Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
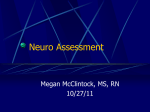
doi:10.1093/brain/awn010 Brain (2008), 131, 1142^1155 Paroxysmal hemicrania: a prospective clinical study of 31 cases Elisabetta Cittadini,1 Manjit S. Matharu1 and Peter J. Goadsby1,2 1 Institute of Neurology, The National Hospital for Neurology and Neurosurgery, Queen Square, London, UK and Headache Group, Department of Neurology, University of California, San Francisco, San Francisco CA, USA 2 Correspondence to: Professor Peter J. Goadsby, Headache Group, Department of Neurology, University of California, San Francisco, Box 0114, 505 Parnassus Avenue, San Francisco, CA 94 143- 0114, USA E-mail: [email protected] Paroxysmal hemicrania is a rare syndrome characterized by repeated attacks of strictly unilateral, severe, short-lasting pain occurring with cranial autonomic features. The hallmarks of this syndrome are the relatively short attacks and the exquisite response to indometacin.We describe the phenotype of this condition in a series of 31 patients.The mean duration of attack was 17 min.The mean attack frequency was 11.The distribution of the pain was orbital and temporal in 77% of the patients, retro-orbital in 61%, frontal in 55%, occipital in 42%; although pain was also reported in the vertex, second division of trigeminal nerve, neck, nose, jaw, parietal region, ear, teeth, eyebrow, shoulder (ipsilateral and bilateral), arm and third division of trigeminal nerve. Of the cohort, 87% had lacrimation, 68% had conjunctival injection, 58% rhinorrhoea, 54% nasal congestion, ptosis and facial flushing. Other cranial autonomic features include eyelid oedema, forehead/facial sweating, sense of aural fullness and periaural swelling, miosis, mydriasis and swelling of the cheek. The majority of the patients (80%) were agitated or restless, or both, with the pain and 26% were aggressive. All patients had positive placebo control indometacin test (100^200 mg intramuscularly), or a positive oral indometacin trial or both. We suggest the International Headache Society criteria be revised to remove specification of attack site, and to include the full range of cranial autonomic features. Currently, the sine qua non for paroxysmal hemicrania is a response to indometacin. Since there is no reliable clinical marker of that response we recommend an indometacin test, either orally or by injection for any patient with lateralized discrete attacks of head pain with associated cranial autonomic symptoms. Keywords: paroxysmal hemicrania; trigeminal autonomic cephalalgias; indometacin; cluster headache Abbreviations: CGRP = calcitonin gene-related peptide; HIS = International Headache Society; NO = nitric oxide; PH = paroxysmal hemicrania; REM = rapid eye movement; SUNCT/SUNA = short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing syndrome; TAC = trigeminal autonomic cephalalgia; VRS = verbal rating scale. Received August 18, 2007. Revised December 10, 2007. Accepted January 10, 2008. Advance Access publication February 5, 2008 Introduction Paroxysmal hemicrania (PH) is a relatively rare primary headache disorder first described by Sjaastad and Dale (1974) and christened ‘chronic paroxysmal hemicrania’ 2 years later (Sjaastad and Dale, 1976). Patients have been described in several countries (Joubert et al., 1987; Antonaci and Sjaastad, 1989; Sjaastad, 1992). The incidence and prevalence of PH has been estimated to be about 1–3% that of cluster headache (Antonaci and Sjaastad, 1989), or about 1 in 50 000 (Matharu et al., 2003a), although it may be rarer (Sjaastad and Bakketeig, 2007). None of these estimates are based on substantial series. PH is classified as a trigeminal autonomic cephalalgia (TACs) by the International Headache Society (IHS) (2004), and defined by at least 20 attacks of severe unilateral orbital, supraorbital or temporal pain, lasting 2–30 min, accompanied by ipsilateral cranial autonomic features such as ptosis, eyelid oedema, conjunctival injection, lacrimation, nasal blockage or rhinorrhoea. Attacks usually have a frequency of above five a day, and respond completely to indometacin. In the first edition of the classification (1988), all cases were referred to as chronic PH. However, with validation of the episodic variant over subsequent years (Kudrow et al., 1987; Newman et al., 1992; Goadsby and Lipton, 1997), the second edition of the classification recognized both an episodic and a chronic form ß The Author (2008). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: [email protected] Paroxysmal hemicrania (Headache Classification Committee of The International Headache Society, 2004). Case series of PH have been presented with 84 cases reviewed in from the literature for the largest one (Antonaci and Sjaastad, 1989). Russell (1984) described 105 attacks, although sample from only five patients with chronic paroxysmal hemicrania to assess severity, duration and circadian pattern. In 2002, Boes and Dodick (2002) retrospectively reviewed 74 cases from the Mayo Clinic in an attempt to further refine the clinical spectrum of this condition. More recently, Zidverc-Trajkovic and colleagues (2005) reported eight consecutive patients affected by PH. Until now, the rarity of the syndrome has prevented substantial cohorts to be collected by one group over a short enough period to provide a broadly based prospective description of the syndrome with the same persons conducting the clinical interviews. Therefore, the aim of this study was to describe in detail the clinical picture of PH by assessing prospectively a large group of patients. The work was initially reported in preliminary form at the 16th Migraine Trust International Symposium (London, 18–20 September 2006, Cittadini and Goadsby, 2006). Methods Thirty-one patients (mean age 37 years, range 5–68) with possible PH, were identified at the National Hospital for Neurology and Neurosurgery and the Hospital for Sick Children, Great Ormond Street from May 1995 to January 2007 and attended the outpatient departments between January 2004 and January 2007. The data used for this study were obtained from the clinical notes and by information received on the phone by one of us (E.C.). Patients were seen by at least two specialists in the out-patient clinic, and some were seen more than once if admitted for investigation. Twenty-eight patients were contacted by telephone after giving written consent, or consent during the clinic appointment. Two subjects were not contacted by telephone because they were children; their history had been taken directly by one author and they were followed up through their parents (P.J.G.). One patient was lost to follow-up and we used his medical notes to obtain the information. Again, this patient had had the history taken directly by one of us (P.J.G.). The study was approved by the National Hospital for Neurology and Neurosurgery Joint Research Ethics Committee. A standard proforma of questions, including side, site, type of pain, severity, duration, frequency and periodicity of the attacks; presence or absence of autonomic features; possible triggers and behaviour during the attacks was completed for each patient. The response to oral indometacin and the placebo-controlled Indotest (Matharu et al., 2004) was assessed. In addition, the patient’s response to other medications, and personal and family history of headache were recorded. Information regarding response to other medications and neuroimaging reports were collected from the clinical notes. The results were collated and summarized using Excel (Microsoft). Brain (2008), 131, 1142^1155 1143 Results Of 31 patients, 26 patients had PH as defined by the IHS Classification Committee (2004). Five patients had shortlasting head pain with cranial autonomic features responding absolutely and robustly to indometacin but not fulfilling the current IHS criteria (Headache Classification Committee of The International Headache Society, 2004). In particular, one patient (#13) reported as an autonomic feature a sense of aural fullness and had a low frequency of attacks (three per day), and three patients (#14, #18, #29) had a low frequency of attacks over a 24-h period, two, three and four per day, respectively. Another patient reported unilateral pain localized over the occipital region (#17). Clinical characteristics used by the IHS to define PH Pain Laterality. Fifteen patients (48%) had exclusively rightsided attacks; 15 (48%) patients had exclusively left-sided attacks and one (3%) patient had side alternating attacks, which were more frequent on the right side. Site of attacks. The majority of the patients complained of pain in the distribution recognized by the IHS (Headache Classification Committee of The International Headache Society, 2004), which included: 24 (77%) in the temporal region and orbital region and 19 (61%) in the retro-orbital region. Their pain was also reported in the frontal region in 17 (55%), the occipital region in 13 (42%), the vertex in 11 (36%), the maxillary (second) division of the trigeminal nerve in 10 (32%), the neck in eight (26%), the nose and jaw in six (19%), the parietal region in five (16%) and the ear and teeth in four (13%) patients. Furthermore, the pain was over the eyebrow, ipsilateral shoulder and ipsilateral arm in three (10%) patients each. One patient