg [5]. It is perhaps less surprising, then, that
oral bromfenac 10 mg was superior to sublingual
buprenorphine 0.4 mg, and suggests that 0.8 mg
would be necessary to provide equivalent analgesia,
with an increased risk of unacceptable adverse
effects.
There was no evidence of a dose—response for
bromfenac; indeed, the analgesic scores for 10 mg
were better than those for 25 mg on most outcomes.
Such ceiling effects with NSAID have been reported
previously in single-dose analgesic studies [5];
occasionally with NSAID, a dose-response is found
for duration of analgesia, although not apparent on
peak or total (TOTPAR) analgesia during the study
period. The clinical conclusion is that in this setting
there would be no advantage in giving bromfenac
25 mg rather than 10 mg. Bromfenac, in common
with other oral NSAID, proved to be an effective
analgesic for moderate or severe postoperative pain.
The lesser incidence of adverse effects with NSAID
compared with opioids at equivalent (or better)
levels of pain relief suggests that oral NSAID should
817
be used more in the management of postoperative
pain.
ACKNOWLEDGEMENTS
This study was supported by AH Robins/Wyeth Research UK.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
REFERENCES
Hanks GW, Rose NM, Aherne GW, Piall EM. Analgesic
effect of morphine tablets. Lancet 1981; 1: 732-732.
McQuay HJ, Carroll D, Frankland T, Harvey M, Moore A.
Bromfenac, acetaminophen, and placebo in orthopedic postoperative pain. Clinical Pharmacology and Therapeutics 1990;
47: 760-766.
Hill CM, Carroll MJ, Giles AD, Pickvance N. Ibuprofen
given pre and post operatively for the relief of pain.
International Journal of Oral Maxillofacial Surgery 1987; 16:
420-424.
Buckley MM-T, Brogden RN. Ketorolac. A review of its
pharmacodynamic and pharmacokinetic properties and therapeutic potential. Drugs 1990; 39: 86-109.
Sunshine A, Olson NZ. Analgesic efficacy of ketoprofen in
postpartum, general surgery, and chronic cancer pain. Journal
of Clinical Pharmacology 1988; 28: S47-S54.
McQuay HJ, Poppleton P, Carroll D, Summerfield RJ,
Bullingham RES, Moore RA. Ketorolac and acetaminophen
for orthopedic postoperative pain. Clinical Pharmacology and
Therapeutics 1988; 39: 89-93.
O'Hara DA, Fragen RJ, Kinzer M, Pemberton D. Ketorolac
tromethamine as compared with morphine sulfate for treatment of postoperative pain. Clinical Pharmacology and
Therapeutics 1987; 41: 556-561.
Forbes JA, Beaver WT, Jones KF, Edquist IA, Gongloff
CM, Smith WK, Smith FG, Schwartz MK. Analgesic efficacy
of bromfenac, ibuprofen, and aspirin in postoperative oral
surgery pain. Clinical Pharmacology and Therapeutics 1992;
51: 343-352.
Tursky B. The development of a pain perception profile: a
psychological approach. In: Weisenberg M, Tursky B, eds.
Pain: New Perspectives in Therapy and Research. New York:
Plenum Press, 1975; 171-194.
Lasagna L. Analgesic methodology: a brief history and
commentary. Journal of Clinical Pharmacology 1980; 20:
273-276.
Wallenstein SL, Houde RW. The clinical evaluation of
analgesic effectiveness. In: Ehrenpreis S, Neidle A, eds.
Methods in Narcotics Research. New York: Marcel Dekker,
1975; 127-145.
Wallenstein SL, Kaiko RF, Rogers AG, Houde RW.
Crossover trials in clinical analgesic assays: studies of
buprenorphine and morphine. Pharmacotherapy 1986; 6:
228-235.