Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
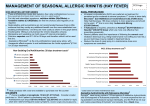
New Challenges to Old Standards in the Treatment of Rhinitis Anticholinergics Ipratropium bromide, another safe medication with few side I_"~"':I.~/ A Comparison of Selected Product Indications ef~ects, is useful in treating rhinorrhea but will not address allergic symptoms. lpratropium bromide is a quaternary amine that minimally crosses the nasal and gastrointestinal membrane, Seasonal Allergic Nonallergic Rhinitis Rhinitis reducing systemic antichoJinergic effects. 15. 16 Although it can be Clarilin V combined ,vith nasal steroids to treat rhinitis, iprmropium bromide is not very effective for vasomotor rhinitis. Allegra V Z yrtec V Astelin V V V V Flonase V V Nasacort V Nasonex V Rhinocort V Rhinocort AQ V Vancenase AQ V Decongestants Topical decongestants like pseudoephedrine are systemic medications that may alleviate nasal congestion. However, they may have adverse effects, such as loss of appetite, anxiety, nervous- ness, and insomnia. Patiellls who have an arrhythmia, angina, hypenension, or hyperthyroidism are not good candidates for these medications because they can aggravate these conditions. The Food and Drug Administration (FDA) recently issued a recall for all products cOlllaining phenylpropanolamine (PPA) due to safety concerns. Topical decongestants Jike oxymetazoJine can be effective in treating rhinitis-induced congestion but only for fewer than four days. Longer use may lead to rhinitis medicamentosa or 17 "rebound" congestion. Intranasal Corticosteroids Beconase AQ - V V Note: C!witin, Nasonex, and \lancenase are trademarks Allegra and Nasacon oj Schering-Plough. oj Aventis. Rhinocol'/ is an AstraZeneca trademarll. Bccona.le and F!onase are trademarl1s of G!cLxoSmithKline and Zyrtcc 1.1 a Beclomethasone dipropionate, budesonide, and Oucticasone are all nasal conicosteroids that have been approved for treatment of seasonal allergic rhinitis and perennial nonallergic rhinitis. W'C trademarks PJizertrademarl1. .,~...:t.:a. Target Drugs /' Their localized anti-inOammatory activity and minimal systemic absorption make them very effective. Side effects include nasal irritation and nasal bleeding. Because they are steroids, Antihistamines . . there is some .concern about growth suppression in children. Current FDA guidelines require that children younger than 12 . Antihistamines Antihistamines Nasal'Steroids Antihistamine options include either first- or second-generation oral antihistamines and a nasal antihistamine. Because first-gen- . . eration oral antihistamines, such as diphenhydramine and hydroxyzine, are considered strong sedatives, they are usually not first-line choices for most patiellls. Loratadine and fexofenadine, . . both second-generation oral antihistamines, are effective in reducing sneezing, itching, and rhinorrhea, but they have mini- Oral Solids Zyrtec (celirizine) Allegra (fexofenacline) who receive either nasal or inhaled steroids be measured regularly using a stadiometer. '" . - Claritin (loratacline) - Nasal Spray Astelin (azelasline) Nasalicle, Nasarel (nunisolicle) Beconase, Beconase AQ, Beconase AQ DS, Vancenase, Vancenase AQ (beclomethasone) Nasacort, Nasacort AQ (triamcinolone) . Rhinocorl, Rhinocort AQ (buclesonicle) . Flonase (nuticasone) . Nasonex (mometasone) mal effects on nasal congestion and postnasal drip. Therefore, they may be prescribed in combination with other medications.; Like second-generation oral antihistamines, the nasal antihistamine azelastine has an onset of action within three hours. It is the only second-generation antihistamine to be approved to treat seasonal allergic rhinitis in adults and children age 5 and over, as well as nonallergic vasomotor rhinitis in adults and children age 12 and over. It is effective in treating the symptoms of rhinitis, including Vol. 7. No.2 The most common side effects are bitter taste, headache, somnolence, and nasal burning. nasal congestion and postnasal dJip.; _ '" Evaluating Utilization Patterns Medication costs for treatment of rhinitis continue to rise, in some cases quite shaqJI)' For example, in 1998, the cost of March/April 200\ prescribed Supplement to the Journal of Managed Care Pharmacy 7 New Challenges to Old Standards in the Treatment of Rhinitis more than 25%. Similarly, the PM PY cost for intranasal steroids providers, 64%; a1lergists, 14%; ear, nose, and throat (ENT) specialists, 7%; pulmonary specialists, 2%; and other physicians, such as cardiologists, surgeons, and neurologists, 13%. jumped from $3.59 PMPY in 1998 to $4.56 PMPY in 1999."'