had pain over the shoulder bilaterally and another one had pain over the mandibular (third) division of the trigeminal nerve (Table 1). Severity of the pain. Patients were asked to rate the severity of their attacks on a verbal rating scale (VRS) of 0 to 10, 0 being no pain at all and 10 the most severe pain imaginable. Twenty patients (65%) rated their most painful attacks at 10. Five patients (16%) rated their most painful attacks at nine. One patient rated the most painful attack between 8 and 10 and another one rated the most painful attack between 8 and 9. Two (6%) patients rated their most painful attacks at seven. The pain was reported severe/very severe in two children. Twenty (65%) patients said that this was the most painful condition they had ever experienced comparing it to childbirth and perforation of duodenal ulcer. Cranial autonomic features According to the IHS classification criteria (Headache Classification Committee of The International Headache Society, 2004), patients with PH are required to have at least one of the cranial autonomic feature. In our cohort, 1144 Brain (2008), 131, 1142^1155 E. Cittadini et al. Table 1 Site of attacks Site n (%) Temporal region Orbital region Retro-orbital region Frontal region Occipital region Vertex V2 Neck Nose Jaw Parietal region Ear Teeth Eyebrow Shoulder Arm V3 24 (77) 24 (77) 19 (61) 17 (55) 13 (42) 11 (36) 10 (32) 8 (32) 6 (19) 6 (19) 5 (16) 4 (13) 4 (13) 3 (10) 3 Ipsilateral (10%) and 1 bilateral (3%) 3 Ipsilateral (10%) 1 (3) Table 2 Associated cranial autonomic symptoms Autonomic feature n (%) Lacrimation Conjunctival injection Rhinorrhoea Nasal congestion Ptosis Facial flushing Eyelid oedema Forehead/facial sweating Aural fullness Aural swelling Miosis Mydriasis Swelling of the cheek 27 (87) 21 (68) 18 (58) 17 (55) 17 (55) 17 (55) 13 (42) 10 (32) 8 (26) 4 (13) 3 (10) 2 (6) 1 (3) we found autonomic features at the following frequencies: 27 (87%) patients had lacrimation, 21 (68%) had conjunctival injection, 18 (58%) had rhinorrhoea, 17 (55%) had nasal congestion, 17 (55%) had ptosis, 13 (42%) had eyelid oedema, 10 (32%) had forehead and facial sweating and three (10%) had miosis. In addition, other autonomic features were reported such as facial flushing in 17 (55%) patients, a sense of aural fullness in eight (26%) and a sense of aural swelling in four (13%) patients. Two (6%) patients reported ipsilateral mydriasis and one (3%) patient reported swelling of the cheek. One of our patients had only a sense of ear fullness during the attacks and denied all the other autonomic symptoms. Another patient sometimes had cranial autonomic features without pain (Table 2; Pareja, 1995). Duration and frequency of attacks Length of attacks. The IHS criteria for the length of attacks in PH are between 2 and 30 min (Headache Classification Committee of The International Headache Society, 2004). In our cohort, the range of the attacks was between 10 s and 4 h. In 17 (55%) patients, the longest attack duration was more than 30 min. One patient (#9) had one attack that lasted 48 h; therefore, this patient’s data were not included in the final analysis of length of attacks. The mean length of the attacks was 17 min and the median was 19 min. Number of attacks per day. The IHS criteria require the number of attacks per day to be more than five for more than half of the time (Headache Classification Committee of The International Headache Society, 2004). The number of attacks per day ranged from 2 to 50. The mean was 11 attacks in 24 h and the median was nine. In our cohort, four (13%) patients had fewer than four attacks a day for more than half of the time. In particular, in two patients (#13, #29) the range of the attacks in 24 h was between three and five, in one patient (#14) the range was between two and three, and in one patient (#18) the range was between two and four attacks per day. One patient (#26) reported a range of attacks between no attack and eight attacks per day with fewer than five attacks per day for more then half of the time when we saw and diagnosed the condition. However, during one of his previous bouts he had had seven to eight attacks per day. Indometacin response The IHS criteria require an absolute response to indometacin (Headache Classification Committee of The International Headache Society, 2004). In our cohort, 17 (55%) patients had the modified Indotest (Antonaci et al., 1998a); a placebo-controlled indometacin test with intramuscular indometacin at the dose of 100 or 200 mg (Matharu et al., 2004). Out of these 17 patients, 14 (82%) had a positive response. They subsequently underwent a trial of oral indometacin that was positive in 13 (93%) cases, with one case not assessable due to indometacin side-effects after a few days. Of the remaining three patients who had the Indotest, one had an equivocal response to the modified Indotest and two patients had a negative response. Each of these had a positive response to oral indometacin. Finally, 14 (45%) patients had only the oral trial with indometacin which was positive (Fig. 1). The mean daily dose of indometacin used in the oral trial based on 30 patients was 137 mg (range 30–300 mg). The median dose was 150 mg/day. Table 3 shows the daily effective dose for each patient. Clinical features not currently used by the IHS to define PH Age and gender of patients and duration of symptoms Seventeen patients were male and 14 were female (M:F ratio of 1:1). The mean age at the onset of the symptoms was 37 years (range 5–68). Paroxysmal hemicrania Brain (2008), 131, 1142^1155 31 patients 14 patients had positive oral indometacin response Indotest 17 patients Negative Indotest 2 patients Equivocal Indotest 1 patient Positive Indotest: 14 patients 13 pts had positive oral indometacin trials Positive oral indometacin trial 1 pt stopped oral trial due to side effects Positive Oral indometacin trial Fig. 1 Flow chart of patients who had the placebo-controlled Indotest and open label oral trials with Indometacin. 1145 Table 4 Characteristics of the pain Characteristics n (%) Sharp Stabbing Throbbing Shooting Burning sensation Constant Boring Pressure Knife in the head Tightening Dull Aching Sticking Pushing Cramped Toothache pain Tearing Twisting Screaming Stiffness Red hot poker Power drilling 16 (51) 15 (49) 10 (32) 4 (13) 4 (13) 3 (10) 3 (10) 2 (6) 2 (6) 2 (6) 2 (6) 2 (6) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) Table 3 The effective dose of indometacin per day Patient Daily dose of indometacin 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 200 ^225 mg 200 mg 50 mg 150 mg 200 mg 150 ^225 mg 150 ^300 mg 100 mg 150 mg 50 mg 50 ^75 mg 75^150 mg 50 mga 75 mg 150 mg 75 mg 250 mg 75 mg 150 mg 200 mg 50 mg 200 ^300 mg 30 mgb 50 mg 150 ^200 mg 300 mg 75 mg 150 mg 100 mg 200 mg 100 ^150 mg a Patient stopped the intake of indometacin after a few days due to side effects. bPatient 5½ years old. Type of pain In our group, the majority of the patients 16 (52%) described their pain as sharp and 15 (48%) referred to it as stabbing. In 10 (32%) patients, the pain was reported as throbbing. Other types of pain are reported in the Table 4. Triggering of attacks In our group, the attacks could be either triggered or spontaneous. Common triggers were stress or relaxation after stress in eight (26%) patients; exercise in seven (23%) patients; alcohol and neck movement in six (19%) patients, a warm environment, cold weather, a strong smell, bending down and coughing, were triggers in five (16%) patients each; sneezing in four (13%) patients; and, tiredness and straining in three (10%) patients each. Other less frequent triggers including cutaneous triggers, weather change, irregular sleep or lack of sleep, the perimenstrual or menstrual period and lifting were recognized by two (6%) patients each. Additional triggers were environment temperature change, cold–heat wind, dietary products (cream, cheese, chocolates, coffee, citrus fruits), skipping meals, flickering lights, sleep and pressure over the greater occipital nerve. These triggers were indicated by one (3%) patient in each category. We also used glyceryl trinitrate in four patients and this triggered a typical attack of PH in one. One patient noted that some bouts were precipitated by infections such as ear infection, tonsillitis and chest infection (Table 5). Agitation Agitation or a sense of restlessness is typical behaviour during cluster headache attacks, occurring in 490% of cases 1146 Brain (2008), 131, 1142^1155 E. Cittadini et al. Table 5 Triggers to attacks Characteristics n (%) Stress/relaxation after stress Exercise Alcohol Warm environment Strong smell Neck movement Cold weather Bending down Coughing Sneezing Tiredness Straining Cutaneous triggers Weather Change Irregular sleep/lack of sleep Period/week before the period Lifting Temperature change Cold/heat wind. Hot weather Skipping meal Dietary products (cream, chocolates, cheese, coffee, citrus fruits) Flickering lights sleep Pressure over the GON NTG Ear/chest infection, tonsillitis 8 (26) 7 (23) 6 (19) 5 (16) 5 (16) 6 (19) 5 (16) 5 (16) 5 (16) 4 (13) 3 (10) 3 (10) 2 (6)a 2 (6) 2 (6) 2 (6) 2 (6) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (3) 1 (25)b 1 (3) a Touching around the jaw, talking, chewing, resting the right side of the face on the pillow in one patient (#12). Touching