Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
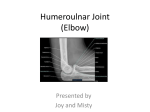
n tips & techniques Section Editor: Steven F. Harwin, MD Supine Extensile Approach to the Anterolateral Humerus Michael A. Kuhne, MD; Darin Friess, MD Abstract: The radial nerve is at risk of injury during surgical approaches to the humeral shaft. Previous authors have described an anterolateral approach to the humerus limited by the radial nerve, requiring that distal dissection be carried anterior into a neurovascularly crowded interval. A novel extensile approach is described using a neuromuscular bridge to protect the radial nerve, thus enabling safe distal extension of the anterolateral humerus approach. The authors present a case series of 7 patients who required an extensile humeral exposure. To date, there have been no complications, including loss of reduction, malunion, nonunion, or nerve palsy. [Orthopedics. 2016; 39(1):e193-e195.] T he knowledge of extensile extremity approaches is a useful tool in the armamentarium of the orthopedic surgeon. To date, there are few descriptions in the literature of extensile approaches to the entire humerus. This novel approach to the anterolateral humerus provides protection of the radial nerve while allowing exposure of the entirety of the anterolateral border of the humerus and for extended plating to achieve adequate screw pur- The authors are from the Naval Hospital Camp Lejeune (MAK), Camp Lejeune, North Carolina; and the Department of Orthopaedics & Rehabilitation (DF), Oregon Health & Science University, Portland, Oregon. Dr Kuhne has no relevant financial relationships to disclose. Dr Friess is a paid consultant for Accumed, LLC. Correspondence should be addressed to: Darin Friess, MD, Department of Orthopaedics & Rehabilitation, Oregon Health & Science University, 3181 SW Sam Jackson Park Rd, OP-31, Portland, OR 97239 (friessd@ohsu. edu). Received: June 10, 2014; Accepted: November 14, 2014. doi: 10.3928/01477447-20151222-17 chase and plate stability. Strong distal fixation in a potentially short distal segment is possible with this technique due to the large medial-lateral bony diameter. The technique described is a combination of an anterolateral humeral approach1,2 with bridging to a lateral elbow (Kocher3) approach distally. If necessary, the approach may be extended proximally into a deltopectoral approach, which has been previously described in the literature.1,2 Iatrogenic injury to the radial nerve occurs in 5% of cases of humeral open reduction and internal fixation.2 Campbell’s text describes an anterolateral humerus approach that must terminate 5 cm proximal to the elbow due to the presence of the radial nerve.4 Gerwin et al5 described an extensile posterior approach to the humerus and performed a cadaveric study mapping the course of the radial nerve. Based on the results of this study, the radial nerve crosses the lateral intermuscular septum at 10.2±0.4 cm proximal to the lateral epicondyle. With a modified posterior approach, the authors reported exposure of 94% of the distal humerus,5 but this approach requires a lateral or supine position, which is not always possible. In his text on extensile exposures, Henry1 described an anterolateral approach with splitting of the brachialis and coursing anterior on the elbow to protect the radial nerve. This limits the exposure of the lateral border of the distal humerus, thus exposing a more anterior approach than described here, and also risks denervation in splitting the brachialis despite its dual nerve innervation (radial nerve and musculocutaneous nerve). Mekhail et al6 described an extensile anterolateral approach requiring exposure of the radial nerve with the dissection traveling anterior to the brachioradialis to expose the distal humerus. JANUARY/FEBRUARY 2016 | Volume 39 • Number 1e193 n tips & techniques Figure 1: The proximal (shoulder, left) portion of the anterolateral approach was carried distally (elbow, right) to the extent of the mobile wad (hemostat identifies radial nerve). Figure 2: With the distal Kocher interval opened, a Cobb elevator was slid subperiosteally under the mobile wad and radial nerve. Left is proximal at the shoulder and right is distal to the elbow. The approach described in the current study allows for lateral humeral plating and exposure of the entirety of the humerus, while protecting the radial nerve. The authors’ experience using this technique in 7 patients requiring extensile humeral exposure for open reduction and internal fixation is reported. Materials and Methods Institutional review board approval for chart review was obtained for patients requiring extensile anterolateral humeral exposure for open reduction and internal fixation from January 1, 2006, to December 1, 2010, by a single surgeon (D.F.) at the authors’ e194 level I tertiary care trauma center. Chart review was performed in accordance with ethical standards for experiments on human subjects. Surgical Technique Preoperative patient management is a crucial part of the surgical preparation. The authors recommend against using a preoperative nerve block or skeletal relaxation for control of intraoperative pain to allow intraoperative testing of muscle and nerve function with electrical stimulation such as electrocautery. Surgeon and patient discussion of the risks of the operative intervention, including infection, damage to the radial and musculocutaneous nerves, fracture nonunion or malunion, and loss of fixation, is important. Patients were placed supine with the operative arm extended on a radiolucent arm board. Patients were prepped and draped in sterile fashion with the entire arm prepped free for intraoperative manipulation. Adhesive covering (Ioban; 3M, St Paul, Minnesota) was used to seal the proximal portion of the drapes. Anatomic landmarks, including the coracoid, deltopectoral groove, lateral bicipital sulcus, and lateral epicondyle, were marked. The incision ran proximally along the border of the biceps and the brachialis. It was carried distally to the lateral epicondyle, extending a few centimeters distal along Kocher’s interval. Beginning with the proximal exposure, the deltopectoral groove was identified (Figure 1). The cephalic vein was often mobilized laterally with the deltoid. After incision