Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
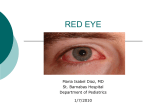
AD_HTT_39_46___JUN11_04 7/6/04 9:06 AM Page 39 How to Treat pull-out section read online @ www.australiandoctor.com.au You can now earn CPD points with How to Treat by completing quizzes online (www.australiandoctor.com.au/cpd) or in every issue. See page 46 for details and this week’s quiz. INSIDE Anatomy and function Signs and symptoms Examination techniques Common conjunctival conditions Case studies The authors Dr Matthew Oliva, Corneal Fellow, Royal Victorian Eye and Ear Hospital, Melbourne. Conjunctival Professor Hugh Taylor AC, professor of ophthalmology, University of Melbourne; director, Centre for Eye Research Australia, Royal Victorian Eye and Ear Hospital, Melbourne. conditions Overview OCULAR surface problems are one of the most common reasons patients seek medical care. However, medical training often invests little time preparing the GP for the wide variety of eye problems encountered in clinical practice. Many ocular symptoms are non-specific and many clinical entities can lead to inflammation of the conjunctiva and the presentation of a ‘red eye’. While most conjunctival conditions are benign, some presentations may herald vision-threatening or, rarely, life-threatening conditions. For these reasons it is important for GPs to have a solid framework of knowledge to help them distinguish between common self-limiting conditions, such as conjunctivitis, and vision-threatening entities requiring prompt referral, such as corneal ulcers and angleclosure glaucoma. This review of conjunctival problems emphasises diagnostic clues, suggested treatments and referral criteria. Some causes of a red eye, such as blepharitis and pterygium, are beyond the scope of this article, as are conditions such as neonatal conjunctivitis. www.australiandoctor.com.au 11 June 2004 | Australian Doctor | 39 AD_HTT_39_46___JUN11_04 7/6/04 9:06 AM Page 41 Anatomy and function THE conjunctiva is a thin, translucent, mucous membrane-lined sac covering the anterior portion of the globe and the undersurfaces of the eyelids. It protects the eye, allows unrestricted movement, contributes products to the tear film and provides a source of immune and antimicrobial agents to protect the ocular surface. The conjunctiva extends from the upper and lower eyelid margins onto the back surface of the eyelid (palpebral portion), into the fornix (forniceal portion), onto the surface of the globe (bulbar portion), and up to the corneoscleral limbus Figure 1: Diagram of the medial conjunctiva showing the plica semilunaris. Punctum lacrimale Plica semilunaris Caruncula Punctum lacrimale Opening of tarsal glands The plica semilunaris is a vertical fold of conjunctiva located in the medial portion of the bulbar conjunctiva. It may represent a remnant of the nictitating membrane found in some animals, such as cats (figure 1). The conjunctiva, corneal and intraocular structures derive their blood supply from terminal branches of the ophthalmic artery. Hyperaemia of the bulbar conjunctiva and a red eye is the hallmark of inflammatory processes of the conjunctiva. Inflammation of the superficial conjunctival vessels, which tend to increase in size away from the (limbal portion). The stratified squamous and columnar conjunctival mucosal surface undergoes transition from keratinised skin at the eyelid margin, into corneal epithelium at the corneoscleral limbus. The tarsal conjunctiva is tightly adherent to the tarsal plate of the upper and lower lids. The forniceal portions of the conjunctiva serve as tear reservoirs. Special regions of the conjunctiva include the caruncle and the plica semilunaris. The caruncle is located in the medical canthus and contains dermal structures such as hair follicles and sebaceous glands. limbus, must be differentiated from inflammation of the deeper vessels supplying the sclera and the thin connective tissue layer between the conjunctiva and the sclera, known as the episclera. These vessels dilate with inflammation of the cornea, iris, ciliary body and sclera. When there is inflammation of the conjunctival and episcleral vessels, white sclera can still be visualised deep to the redness. The conjunctiva is rich in lymphatic networks. These join the lymphatics of the eyelids and drain medially to the submandibular lymph node and laterally to the pre-auricular lymph node system. Signs and symptoms A CAREFUL history is important in diagnosing conjunctival conditions and will significantly narrow the differential diagnosis before examination begins (see