the lower lip, talking, chewing, cleaning teeth, wind blowing against face in another patient (Boes et al., 2003). bNTG was used only in four patients. (Bahra et al., 2002). In a retrospective study of PH, 50% of the patients were agitated (Antonaci and Sjaastad, 1989), while in a more recent prospective study (Zidverc-Trajkovic et al., 2005) 63% were agitated. In a recent prospective study, agitation was described in 62% of SUNCT patients and in 55% of SUNA patients (Cohen et al., 2006a). In our cohort, 25 (80%) patients were agitated or restless, or both and eight (26%) patients were aggressive, mainly verbally rather than physically, during the attack. Migrainous symptoms Phonophobia and photophobia, which are usually bilateral, are typical features of migraine (Headache Classification Committee of The International Headache Society, 2004), although they can be unilateral in some cases (Drummond, 1986; Vingen et al., 1998). Unilateral phonophobia and photophobia have been reported to be more common in PH, hemicrania continua (Irimia et al., 2008), SUNCT (Cohen et al., 2006a; Irimia et al., 2008) and cluster headache (Vingen et al., 1998; Irimia et al., 2008). We found that 20 (65%) of our patients had phonophobia, which was unilateral in five (25%) patients. Out of these 20 patients, 16 (80%) had personal or family history for migraine, or headache not otherwise specified or both. Twenty (65%) patients had photophobia, which was unilateral in eight (40%) cases. Out of these 20 patients, 13 (42%) patients had personal or family history of migraine, or headache not otherwise specified or both. Motion sensitivity is a common symptom in migraine. We found 16 (52%) patients had motion sensitivity and 12 (39%) of these had a personal of migraine or family history of headache, or both. Osmophobia is well recognized in migraine (Kelman, 2004; Zanchin et al., 2005). In our cohort, seven patients had osmophobia and all had personal or family history of migraine, or headache not otherwise specified or both. Twelve (39%) patients in our cohort had nausea or vomiting during the attacks, or both. Each of these patients had a personal or family history of migraine, or headache not otherwise specified or both. It seems likely given the high population prevalence of migraine (Steiner et al., 2003) and data on the family history of migraine and headache severity (Stewart et al., 2006), that most severe headache reported here in families was migraine. Circadian and circannual periodicity It is reported in PH that the attacks occur regularly throughout the day, without a nocturnal preponderance (Russell, 1984; Antonaci and Sjaastad, 1989; Boes and Dodick, 2002; Zidverc-Trajkovic et al., 2005). However, nocturnal attacks associated with the rapid eye movement (REM) phase of sleep have also been described (Kayed et al., 1978). In our cohort, there was no clear preponderance of nocturnal attacks. Two (6%) patients (#2 and #26) had clear nighttime preponderance. In contrast with cluster headache, we did not find a strictly circadian and circannual periodicity, noting a considerable individual variation in attack periodicity. Fifteen (48%) patients reported their attacks were generally random over a 24-h period. Within this group, however, two patients (#1 and #4) specified that the attacks experienced at the onset of their headache used to occur at the same time during the 24 h, which was 04:00 h in one case, and afternoon and night for the other case. Another patient (#10) reported a period lasting 18 months during which one attack occurred at 11:00 h and he also had another period lasting three months during which he had one attack at 16:00 h. One patient (#17) reported that the attacks that occurred at night were more severe and longer than those during the day. The remaining 14 (45%) patients could have predictable attacks during the 24 h. Three patients (#3, #27, #29) had attacks only during the waking hours. One of these patients had one predictable attack at 19:30 h. Five patients (#6, #18, #20, #28, #30) had attacks mainly during waking hours. In one case one to two attacks tended to arrive at the same time each day and the others are random, whereas they Paroxysmal hemicrania were all predictable for the first 6 months. In another case, they occurred at the same time every morning and at hourly intervals and rarely during the night. One patient (#11) specified that although their attacks were mainly random, some tended to occur at the same time in the morning. One patient (#12) had attacks both in the morning and night; one patient (#13) had attacks during the waking hours (70% of the attacks) and in the early morning (30%); one patient (#21) stated that the first attack occurred around 09:00–10:00 h and then the other attacks were random during the day, though the worst attacks were in the evening. One patient (#25) reported attacks mainly during the waking hours and only occasionally at night, although they used to occur in the past either during the sleep hours or the waking hours; one patient (#19) had attacks during the day, whereas at the beginning they were present during both sleeping and waking hours and the worst attack was at 17:00 h. With regard to the circannual periodicity, one patient (#1) experienced a worsening of their attacks in spring and autumn, one (#3) during autumn and winter and another one (#17) had bouts tending to occur in February. Background pain, migraine and analgesic overuse Typically, PH is not characterized by interictal pain. In one prospective study (Zidverc-Trajkovic et al., 2005), one out of eight patients had tenderness between the attacks, while in a retrospective study interparoxysmal discomfort was reported in 28 out of 84 patients. We found that 18 (58%) patients had background pain between each attack. The presence of interparoxysmal pain raised the differential diagnosis of hemicrania continua. Careful interview and the use of headache diary tracking hourly pain allowed us to clarify the clinical presentation. Out of these 18 patients, eight (44%) had medication overuse. Seven (88%) of these eight patients had personal or a family history of migraine, or headache not otherwise specified, or both. The remaining 10 (56%) patients had background pain without analgesic overuse, and seven (70%) of them had personal history positive for headache, either migraine or headache the details of which were not available. The interparoxysmal pain in our cohort was relatively mild in comparison to the attack pain, a factor which serves to contrast these patients with those with hemicrania continua. We evaluated the relationship between migraine and PH and found that 16 (51%) patients had a personal history positive for migraine and 18 (58%) patients had a family history positive for migraine, or headache not otherwise specified or both. Medication overuse is associated with chronic daily headache in migraine (Bigal et al., 2004), and in cluster headache (Paemeleire et al., 2006) and SUNCT patients (Cohen et al., 2006a), with the common theme being background migrainousness (Goadsby, 2006). We assessed the presence of medication overuse, defined by the use of Brain (2008), 131, 1142^1155 1147 analgesic on 15 or more days per month, and found that it was present at some point in 10 (32%) patients. The analgesics used were codeine and paracetamol (acetaminophen) combinations, paracetamol, aspirin and caffeine combinations, ibuprofen, aspirin, paracetamol–caffeine– codeine–doxylamine combinations, caffeine and paracetamol combinations, ergotamine and caffeine combinations. Of this group, eight (80%) patients had positive personal history for migraine, or positive family history for headache or both. Periodicity and chronicity of PH PH can be classified as episodic or chronic depending on the presence of a remission period. About 20% of patients suffered from episodic PH, which is diagnosed when there is a remission period between bouts of attacks of at least 1 month (Headache Classification Committee of The International Headache Society, 2004). The remaining 80% of patients have chronic PH, which is diagnosed when patients have daily attacks without a remission of at least 1 month. In contrast to cluster headache, in PH the chronic form is more frequent than the episodic form. Interestingly, in a recent prospective study of SUNA/ SUNCT the chronic form was also more frequent (Cohen et al., 2006a). We found that 20 (65%) patients had primary chronic PH at onset and six (19%) of these patients were completely in remission at interview. The mean duration of the chronic phase was 4.3 years (range 3–7 years). The mean duration of remission was 4.3 years (range 3–6 years). One patient with primary chronic PH had first a chronic phase lasting 3 years, followed by a remission lasting about 4 years, followed by an episodic phase lasting 1 year, followed by a remission of 1 year to date. Another patient with primary chronic PH initially had a chronic phase lasting about 3 years, followed by an episodic form lasting about 6 years, followed by a chronic form lasting about 3 years, followed by a remission lasting about 15 months and followed finally by a chronic form. Two (6%) patients had secondary chronic PH with a mean interval between the onset of the disease to the chronic form of about 34 months. Six (19%) patients