.21 A patient analysis conducted in 2000 by Nelda Johnson and Combination Therapy antihistamines was $8.33 per health care plan member per year (PMPY). One year later, this figure rose to $10.51, an increase of technology-based Of the patients studied, 11 % were started on combination thera- information management company, was supported by Wallace laboratories to explore several managed health care prescrip- py, usually antihistamine and a nasal steroid. Drugs were sometimes added to a treatment plan after an initial single-drug start. In a1l, 39% of patients in the study used two or more classes of medications during the one year fo1low-up peIiod, perhaps as a result Omar Shoheiber of Tricore Technology, Inc., a tion-utilization and diagnostic indicators: \Vhat are the prescription patterns? What medical diagnoses are associated with prescriptions for second-generation antihistamines and nasal steroids? . . . What are the resource-utilization patterns? The retrospective database analysis used medical and pharmacy claims for three different health plans, each with a minimum of 100,000 members. One was located in the northeast, one in the north central, and one in the western part of the United States. Candidates for the study were plan members who had been continuous1y enrolled for at least 12 months with both medical and pharmacy coverage and who had received at least two of the target drugs. The target drugs are listed in Table 5 on page 7. Of a starting sample population of 44,989 patients who had received one of the drugs, 19,325 patients were se1ected who had received more than one prescription for a target drug, inclicating either a refi1l or another therapeutic option, and had been continuously enrolled in the health plan for 12 months or more. of treatment failure. Allergists were most likely to recommend combination care from the stan. Among plimaty care, allergy, ENT, and pulmonaty care physicians, a1lergists prescribed initial combination therapy 20% of the time-about twice as often as plimary care physicians. Primary care physicians favored initial antihistamine therapy, choosing one of the target antihistamines 56% of the time. Initial therapy with nasa1 steroids was the first choice of both ENT spepulmon010gists (see Table 6, below). cialists and The cost and number of prescriptions per person were greater than the study averages for the group receiving initial combination therapy: $188 PMPY, compared with the study average of $175. Similarly, the average number of prescriptions for combination therapy was 4.9 prescriptions compared to a study average of 4.5. Medical Claims Analysis The mean age of patients was 35 years; 55% were female. Examining the medical rather than phannacy claims for these 19,325 patients produced further insights. Of the qualified patients Targeted Options (those continuously enrolled for more than one year who had prescriptions for one of the target drugs) medical claims showed that on1y 40% had one of the target diagnoses. The two categories of medication included were antihistamines (oral and nasal) (62%) and nasal steroids (38%). The average number of prescriptions for all target drugs was 4.5 prescriptions PMPY, at an average annual cost of $175 per person. Diagnoses analyzed, identified by lCD-9 codes, were a11ergic rhinitis, chronic rhinitis, acute sinusitis, chronic sinusitis, acute nasopharyngitis (common cold), and other diseases of the nasa1 Among patients with a target primary diagnosis, the study authors identified some startling patterns in correlated therapies observab1e within 30 days of the diagnosis date. Pure antihistamines were prescribed 41% of the time in response to a diag- cavity and sinuses. are not indicated. Allergic rhinitis pátiems received antihista- The population was also analyzed according to the type of physician prescribing the target medication: primary care mine therapy 50% of the time, and combination therapy 29% of the time. It is unknown what proportion of the patients actual- ~"~":I~=-~ nosis of acute Initial Therapy by Physician Specialty Physician Specialty 8 sinusitis-a condition for which antihistamines Initial Therapy Nasal Steroids Antihistamines Combination Primary Care 33% 56% 11% Allergist 36% 44% 20% Ear, nose, ancllhroal CENT) 60% 30% 10% Pulmonary 53% 39% 9% Supplement to the Journal 01 Managed Care Pharmacy March/April 200 I Vol. 7, No.2 New Challenges to Old Standards in the Treatment of Rhinitis 11'had mixed or pure (with no allergic components or etiology) nonallergic rhinitis. More than 60% of patients with common colds (diagnosis: acute nasopharyngitis) were given one of the targeted antihistamines. 