box). The first impression you have of the patient is critical in guiding effective history-taking. Pay particular attention to their age, occupational risk factors and the context of the presentation. Symptoms not to miss Pain Pain can be difficult to assess given its subjective nature. Most conjunctival lesions typically produce only mild-tomoderate discomfort. Descriptions of mild burning, stinging, itching, scratchiness, aching or foreign body sensation are all common complaints and are typically caused by ocular surface disturbances. In the patient who describes moderate-to-severe pain, consider causes such as corneal abrasions or ulcers, uveitis, scleritis, angle-closure glaucoma or, less commonly, orbital processes such as orbital cellulitis or pseudotumour. As a general guideline, a patient with severe pain should warrant investigation for a process not involving the conjunctiva alone. Important symptoms and associated ocular conditions Key history points Pain Onset and duration — is the condition acute or chronic in nature? Symptoms lasting more than four weeks are chronic, while those occurring in the previous 12 hours are hyperacute. Laterality — is the condition monocular or binocular? Did it begin in one eye and then spread to the other? Course — is the condition improving or worsening, or does it wax and wane? Is it associated with seasonal variations? Social history — is there any recent contact with children or adults with a red eye? Is there a history of long-term sun exposure (pterygium and pingueculae)? Some patients may need to be asked specifically about their sexual history, including current or prior genital tract infection with, or exposure to, sexually transmitted infections (gonococcal and chlamydial conjunctivitis). Occupational history — does the patient work in a situation that may predispose to trauma or allow environmental exposures to irritants or allergens such as dust, wind, smoke or chemicals? Past medical history and review of systems — has the patient had a recent upper respiratory illness? Systemic malignancies, dermatological conditions and inflammatory disorders such as sarcoidosis and lupus can manifest as ophthalmic conditions. Pay special attention to immune status, autoimmune diseases, prior head and neck pathology, thyroid conditions, history of allergy, and coagulation status. Ophthalmic history — does the patient wear contact lenses? Is there a history of intra- or extra-ocular surgery, including eyelid surgery? Has there been any prior radiation treatment to the orbital region? Medications — many systemic medications may have ocular side effects, such as antihistamines causing dryness. Document all topical ocular medications and their actual frequency and duration of use. Pay special attention to over-the-counter medicines such as ‘get the red out’ medicines, tear substitutes and contact lens solutions. Itching Loss of vision Relieved with topical anaesthetic Corneal abrasion, corneal ulcer, severe dry eye Mild Blepharitis, viral or bacterial conjunctivitis, dry eye, mild allergic eye disease Not relieved with topical anaesthetic Scleritis, orbital process, anterior uveitis, angle-closure glaucoma Severe Allergic or atopic keratoconjunctivitis, vernal keratoconjunctivitis Discharge Corneal processes Microbial keratitis (ulcer), severe dry eye, abrasions Mucopurulent Bacterial conjunctivitis Watery (serous) Viral conjunctivitis Intraocular processes Uveitis, cataract, retinal pathology, optic neuropathies, acute glaucoma Stringy Allergic conjunctivitis Orbital processes Optic neuropathies, orbital tumours, orbital infections Cortical processes Brain tumours, stroke Visual disturbance Another important question to ask the patient is whether vision has been affected. It is critical to determine whether an intraocular process is manifesting as an external inflammation or if there is involvement of the cornea, which may also cause a visual disturbance. Conjunctivitis unaccompanied by a corneal process or intraocular inflammation usually does not affect visual acuity. If acuity is decreased, the GP must assume corneal involvement or an intraocular process such as iritis or acute angle-closure glaucoma and refer to a collabo- Guidelines for immediate referral Severe ocular pain. ■ Any visual deficit associated with an inflamed eye. ■ Any corneal infiltrate or hypopyon. ■ Any unilateral red eye associated with nausea and/or vomiting. ■ rating ophthalmologist. Discharge If an infectious cause is suspected, ask about the presence and type of discharge. In the acute setting, a history of