had a primary episodic form, with their bouts lasting for a mean of 16 weeks (range 4–24 weeks), and a remission phase that lasted for a mean of 100 weeks (range of 12–376 weeks; 7.3 years). One patient with primary episodic PH had an unusually long remission, which lasted 3 years and another unusual short remission which lasted only 1 month. One (3%) patient had secondary episodic PH: he had a chronic form which lasted 3 years, followed by 9 months of remission and then a recurrence of two to three attacks over a period of 4 months. Two (6%) patients had post-traumatic chronic PH. One of them had first a chronic phase lasting 2 years, followed by an episodic phase lasting 1 year, followed by a remission period lasting another 1 year, followed by 1148 Brain (2008), 131, 1142^1155 a recurrence of his attacks for about 3 months and followed finally by a remission lasting 4 years to date. Medication responses In our cohort, 17 (55%) patients had oxygen with none having a good response, five (30%) a mild response and twelve (71%) patients no response. Twelve (39%) patients tried subcutaneous sumatriptan 6 mg with a good response in two cases (17%), a mild response in one (8%) patient and no response in nine (75%). Comorbidities, examination and MRI findings Four patients (13%) had abnormal findings on neurological examination. Three patients had sensory changes, which were hyperaesthesia to pinprick in V1-V2-V3 in one case, allodynia in V1 in the second case and there was loss of all sensory modalities over the medial aspect of the right upper and lower eyelid, and medial aspect of the area above the right supra-orbital ridge in the third case. One patient with a diagnosis of ophthalmic arterio-venous malformation, had impairment of the visual function in the corresponding eye which included: (i) ipsilateral ptosis, (ii) severely impaired visual acuity, (iii) large central scotoma, (iv) venous stasis on fundoscopy and (v) defect in the eye abduction and afferent papillary defect. Twenty-five (80%) patients had brain imaging, which included MRI or CT scan. Sixteen (64%) patients had normal intracranial appearances, while in nine (36%) cases radiological abnormalities were found. They were as follows: (i) Vascular loop compressing the trigeminal nerve ipsilateral to the pain and generalized cerebral involution in keeping with the patient’s age (#25); (ii) bilateral vascular loops not compressing the trigeminal nerve and some non-specific lesions in the periventricular and subcortical white matter of both frontotemporal areas (#12); (iii) ischaemic lesions in the basal ganglia and pons (#19); (iv) ophthalmic arterio-venous malformation (#14); (v) sphenoid wing meningioma, which was subsequently removed with only a temporary remission of the headache (#20); (vi) megacisterna magna (#6); (vii) bulky pituitary gland associated with a deviation towards the left side of the pituitary stalk. In this case, there was also a solitary and non-specific T2/ FLAIR hyperintense lesion within the subcortical white matter of the right frontal lobe (#18); (viii) several non-specific, non-enhancing foci of abnormal signal within the cerebral white matter and mild mucosa thickening throughout the paranasal sinuses and a 10-mm pineal cyst (#26); (ix) a prominent left vertebral artery, and an ectatic vertebro-basilar junction/basilar artery in close E. Cittadini et al. relation to the left trigeminal root entry zone ipsilateral to the pain. The patient underwent microvascular decompression with resolution of the pain since (#30). Discussion We described a large case series of patients affected by episodes of short-lasting unilateral headache with cranial autonomic symptoms responsive to indomeathcin: PH. Our data suggest that it is an excruciating syndrome with a high frequency and brief duration of attacks that is exquisitely sensitive to indometacin. In our cohort, some patients with otherwise typical attack phenotypes had frequencies below five per day, aural fullness or discomfort as a cranial autonomic feature and a wider cranial distribution of pain than has been previously recognized. Our case mix does not confirm the reported female preponderance. PH is a distinct relatively short-lasting, strictly unilateral primary headache with cranial autonomic features that responds to indometacin. Our data suggest some revision to the current diagnostic criteria (Table 6) and serve to remind clinicians of the existence of, and clinical features of this unique primary headache. Table 6 Diagnostic criteria for paroxysmal hemicrania Current diagnostic criteria 3.2 Diagnostic criteria A. At least 20 attacks fulfilling criteria B ^E. B. Attacks of severe unilateral, orbital, supraorbital or temporal pain last 2^30 min. C. Headache is accompanied by at least one of the following: 1. ipsilateral conjunctival injection and/or lacrimation; 2. ipsilateral nasal congestion and/or rhinorrhoea; 3. ipsilateral eyelid oedema; 4. ipsilateral forehead and facial sweating; 5. ipsilateral miosis and/or ptosis. D. Attacks have a frequency above 5 per day for more than half of the time, although periods with lower frequency may occur. E. Attacks are prevented completely by therapeutic doses of indometacin. F. Not attributed to another disorder. Proposed diagnostic criteria 3.2 R Diagnostic criteria A. At least 20 attacks fulfilling criteria B ^E. B. Attacks of unilateral pain lasting 2^30 min. C. Headache is accompanied by at least one of the following: 1. ipsilateral conjunctival injection and/or lacrimation; 2 ipsilateral nasal congestion and/or rhinorrhoea; 3. ipsilateral eyelid oedema; 4. ipsilateral forehead and facial sweating; 5. ipsilateral miosis and/or ptosis; 6. ipsilatreal forehead and facial flushing; 7. ipsilateral sense of aural fullness and/or periaural swelling. D. Attacks have a frequency above 5 per day for more than half of the time, although periods with lower frequency may occur. E. Attacks are prevented completely by indometacin. F. Not attributed to another disorder. Paroxysmal hemicrania Epidemiology PH is a rare syndrome. The relatively small number of patients that we diagnosed at the National Hospital for Neurology and Neurosurgery, and the Hospital for Sick Children, Great Ormond Street, given our referral base and interests, suggests this is the case. Considering we have seen more than 800 patients affected by TACs in the same period, our cohort is certainly small. In our group, the youngest patient with PH was 4-years old and the oldest was 68-years old. Our findings confirm the existing literature that states this condition can begin at any age (Kudrow and Kudrow, 1989; Broeske et al., 1993; Gladstein et al., 1994; de Almeida et al., 2004), but the mean age at onset is in the 30s (Antonaci and Sjaastad, 1989). The Vaga study suggests that the prevalence of PH is no more than 1 in 1838 (Sjaastad and Bakketeig, 2007), and is in line with our experience. Given nearly all the TACs seen in the period in our unit have been seen by at least one of us (P.J.G.), our data (Cohen et al., 2006a) and that again of the Vaga study (Sjaastad and Bakketeig, 2007), suggest that Short-lasting Unilateral Neuralgiform headache attacks with Conjunctival injection and Tearing (SUNCT/SUNA) syndrome is at least as common as PH. This may be a valuable clinical lesson. Our impression is that SUNCT is misdiagnosed more often as atypical trigeminal neuralgia than PH is misdiagnosed as cluster headache. Given the therapeutic implications neither mistake is helpful to the patients. Brain (2008), 131, 1142^1155 1149 widely in the face and head. This suggests a modification to the current criteria to acknowledge the side distribution, and is probably a finding that follows detailed questioning of a larger cohort of patients. Patients need to be asked about pain distribution, and conversely the distribution should not put one off the diagnosis. Autonomic symptoms By current definition, PH patients require at least one cranial autonomic feature with attacks. Lacrimation, nasal congestion, conjunctival injection and rhinorrhoea are the most frequent symptoms and signs accompanying the attack (Antonaci and Sjaastad, 1989). In our group, the majority of the patients (97%) had at least one of the autonomic features currently specified (Headache Classification Committee of The International Headache Society, 2004). However, a wider range of autonomic features was reported, such as facial flushing (55%), a sense of aural fullness (26%) or of aural swelling (13%). In particular, one patient only had the sense of aural fullness. Boes and colleagues (1998) recognized a similar symptom in a small series of patients, and we have found it clinically useful to enquire of this symptom. It can be found in each of the TACs, including cluster headache and SUNCT/SUNA and can be bothersome to some patients. Our findings suggest this symptom should be included in the list of cranial autonomic features in any revision of the diagnostic criteria for PH, and probably for TACs more broadly. Sex distribution Laterality and severity of attacks PH has been considered to be predominantly a problem of females. In the initial reported female:male ratio was 7 : 1 (Sjaastad and Dale, 1974), and in a subsequent review of 84 patients (Antonaci and Sjaastad, 1989) the female:male ratio was 2.36 : 1. In our case