1I:IIIClII:I=-_ 12-Month Prescription and I / $250 Cost of Care-Medical and Pharmacological The medical claims also showed that, most of the time (59%), patients visited their primary care physicians for treatment of their rhinitis symptoms. On average the number of office visits resulting in one of the target diagnoses as a primary diagnosis was 0.6 visits per patient per year, at an average annual medical charge of $19 per patient per year (PPPY). Taking both medical and phannacy eXlJenditures into account, the greatest total cost per patient per year was associated with combination therapy at $210, followed by oral antihistamines at $202, and nasal steroids at $177 PPPY. Treatment with nasal antihistamines had the lowest cost, $131 (see Figure 1, right). The data demonstrate that allergic rhinitis is treated mainly in the primary care setting. Up to 39% of patients are treated with multiple products. About 60% did not have a diagnosis matching one of the primary diagnoses studied. The absence of such diagnosis coupled with the significant use of multiple _The C-=J Prescription Costs _ Diagnosis Costs $200 $177 $210 - S20..' 1 I - I I $150 $131 $100 .. $188 $188 Oral Combination $151 $103 $50 $0 Nasal Nasal Steroids Antihistamines products suggests that physicians may be treating empirically. Whether these products are targeting the underlying causes of rhinitis is questionable. Diagnosis Costs Antihistamines Approaching Ideal Treatment A process in Primary Care Physician's Perspective According to the reference study conducted by Tricore, only 40% of patients receiving prescriptions for rhinitis had a related diagnosis. Physicians today, especially primary care physicians, are experiencing greater demands on their time and may need to see more patients in a day and take care o[ patient complaints quickly without benefit o[ a complete histOlY and exam. To provide some relief [or their patients, physicians may choose an antihistamine, knowing that about half the time it will work. Patients come .to physicians anned with in[ormation from direct-to-consumer marketing, the popular press, or the Internet. They are requesting particular rhinitis medications by name to treat their rhinitis symptoms. This therapeutic category is one o[ those most aggressively targeted by direct-to-consumer advertising. Patients [urther believe they have researched the topic well enough to know exactly what they need. According to the 2000 Novartis pharmacy benefit report, prescriptions in the category grew by over 30% in 1999. When physicians empirically choose an antihistamine treat- ment, the outcomes can be predicted based on the nature of the patient's rhinitis symptoms. For the 43% of patients whose symptoms are purely allergic, antihistamine therapy will probably improve symptoms. For the 57% of patients whose symptoms are either purely nonallergic or mixed, antihistamine therapy wi11 be only partially effective or ineffective (see Figure 2, page 10). Vol. 7. No.2 which less than half the patients treated get relief after their initial visits is not satisfactory. Physicians need a process that will bring greater patient satisfaction, yield better results in a shorter time, and be more cost effective. As early as possible, patients who present with rhinitis symp- toms should have their symptoms categorized as pure allergic, pure nonallergic, or mixed. Patients whose symptoms are purely allergic can be tested [or potential allergens, be treated for their symptoms, and learn to remove or avoid those allergens. The remaining patients can then have their symptoms treated with an effective medication while causes are investigated (see Figure 3, page 10). A Diagnostic Tool For this ideal treatment approach to work, physicians must be able to establish a diagnosis quickly; they need a tool or a technique that integrates the patient into the proce'ss, one that would help patients understand the causes of their symptoms and guide their expectations about treatment. Dr. Phillip Lieberman, clinical professor o[ medicine at the University of Tennessee School ofMeclicine, has developed a simple, self-administerecl screening tool designed to help patients and physicians identify rhinitis etiology (see Figure 4, page 11). The patient can complete the evaluation independent of the physician. With the data presented by the patient, the physician can easily conduct a focused patient assessment and choose the March/April 2001 Supplement to the Journal of Managed Care Pharmacy 9