of the brachial fascia, the biceps was mobilized laterally, exposing the interval between the biceps and the brachialis. Prior to reduction and plating, the anterior insertion of the deltoid may need to be released.7 Care was taken to preserve the lateral brachial cutaneous nerve superficial to the biceps muscle. The musculocutaneous nerve was retracted medially with the biceps. The brachialis was split longitudinally due to its internervous interval and bluntly dissected to bone.7 The dissection was extended distally until visualization of the forearm extensor musculature (mobile wad) coursing obliquely. This marked the distal safe interval, as the mobile wad houses the radial nerve. The radial nerve is located approximately 10 cm proximal to the lateral epicondyle.5 Bovie electrocautery could be used toward the distal aspect of the proximal portion of this approach and muscular contraction may be observed near the nerve. However, this does not take the place of the surgeon’s knowledge of anatomy and cautious dissection principles. At this point, the dissection started distally at the lateral epicondyle. The proximal portion of the Kocher interval between the anconeus and extensor carpi ulnaris was developed. It was only necessary to develop the proximal portion because dissection to the forearm was unnecessary for the approach.3 Once at the distal humerus, a Cobb elevator was meticulously slid along the humerus subperiosteally from proximal to distal and from distal to proximal, thus providing 2 windows with a soft tissue bridge housing the radial nerve, mobile wad, and part of the brachialis (Figure 2). A large fragment 4.5-mm plate of appropriate length for the fixation of the intended fracture (typically 10 to 14 holes) was chosen. The authors typically chose a narrow plate for primary fracture Copyright © SLACK Incorporated n tips & techniques fixation and a broad plate for revision fixation. The plate was contoured with a slight pre-bend at the shaft and with a distal flare to accommodate the supracondylar region, using a table-top bender. The plate was then slid underneath the forearm extensor musculature along the lateral humerus. At least 2 or 3 screw holes of the plate distal to the neuromuscular bridge were available for screw fixation traversing the large lateral to medial diameter of the distal humerus. One or 2 holes generally remained underneath the muscular bridge that were not accessible with retraction and would have risked damage to the radial nerve (Figure 3). Once fixation was complete, the wound was thoroughly irrigated and closed in standard fashion per surgeon preference. The skin was then closed over a drain. Results Seven patients in whom this technique was used were identified via chart review. Four patients were indicated due to complications from an initial open reduction and internal fixation: 3 had fracture nonunion (Figure 4) and 1 sustained a periprosthetic fracture. Two patients had nonunion after attempted treatment in a Sarmientotype brace. One patient had a long-spiral humeral fracture indicated for primary open reduction and internal fixation. Among these 7 patients, there has been no evidence of nerve injury to date. Postoperatively, 1 patient developed a superficial infected hematoma requiring unplanned return to the operating room for irrigation and debridement. Discussion Using an anterolateral humerus approach combined with a Kocher elbow approach, an extensile humeral exposure appeared to be a safe procedure without evidence of radial nerve injury in this case series. A muscular bridge protecting the radial nerve was maintained during internal fixation. Caution must be used in nonunion cases with prior hardware, as scar tissue may make delineation of the muscular planes more difficult, thus putting the radial nerve at greater risk. The authors’ results are limited by the small case series; a larger number of patients are required to determine the true incidence of potential nerve injury with this approach. Conclusion Indications for operative fixation of the humerus, especially an extensile approach, are limited. Optimal candidates are those with humeral shaft nonunions, malunions, fractures surrounding a prior humerus implant with a prior anterolateral approach, and a long fracture pattern that would not be amenable to other forms of treatment and obese or polytraumatized patients who cannot lie lateral or prone for an extensile posterior approach. With proper patient selection, this novel approach enables safe distal Figure 3: Completed plate fixation of a right humeral shaft nonunion with 2 windows of the extensile approach, with the shoulder to the left and the elbow to the right. A B Figure 4: Prior to revision surgery, nonunion occurred after failed open reduction and internal fixation (A). Postoperative radiograph of the same patient using the extensile approach described (B). extension of the anterolateral humerus approach with good outcome. References 1. Henry AK. Exposures in the upper limb. In: Henry AK, ed. Extensile Exposure. 2nd ed. Baltimore, MD: Williams and Wilkins; 1963:25-48. 2. Robinson D, O’Brien P. Humeral shaft fractures: open reduction internal fixation. In: Wiss D, ed. Master Techniques in Orthopaedic Surgery: Fractures. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:67-80. 3. Ring D. Radial head fractures: open reduction internal fixation. In: Wiss D, ed. Master Techniques in Orthopaedic Surgery: Fractures. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:121141. 4.Crenshaw A. Surgical techniques and approaches. In: Canale ST, Beaty JH, eds. Campbell’s Operative Orthopaedics. 11th ed. Philadelphia, PA: Mosby Elsevier; 2008:100103. 5.Gerwin M, Hotchkiss RN, Weiland AJ. Alternative operative exposures of the posterior aspect of the humeral diaphysis with reference to the radial nerve. J Bone Joint Surg Am. 1996; 78(11):1690-1695. 6.Mekhail AO, Checroun AJ, Ebraheim NA, Jackson WT, Yeasting RA. Extensile approach to the anterolateral surface of the humerus and the radial nerve. J Shoulder Elbow Surg. 1999; 8(2):112-118. 7. Morrey BF. Humerus. In: Morrey BF, Morrey MC, eds. Master Techniques in Orthopaedic Surgery: Relevant Surgical Exposures. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:91-104. JANUARY/FEBRUARY 2016 | Volume 39 • Number 1e195