series, we did not find a clear female preponderance. This is in mark contrast to cluster headache where there is a clear male preponderance (Bahra et al., 2002) and rather more similar to SUNCT at 1.5 male to 1 female (Cohen et al., 2006a). The prevailing view of PH as a condition of females may arise from mis-diagnosis of males with PH as cluster headache, as it is the more common problem and recognized to have a male preponderance. Typically the attacks of PH are strictly side-locked, although three cases of bilateral pain have been reported (Pollmann and Pfaffenrath, 1986; Mulder and Spierings, 2004; Bingel and Weiller, 2005). In our series, no patients had convincing bilateral attacks, and we have speculated that such patients may be a separate group (Matharu and Goadsby, 2005). Typically, cluster headache is described as an excruciating syndrome and is often called ‘suicide headache’ (Torelli and Manzoni, 2003), although it is now reasonably established that other TACs, as SUNCT/SUNA are indeed excruciating conditions (Cohen et al., 2006a). We found that the majority of our patients considered their pain to be the worst pain they had ever experienced with a severity of 10 out of 10 in a VRS. These findings support the general impression that TACs are indeed all extremely painful conditions and underscore the importance of accurate diagnosis and swift management to alleviate the patients’ very considerable suffering. Site of the pain The IHS (Headache Classification Committee of The International Headache Society, 2004) considers the site of the pain to be unilateral, supraorbital or temporal, and a previous case series reported frequent localization in the ocular and temporal regions (Antonaci and Sjaastad, 1989). In our cohort, we also found that pain was mainly reported over the temporal (77%) region, orbital (77%) and supraorbital/frontal region (55%) consistent with the current criteria. However, the pain was also reported Duration and frequency Current criteria for the diagnosis of PH mandate attack duration of 2 and 30 min and a frequency of more than five attacks per day for more than half of the time (Headache Classification Committee of The International Headache 1150 Brain (2008), 131, 1142^1155 Society, 2004). In a prospective study of 105 attacks in five patients (Russell and Storstein, 1984), the mean attack duration was 13 min with a range of 3–46 min and the mean attack frequency was 14 attacks in 24 h with a range of 4–38. We have found a range of the attack duration between 10 s and 4 h, with a mean of 17 min, although of the patients with very short attacks had longer attacks of several minutes. We noted in about half of the patients (55%) the attack duration was more than 30 min, although within each individual attacks of 30 min or less would occur. One patient even had an attack that lasted 48 h. Whether this was one attack or not can never be established retrospectively, although patient histories at the outset are always retrospective so it is valuable to be aware of this variability. The longer attack length can lead to the misdiagnosis of cluster headache, although the lack of response to oxygen and sumatriptan are against that conclusion, as is the positive response to indomethacin. Moreover, one would expect variability over time with bouts not being identical in episodic PH and some variability in chronic PH from year to year until it is treated. Interictal painçPH versus hemicrania continua An interictal discomfort or pain is reported in up to onethird of patients (Antonaci and Sjaastad, 1989). We found that 18 patients had background pain between each attack. The main differential diagnosis here is hemicrania continua. A headache diary is very useful during the work-up of PH as it can provide important information regarding temporal aspects of the pain. In our experience PH typically has prominent cranial autonomic features, whereas in hemicrania continua these features are modest or inconstant. Further, in PH the attacks are much more severe and the attack length is relatively short, compared with longer less severe worsenings of hemicrania continua. It is also our general impression that background pain in PH is generally less severe than it is in hemicrania continua (Matharu et al., 2003a). A careful history supplemented with a headache diary allows these distinctions to be made. It must be said that a weakness of this analysis might be the view that both disorders are on a spectrum. Given the clinical distinctions above and the very different pattern of brain imaging seen when comparing PH (Matharu et al., 2006) to hemicrania continua (Matharu et al., 2004), it would seem reasonable to continue to endeavour to study these conditions separately. Concomitant headache, migraine and background pain In our cohort, 16 (52%) patients had a personal history of migraine. Migraine is common (Steiner et al., 2003), and so commonly seen in patients with other trigeminal autonomic cephalalgias, such as cluster headache (Bahra et al., 2002) E. Cittadini et al. and SUNCT/SUNA (Cohen et al., 2006a). The high prevalence of migraine in our group may suggest a predisposition for primary headaches, patients with a disabling headache seeking medical advice more often or perhaps reveals that the biological predisposition to migraine is more common than we have hitherto considered. If one considers the peak prevalence of migraine about one-third of adult Western females, using criteria (Headache Classification Committee of The International Headache Society, 2004) that would under-diagnose migraine by excluding patients with so-called tension-type headache with one migraine feature, such as photophobia or phonophobia, or patients with now accepted chronic migraine (Olesen et al., 2006), is the background genetic rate of migraine much higher than previously considered? It may simply be that in patients with two genetic hits—PH and migraine, the migraine biology is more likely to be activated than without the extraPH-problem. Indeed, patients with migraine (Wilkinson et al., 2001; Bahra et al., 2003), cluster headache (Paemeleire et al., 2006) or SUNCT/SUNA (Cohen et al., 2006a) with underlying migraine biology tend to dominate cohorts who develop medication overuse headache. Here, seven of eight patients with medication overuse had migraine biology, which supports the emerging principle that migraine, active or latent, may be the crucial factor in predisposing to medication overuse problems (Goadsby, 2006). Behaviour Typically, patients with cluster headaches are agitated and restless (Torelli and Manzoni, 2003), indeed aggressive behaviour is seen (Bahra et al., 2002). Recently, it has been reported that 62% of the patients with SUNCT were agitated during attacks (Cohen et al., 2006a). In both conditions, activations in the region of the posterior hypothalamic grey have been reported using functional imaging techniques (May et al., 1998, 1999; Cohen et al., 2006b). Importantly, posteromedial hypothalamotomy has been used as a therapeutic treatment in patients with behavioural disorders that include aggression (Sano et al., 1970; Schvarcz et al., 1972; Sano and Mayanagi, 1988). Recent functional imaging results with PH identify again activations in the region of the posterior hypothalamic grey (Matharu et al., 2006), as for cluster headache and SUNCT. Whether the area is indeed hypothalamic or sub-thalamic, such as the calcitonin gene-related peptide (CGRP) neurons of the sub-parafasicular thalamus (de Lacalle and Saper, 2000) is yet to be determined. Our finding here that 80% of the patients were agitated, or restless or both, and one quarter were described as being aggressive during the pain is consistent with the broad correlation of the functional imaging findings with the phenotype of the attack. Family history A family history of PH has been reported (Cohen et al., 2006a), and this case is in our reported cohort (#6). Paroxysmal hemicrania Brain (2008), 131, 1142^1155 1151 Table 7 Comparison on the trigeminal autonomic cephalalgias based on cohorts we have studied (Bahra et al., 2002; Cohen et al., 2005; Cohen et al., 2006a) and patients we have reviewed (Cohen et al., 2007) Sex Pain Quality Severity Distribution Attacks Frequency (per day) Length (minutes) Triggers Alcohol NTG Cutaneous Agitation/restlessness Episodic versus chronic Circadian/circannual periodicity Treatment effects Oxygen Sumatriptan 6 mg Indomethacin Migraine features with attacks Nausea Photophobia/phonophobia Cluster headache Paroxysmal hemicrania SUNCT/SUNA 3M to 1F M=F 1.5M to 1F Sharp/stab/throb Very severe V14C24V24V3 Sharp/stab/throb Very severe V14C24V24V3 Sharp/stab/throb Severe V14C24V24V3 1^ 8 30 ^180 20 2^30 100 1^5 +++ +++ + + 90% 90:10 Present 80% 35:65 Absent +++ 65% 10:90 Absent 70% 90% No effect No effect 20% 100% No effect 510% No effect 50% 65% 40% 65% 25% 25% Although there are exceptions to all rules the responses and effects listed reflect the behaviour of the largest parts of the cohorts we have studied. SUNCT = SUNA, Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing/short-lasting unilateral neuralgiform headache attacks with cranial autonomic features; C = cervical; V = trigeminal. Typically, migraine is described as a genetic headache disorder (Ferrari, 1998) and mutations have been discovered in patients affected by familial hemiplegic migraine (Ophoff et al., 1996; De Fusco et al., 2003; Dichgans et al., 2005). Among the TAC syndromes, a family history of CH (Leone et al., 2001) and SUNCT has been reported (Gantenbein and Goadsby, 2005). A large group of patients need to be evaluated in order to establish a genetic component, although the rarity of this disorder will make this a challenge. It certainly seems likely that the underlying determinant of the disorder is genetically determined. Triggers Most attacks are spontaneous, while it is reported that 10% of patients can trigger an attack with neck movement and about 7% of the patients can trigger an attack with alcohol (Antonaci and Sjaastad, 1989). In our cohort, the majority of the attacks were spontaneous; when identified triggers included stress or relaxation after stress, alcohol, exercise and neck movement. In comparison, cluster headache attacks can be typically and easily triggered by alcohol, nitroglycerine (NTG) (Ekbom, 1968; Fanciullacci et al., 1995), exercise, strong smells and increased body heat (Bahra et al., 2002), whereas in SUNCT/SUNA the attacks are generally triggered by cutaneous triggers such as touching the face or scalp, washing, shaving, eating brushing the teeth, talking and coughing (Pareja and Sjaastad, 1997; Cohen et al., 2006a). One patient out of four reported a typical attack following use of a NTG spray. In general terms, lack of response to alcohol, NTG and lack of cutaneous triggers to attacks are clinical pointers to PH when considering the differential diagnosis among the TAC syndromes (Table 7). Indometacin response A response to indometacin has been said to be a sine qua non in PH and we have adopted that position to define the cohort here. The mean daily dosage is 100 mg with a range of 25–300 mg. However, some patients needed only 12.5 mg/day (Antonaci and Sjaastad, 1989). We found that all patients (97%) who could tolerate oral indometacin had an absolute response to the oral trial. The range of effective doses in our cohort varied between 30 mg in a 5-year old to 300 mg/day. Interestingly, we noted that one patient had (#26) had a highly effective response during two consecutive trials with indometacin. However, a third trial at the highest dose of 375 mg/day for 2 weeks was not beneficial and subsequently fourth trial at the dose 300 mg/day was beneficial. Otherwise, responses and doses tended to be stable with time so that it is our practice to 1152 Brain (2008), 131, 1142^1155 re-examine and re-image the brain in patients who stop responding. Some two-thirds of patients report at some point side-effects, mainly gastrointestinal problems, which may lead to a discontinuation of the medicine. In this context, where gastrointestinal side-effects have been a problem employing a placebo-controlled Indotest by injection was very helpful (Matharu et al., 2004). In our cohort, the majority of the patients (82%) had a positive test, which confirmed the diagnosis of PH. We also assessed the response to high-flow oxygen and sumatriptan subcutaneously, which are typically positive in cluster headaches (Lance and Goadsby, 2005). Open label use of subcutaneous sumatriptan 6 mg has been reported to be reported to be both ineffective (Dahlof, 1993; Antonaci et al., 1998b) and helpful (Pascual and Quijano, 1998) in patients with PH. If one considers a good or better response as an outcome, in our patients oxygen was no effective. Sumatriptan subcutaneously was either clearly useful in about 20% or not useful at all; this would explain the controversy in the literature which is simply a sampling issue. A response to sumatriptan should not distract from a trial of indometacin. Neurological examination, secondary headache and associations As a rule, patients with PH tend to have normal neurological examinations. In our group, three (10%) patients had sensory impairment: hyperaesthesia to pinprick in V1-V2-V3 in one case (#12), allodynia in V1 in a second case (#3) and in the third case, sensory loss in all modalities over the medial aspect of the right upper and lower eyelid, and medial aspect of the area above the right supra-orbital ridge. One patient (#12) of this group had bilateral vascular loops not compressing the trigeminal nerve and the sensory impairment was on the same side of the attack. One patient had post-traumatic PH and the sensory impairment was attributed to damage of the trigeminal nerve following a traumatic injury (#29, Matharu and Goadsby, 2001). One patient (#14) with an arterio-venous malformation had impairment of visual acuity in the corresponding eye. The headache was on the same side of the malformation, although it started about 18 years after the initial presentation of the proptosis. When he developed PH, the proptosis had progressed significantly. Three years later, he underwent a trial with indometacin with complete resolution of the headache. It seems unlikely that the malformation was causal. Overall, in our case series there is only infrequent impairment of the trigeminal nerve. This is substantially different form the recent data regarding SUNCT/SUNA syndrome in which the reduced facial sensation may be more common (Cohen et al., 2006a). Probably as a result of publication bias, secondary PH is relatively common in the literature in comparison to the primary variety, and has been suggested to be caused by a diverse set of pathological processes (Boes and Dodick, 2002). E. Cittadini et al. One of our patients had an ischaemic lesion in the basal ganglia and pons, which may account for the problem (#19). PH has been described in patients with macroprolactinoma (Boes et al., 1998; Sarov et al., 2006), prolactinsecreting adenoma (Raskin, 1988) and microadenoma (Gatzonis et al., 1996). Pituitary adenoma have also been reported in patients with SUNCT (Ferrari et al., 1988; Massiou et al., 2002; Levy et al., 2003; Matharu et al., 2003b) and in patients with cluster headache (Greve and Mai, 1988; Milos et al., 1996; Porta-Etessam et al., 2001; Negoro et al., 2005). Several hypotheses have been proposed to explain the association between pituitary adenomas and TAC syndromes. First, these tumours may have a mechanical effect. Second, an increased intrasellar pressure may play a role in the genesis of the headache (Arafah et al., 2000). Finally, it has been proposed that the pathogenesis of the attacks is predominately neurohormonally mediated rather than by the size or invasiveness of the tumour (Levy et al., 2004). Activation of the headache phenotype by treatments aimed at biochemical change in smaller tumours and the early recrudescence of symptoms with biochemical changes (Levy et al., 2005) both favour a non-mechanical explanation. PH has been reported in association with migraine, cluster headache, trigeminal neuralgia and cough headaches (Matharu et al., 2003a). We had two patients with PH-tic syndrome, that we have reported previously (Boes et al., 2003). Both patients had abnormal brain MRI findings: one patient (#25) had vascular loop compressing the trigeminal nerve on the same side as the pain and the other patient (#30) had an ectatic basilar artery close to the trigeminal root entry zone, ipsilateral to the side of his head pains. The latter underwent microvascular decompression with a resolution of both pains and he has been pain-free for the last 5 years. So far, there have been no other reports of vascular decompression procedures in PH-tic-syndrome (Hannerz, 1993; Caminero et al., 1998; Martinez-Salio et al., 2000; Zukerman et al., 2000; Boes et al., 2003; Leone et al., 2006). Occasionally, cluster-tic syndrome can be also associated with trigeminal nerve compression (Solomon et al., 1985), although in those four cases the vascular decompression leads only to relief of the tic component. PH has been described in association with cough headache (Mateo and Pascual, 1999) and both headaches responded well to indometacin. We had one patient (# 9) with PH and a cough headache. Interestingly, only the paroxysmal pain responded satisfactory to indometacin whereas the cough pain did not improve. Meningioma of cavernous sinus has been described in association with PH (Sjaastad et al., 1995) with only a moderate and transient improvement of the headache following excision. We had one patient (#20) with a history of sphenoid wing meningioma. The removal of the tumour led to a transitory remission lasting about 9 months. After this period, the pain came back with the same pattern that was evident preoperatively. Paroxysmal hemicrania Pathogenesis The pathogenesis of PH is poorly understood in relation to other primary headaches, such as migraine (Goadsby and Oshinsky, 2008). CGRP and vasoactive intestinal polypeptide (Goadsby and Edvinsson, 1996) are elevated during acute attacks of PH. This release is likely to mark trigeminovascular system and cranial parasympathetic activation, and is similar to that observed in cluster headache (Goadsby and Edvinsson, 1994). Trigeminal and autonomic activation in concert seems a marker of this group of syndromes—the trigeminal—autonomic cephalalgias (TACs, Goadsby and Lipton, 1997). The physiology of this system is relatively well described (May and Goadsby, 1999), indeed a degree of cranial autonomic activation is a normal response to a cranial nociceptive input (May et al., 2001). An important new dimension to understanding these syndromes, and PH in particular, comes with the application of functional imaging techniques. It has been shown during PH there is activation in the posterior hypothalamic region (Matharu et al., 2006), in addition to ventral midbrain activation. The same region near the posterior hypothalamus is also activated in cluster headache and SUNCT (Cohen and Goadsby, 2006), while the ventrolateral midbrain area is activated in hemicrania continua (Matharu et al., 2004). Whether this later area holds the key to understanding the indometacin effect in these syndromes remains one of the more fascinating questions for the next few years. Indometacin inhibits the production of nitric oxide (NO) by endothelial and inducible nitric oxide synthase (Beasley et al., 1998; Hrabak et al., 2001) and perhaps works by antagonizing one or more steps in the NO pathway, although given the relatively small proportion of PH patients sensitive to nitroglycerin in our series there must be other aspects to this problem. Certainly posterior hypothalamic region activation is the common theme of TACs (Cohen and Goadsby, 2006) and with the clinical picture makes a useful case for the utility of the grouping. Conclusion We have described 31 patients affected by PH and have characterized the clinical picture of this disorder in great detail. An advantage of the study is that all patients have been seen by at least two clinicians with extensive experience of TACs, that the cases have been contemporaneously seen and that the clinical aspects have been done prospectively. A limitation of all hospital-based studies is the bias of referral; however, for such a rare condition there seems no other reasonable way to collect an appropriate cohort. We have found the current IHS classification (Headache Classification Committee of The International Headache Society, 2004) to be helpful, and provide suggestions based on our data for a revision. We propose removing specifying the site of pain accepting that it can be anywhere on the head, and to include other autonomic Brain (2008), 131, 1142^1155 1153 features, such as ipsilateral forehead/facial flushing, ipsilateral sense of aural fullness and periaural swelling in the range of cranial autonomic features present during the attacks (Table 6). We emphasize that the absolute response to indometacin is essential for the diagnosis, and suggest the placebo-controlled Indometacin test as a suitable aid in the diagnostic evaluation. We note the frequency of the attacks is more than five per day, although low attack frequency can be present with other typical attacks. Moreover, while the typical attack is short at 20 min, longer attacks occur. Interestingly, the majority of the patients showed signs of agitation, or restlessness or both and about one-third were aggressive during the attacks consistent with the neuroimaging of the TACs locating some important part of the pathophysiology to the posterior hypothalamic region. PH is a treatable primary headache that is very rewarding to diagnose and manage that can be differentiated on clinical grounds from the other TACs (Table 7) in order to provide optimal management. References Antonaci F, Pareja JA, Caminero AB, Sjaastad O. Chronic paroxysmal hemicrania and hemicrania continua. Parenteral indomethacin: the ‘Indotest’. Headache 1998a; 38: 122–8. Antonaci F, Pareja JA, Caminero AB, Sjaastad O. Chronic paroxysmal hemicrania and hemicrania continua: lack of efficacy of sumatriptan. Headache 1998b; 38: 197–200. Antonaci F, Sjaastad O. Chronic paroxysmal hemicrania (CPH): a review of the clinical manifestations. Headache 1989; 29: 648–56. Arafah BM, Prunty D, Ybarra J, Hlavin ML, Selman WR. The dominant role of increased intrasellar pressure in the pathogenesis of hypopituitarism, hyperprolactinemia, and headaches in patients with pituitary adenomas. J Endocrinol Metab 2000; 85: 1789–93. Bahra A, May A, Goadsby PJ. Cluster headache: a prospective clinical study in 230 patients with diagnostic implications. Neurology 2002; 58: 354–61. Bahra A, Walsh M, Menon S, Goadsby PJ. Does chronic daily headache arise de novo in association with regular analgesic use? Headache 2003; 43: 179–90. Beasley TC, Bari F, Thore C, Thirkawala N, Louis T, Busija D. Cerebral ischemia/reperfusion increases endothelial nitric oxide synthase levels by an indomethacin-sensitive mechanism. J Cereb Blood Flow Metab 1998; 18: 88–96. Bigal ME, Rapoport AM, Sheftell FD, Tepper SJ, Lipton RB. Transformed migraine and medication overuse in a tertiary headache centre—clinical characteristics and treatment outcomes. Cephalalgia 2004; 24: 483–90. Bingel U, Weiller C. An unusual indomethacin sensitive headache: a case of bilateral episodic paroxysmal hemicrania without autonomic symptoms? Cephalalgia 2005; 25: 148–50. Boes CJ, Dodick DW. Refining the clinical spectrum of chronic paroxysmal hemicrania: a review of 74 patients. Headache 2002; 42: 699–708. Boes CJ, Matharu MS, Goadsby PJ. The paroxysmal hemicrania-tic syndrome. Cephalalgia 2003; 23: 24–8. Boes CJ, Swanson JW, Dodick DW. Chronic paroxysmal hemicrania presenting as otalgia with a sensation of external acoustic meatus obstruction: two cases and a pathophysiologic hypothesis. Headache 1998; 38: 787–91. Broeske D, Lenn NJ, Cantos E. Chronic paroxysmal hemicrania in a young child: possible relation to ipsilateral occipital infarction. Journal Child Neurol 1993; 8: 235–6. 1154 Brain (2008), 131, 1142^1155 Caminero AB, Pareja JA, Dobato JL. Chronic paroxysmal hemicrania-tic syndrome. Cephalalgia 1998; 18: 159–61. Cittadini E, Goadsby PJ. Revisiting the International Headache Society criteria for paroxysmal hemicrania: a case series of 21 patients. Cephalalgia 2006; 26: 1401–2. Cohen AS, Goadsby PJ. Functional neuroimaging of primary headache disorders. Expert Rev Neurother 2006; 6: 1159–72. Cohen AS, Matharu MS, Goadsby PJ. Suggested guidelines for treating SUNCT and SUNA. Cephalalgia 2005; 25: 1200. Cohen AS, Matharu MS, Goadsby PJ. Short-lasting Unilateral Neuralgiform Headache Attacks with Conjunctival injection and Tearing (SUNCT) or cranial Autonomic features (SUNA). A prospective clinical study of SUNCT and SUNA. Brain 2006a; 129: 2746–60. Cohen AS, Matharu MS, Goadsby PJ. Trigeminal autonomic cephalalgias: current and future treatments. Headache 2007; 47: 969–80. Cohen AS, Matharu MS, Kalisch R, Friston K, Goadsby PJ. Functional MRI in SUNCT (Short-lasting Unilateral Neuralgiform headache attacks with Conjunctival injection and Tearing) and SUNA (Short-lasting Unilateral Neuralgiform headache attacks with cranial Autonomic symptoms) shows differential hypothalamic activation with increasing pain. Cephalalgia 2006b; 26: 1402–3. Dahlof C. Subcutaneous sumatriptan does not abort attacks of chronic paroxysmal hemicrania (CPH). Headache 1993; 33: 201–2. de Almeida DB, Cunali PA, Santos HL, Brioschi M, Prandini M. Chronic paroxysmal hemicrania in early childhood: case report. Cephalalgia 2004; 24: 608–9. De Fusco M, Marconi R, Silvestri L, Atorino L, Rampoldi L, Morgante L, et al. Haploinsufficiency of ATP1A2 encoding the Na+/K+ pump 2 subunit associated with familial hemiplegic migraine type 2. Nat Genet 2003; 33: 192–6. de Lacalle S, Saper CB. Calcitonin gene-related peptide-like immunoreactivity marks putative visceral sensory pathways in human brain. Neuroscience 2000; 100: 115–30. Dichgans M, Freilinger T, Eckstein G, Babini E, Lorenz-Depiereux B, Biskup S, et al. Mutation in the neuronal voltage-gated sodium channel SCN1A causes familial hemiplegic migraine. Lancet 2005; 366: 371–7. Drummond PD. A quantitative assessment of photophobia in migraine and tension headache. Headache 1986; 26: 465–9. Ekbom K. Nitroglycerin as a provocative agent in cluster headache. Arch Neurol 1968; 19: 487–93. Fanciullacci M, Alessandri M, Figini M, Geppetti P, Michelacci S. Increase in plasma calcitonin gene-related peptide from extracerebral circulation during nitroglycerin-induced cluster headache attack. Pain 1995; 60: 119–23. Ferrari MD. Migraine. Lancet 1998; 351: 1043–51. Ferrari MD, Haan J, van Seters AP. Bromocriptine-induced trigeminal neuralgia attacks in a patient with pituitary tumor. Neurology 1988; 38: 1482–4. Gantenbein A, Goadsby PJ. Familial SUNCT. Cephalalgia 2005; 25: 457–9. Gatzonis S, Mitsikostas DD, Ilias A, Zournas CH, Papageorgiou C. Two more secondary headaches mimicking chronic paroxysmal hemicrania. Is this the exception or the rule? Headache 1996; 36: 511–3. Gladstein J, Holden EW, Peralta L. Chronic paroxysmal hemicrania in a child. Headache 1994; 34: 519–20. Goadsby PJ. Is medication-overuse headache a distinct biological entity? Nat Clin Pract Neurol 2006; 2: 401. Goadsby PJ, Edvinsson L. Human in vivo evidence for trigeminovascular activation in cluster headache. Brain 1994; 117: 427–34. Goadsby PJ, Edvinsson L. Neuropeptide changes in a case of chronic paroxysmal hemicrania- evidence for trigemino-parasympathetic activation. Cephalalgia 1996; 16: 448–50. Goadsby PJ, Lipton RB. A review of paroxysmal hemicranias, SUNCT syndrome and other short-lasting headaches with autonomic features, including new cases. Brain 1997; 120: 193–209. Goadsby PJ, Oshinsky M. The pathophysiology of migraine. In: Silberstein SD, Lipton RB and Dodick D, editors. Wolff’s headache and other head pain. New York: Oxford; 2008. p. 105–19. E. Cittadini et al. Greve E, Mai J. Cluster headache-like headaches: a symptomatic feature? A report of three patients with intracranial pathologic findings. Cephalalgia 1988; 8: 79–82. Hannerz J. Trigeminal neuralgia with chronic paroxysmal hemicrania: the CPH-tic syndrome. Cephalalgia 1993; 13: 361–4. Headache Classification Committee of The International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia 1988; 8: 1–96. Headache Classification Committee of The International Headache Society. The International Classification of Headache Disorders (second edition). Cephalalgia 2004; 24: 1–160. Hrabak A, Vercruysse V, Kahan IL, Vray B. Indomethacin prevents the induction of inducible nitric oxide synthase in murine peritoneal macrophages and decreases their nitric oxide production. Life Sci 2001; 68: 1923–30. Irimia P, Cittadini E, Paemeleire K, Cohen AS, Goadsby PJ. Unilateral photophobia or phonophobia in migraine compared with trigeminal autonomic cephalalgias. Cephalalgia 2008; 28: in press. Joubert J, Powell D, Djikowski J. Chronic paroxysmal hemicrania in a South African black. A case report. Cephalalgia 1987; 7: 193–6. Kayed K, Godtlibsen OB, Sjaastad O. Chronic paroxysmal hemicrania. 4. ‘‘REM sleep locked’’ nocturnal headache attacks. Sleep 1978; 1: 91–5. Kelman L. The place of osmophobia and taste abnormalities in migraine classification: a tertiary care study of 1237 patients. Cephalalgia 2004; 24: 940–6. Kudrow DB, Kudrow L. Successful aspirin prophylaxis in a child with chronic paroxysmal hemicrania. Headache 1989; 29: 280–1. Kudrow L, Esperanca P, Vijayan N. Episodic paroxysmal hemicrania? Cephalalgia 1987; 7: 197–201. Lance JW, Goadsby PJ. Mechanism and management of headache. New York: Elsevier; 2005. Leone M, Mea E, Genco S, Bussone G. Coexistence of TACS and trigeminal neuralgia: pathophysiological conjectures. Headache 2006; 46: 1565–70. Leone M, Russell MB, Rigamonti A, Attanasio A, Grazzi L, D’Amico D, et al. Increased familial risk of cluster headache. Neurology 2001; 56: 1233–6. Levy M, Jager HR, Powell MP, Matharu MS, Meeran K, Goadsby PJ. Pituitary volume and headache: size is not everything. Arch Neurol 2004; 61: 721–5. Levy M, Matharu MS, Meeran K, Powell M, Goadsby PJ. The clinical characteristics of headache in patients with pituitary tumours. Brain 2005; 128: 1921–30. Levy MJ, Matharu MS, Powell MP, Meeran K, Goadsby PJ. Phenoytpic characterisation of the headache associated with pituitary tumours. Cephalalgia 2003; 23: 621. Martinez-Salio A, Porta-Etessam J, Perez-Martinez D, Balseiro J, GutierrezRivas E. Chronic paroxysmal hemicrania-tic syndrome. Headache 2000; 40: 682–5. Massiou H, Launay JM, Levy C, El Amran M, Emperauger B, Bousser M-G. SUNCT syndrome in two patients with prolactinomas and bromocriptineinduced attacks. Neurology 2002; 58: 1698–9. Mateo I, Pascual J. Coexistence of chronic paroxysmal hemicrania and benign cough headache. Headache 1999; 39: 437–8. Matharu MS, Boes CJ, Goadsby PJ. Management of trigeminal autonomic cephalalgias and hemicrania continua. Drugs 2003a; 63: 1637–77. Matharu MS, Cohen AS, Frackowiak RSJ, Goadsby PJ. Posterior hypothalamic activation in paroxysmal hemicrania. Annals of Neurology 2006; 59: 535–45. Matharu MS, Cohen AS, McGonigle DJ, Ward N, Frackowiak RSJ, Goadsby PJ. Posterior hypothalamic and brainstem activation in hemicrania continua. Headache 2004; 44: 747–61. Matharu MS, Goadsby PJ. Post-traumatic chronic paroxysmal hemicrania (CPH) with aura. Neurology 2001; 56: 273–5. Matharu MS, Goadsby PJ. Bilateral paroxysmal hemicrania or bilateral paroxysmal cephalalgia, another novel indomethacin-responsive primary headache syndrome? Cephalalgia 2005; 25: 79–81. Paroxysmal hemicrania Matharu MS, Levy MJ, Merry RT, Goadsby PJ. SUNCT syndrome secondary to prolactinoma. Journal Neurol NeurosurgPsychiatry 2003b; 74: 1590–2. May A, Bahra A, Buchel C, Frackowiak RS, Goadsby PJ. Hypothalamic activation in cluster headache attacks. Lancet 1998; 352: 275–8. May A, Bahra A, Buchel C, Turner R, Goadsby PJ. Functional MRI in spontaneous attacks of SUNCT: short-lasting neuralgiform headache with conjunctival injection and tearing. Ann Neurol 1999; 46: 791–3. May A, Buchel C, Turner R, Goadsby PJ. MR-angiography in facial and other pain: neurovascular mechanisms of trigeminal sensation. J Cereb Blood Flow Metab 2001; 21: 1171–6. May A, Goadsby PJ. The trigeminovascular system in humans: pathophysiological implications for primary headache syndromes of the neural influences on the cerebral circulation. J Cere Blood Flow Metab 1999; 19: 115–27. Milos P, Havelius U, Hindfelt B. Cluster-like headache in a patient with a pituitary adenoma. With a review of the literature. Headache 1996; 36: 184–8. Mulder LJ, Spierings EL. Non-lateralized pain in a case of chronic paroxysmal hemicrania? Cephalalgia 2004; 24: 52–53. Negoro K, Kawai M, Tada Y, Ogasawara J, Misumi S, Morimatsu M. A case of postprandial cluster-like headache with prolactinoma: dramatic response to cabergoline. Headache 2005; 45: 604–6. Newman LC, Gordon ML, Lipton RB, Kanner R, Solomon S. Episodic paroxysmal hemicrania: two new cases and a literature review. Neurology 1992; 42: 964–66. Olesen J, Bousser MG, Diener HC, Dodick D, First M, Goadsby P, et al. New appendix criteria open for a broader concept of chronic migraine. Cephalalgia 2006; 26: 742–6. Ophoff RA, Terwindt GM, Vergouwe MN, van Eijk R, Oefner PJ, Hoffman SMG, et al. Familial hemiplegic migraine and episodic ataxia type-2 are caused by mutations in the Ca2+ channel gene CACNL1A4. Cell 1996; 87: 543–52. Paemeleire K, Bahra A, Evers S, Matharu MS, Goadsby PJ. Medicationoveruse headache in cluster headache patients. Neurology 2006; 67: 109–13. Pareja JA. Chronic paroxysmal hemicrania: dissociation of the pain and autonomic features. Headache 1995; 35: 111–3. Pareja JA, Sjaastad O. SUNCT syndrome. A clinical review. Headache 1997; 37: 195–202. Pascual J, Quijano J. A case of chronic paroxysmal hemicrania responding to subcutaneous sumatriptan. J Neurol Neurosurg Psychiatry 1998; 65: 407. Pollmann W, Pfaffenrath V. Chronic paroxysmal hemicrania: the first possible bilateral case. Cephalalgia 1986; 6: 55–7. Porta-Etessam J, Ramos-Carrasco A, Berbel-Garcia A, Martinez-Salio A, Benito-Leon J. Clusterlike headache as first manifestation of a prolactinoma. Headache 2001; 41: 723–5. Raskin NH. Headache. New York: Churchill-Livingstone; 1988. Brain (2008), 131, 1142^1155 1155 Russell D. Chronic paroxysmal hemicrania: severity, duration and time of occurrence of attacks. Cephalalgia 1984; 4: 53–6. Russell D, Storstein L. Chronic paroxysmal hemicrania: heart rate changes and ECG rhythm disturbances. A computerized analysis of 24h ambulatory ECG recordings. Cephalalgia 1984; 4: 135–44. Sano K, Mayanagi Y. Posteromedial hypothalamotomy in the treatment of violent, aggressive behaviour. Acta Neurochir Suppl (Wien) 1988; 44: 145–51. Sano K, Mayanagi Y, Sekino H, Ogashiwa M, Ishijima B. Results of stimulation and destruction of the posterior hypothalamus in man. J Neurosurg 1970; 33: 689–707. Sarov M, Valade D, Jublanc C, Ducros A. Chronic paroxysmal hemicrania in a patient with a macroprolactinoma. Cephalalgia 2006; 26: 738–41. Schvarcz JR, Driollet R, Rios E, Betti O. Stereotactic hypothalamotomy for behaviour disorders. J Neurol Neurosurg Psychiatry 1972; 35: 356–9. Sjaastad O. Cluster headache syndrome. London: W. B. Saunders; 1992. Sjaastad O, Bakketeig LS. The rare, unilateral headaches. Vaga study of headache epidemiology. J Headache Pain 2007; 8: 19–27. Sjaastad O, Dale I. Evidence for a new (?) treatable headache entity. Headache 1974; 14: 105–8. Sjaastad O, Dale I. A new (?) clinical headache entity ‘‘chronic paroxysmal hemicrania’’. Acta Neurologica Scandinavica 1976; 54: 140–59. Sjaastad O, Stovner LJ, Stolt-Nielsen A, Antonaci F, Fredriksen TA. CPH and hemicrania continua: requirements of high dose indomethacin dosages- an ominous sign? Headache 1995; 35: 363–7. Solomon S, Apfelbaum RI, Guglielmo KM. The cluster-tic syndrome and its surgical therapy. Cephalalgia 1985; 5: 83–9. Steiner TJ, Scher AI, Stewart WF, Kolodner K, Liberman J, Lipton RB. The prevalence and disability burden of adult migraine in England and their relationships to age, gender and ethnicity. Cephalalgia 2003; 23: 519–27. Stewart WF, Bigal ME, Kolodner K, Dowson A, Liberman JN, Lipton RB. Familial risk of migraine: variation by proband age at onset and headache severity. Neurology 2006; 66: 344–8. Torelli P, Manzoni GC. Pain and behaviour in cluster headache. A prospective study and review of the literature. Funct Neurol 2003; 18: 205–10. Vingen JV, Pareja JA, Stovner LJ. Quantitative evaluation of photophobia and phonophobia in cluster headache. Cephalalgia 1998; 18: 250–6. Wilkinson SM, Becker WJ, Heine JA. Opiate use to control bowel motility may induce chronic daily headache in patients with migraine. Headache 2001; 41: 303–9. Zanchin G, Dainese F, Mainardi F, Mampreso E, Perin C, Maggioni F. Osmophobia in primary headaches. J Headache Pain 2005; 6: 213–5. Zidverc-Trajkovic J, Pavlovic A, Mijajlovic M, Jovanovic Z, Sternic N, Kostic V. Cluster headache and paroxysmal hemicrania: differential diagnosis. Cephalalgia 2005; 25: 244–8. Zukerman E, Peres MFP, Kaup AO, Monzillo PH, Costa AR. Chronic paroxysmal hemicrania-tic syndrome. Neurology 2000; 54: 1524–6.