the eyelids being stuck closed in the morning, with greenish or yellow discharge that adheres to the lashes and lid margins and requires a washcloth to clean them, is usually indicative of bacterial conjunctivitis. A more watery discharge, with or without stringy mucus, is more suggestive of a viral or allergic cause. Itching Itching is a hallmark of allergic eye disease, although patients sometimes complain of mild itching with dry eyes, blepharitis and acute conjunctivitis. Itching should provide a clue to the GP to inquire further regarding allergies. Examination techniques BASIC equipment should include a near and distance acuity chart, pinhole, handheld light source, topical anaesthetic drops, fluorescein drops, litmus paper and a magnifying device such as a slit lamp, loupes or direct ophthalmoscope. Visual acuity Measure acuity in each eye separately with appropriate correction, or pinhole testing. Observation Notice the patient’s level of hygiene and their body habitus, looking for signs of an underlying disorder such as Cushingoid features and any abnormal habits (such as chronic eye rubbing). Also, look for any signs of systemic conditions that may affect the conjunctiva, such as rheumatoid arthritis. Head and neck examination Avoid the urge to focus attention immediately on the eye itself. Search for any pre-auricular or submandibular lymphadenopathy, especially in patients suspected of having viral conjunctivitis. Perform a complete cranial nerve exam with specific focus on cranial nerves II, III, IV, V and VII. Nerve palsies may predispose to conjunctival conditions from poor lid closure or diminished corneal sensation. Skin examination Look for chronic skin conditions such as rosacea and atopic disease. A rash or cold sore in the distribution of the fifth cranial nerve could suggest active herpes simplex or zoster disease. An acute rash could be evidence of contact dermatitis. and nasolacrimal duct area for masses as well as for areas of tenderness and warmth. Pupil examination Lid examination Abnormalities in upper or lower eyelid structure or function may predispose to conjunctival conditions. Ask the patient to gently close their eyes. Any lid malposition that allows a show of sclera could be evidence of clinically significant corneal exposure. Look for ectropion and entropion. Also evaluate the spontaneous blink rate, which should average one blink per 5-10 seconds, which may be decreased in neurodegenerative disorders such as Parkinson’s disease. Palpate the lids, lacrimal glands www.australiandoctor.com.au A fixed large pupil in the setting of a red painful eye may indicate angleclosure glaucoma. A small pupil suggests uveitis. Conjunctival examination One drop of topical anaesthetic in each eye often helps patient comfort and facilitates examination. If the topical anaesthetic rapidly reduces symptoms, an ocular surface aetiology can be assumed. A thorough examination of the conjunctiva can be facilitated by pulling down the lower lid to examine the inferior fornix. The presence of follicles (viral process) or papillae (bacterial or allergic condition) should be noted. Similarly, the upper lid can be everted to display the tarsal conjunctiva and to search for foreign bodies in the superior fornix. Try to assess the pattern of redness by distinguishing which layer of the ocular surface is inflamed. Fluorescein dye can highlight any disruption of the conjunctival or corneal epithelium, such as with an abrasion, chemical burn or corneal ulcer. Ocular examination If a slit lamp is available, the anterior chamber should be assessed for cells and flare — the critical finding in diagnosing an anterior uveitis. 11 June 2004 | Australian Doctor | 41 AD_HTT_39_46___JUN11_04 7/6/04 9:06 AM Page 42 how to treat - conjunctival conditions Common conjunctival conditions Subconjunctival haemorrhage SUBCONJUNCTIVAL haemorrhage (figure 2) is a common cause of acute ocular redness. The bleeding vessel causes a well-circumscribed area of bright-red blood underneath the conjunctiva, which obscures the view of the sclera. The condition is unilateral and of sudden onset. The adjacent conjunctiva is non-injected, pain is absent and visual acuity is unaffected. Figure 2: Subconjunctival haemorrhage. What not to miss A careful history for antecedent factors should include inquiries about trauma, bleeding disorders, anticoagulation treatments, hypertension, prolonged coughing or vomiting episodes, or vigorous Valsalva manoeuvers. Often no explanation for the haemorrhage will be discovered. Figure 3: Bacterial conjunctivitis. Treatment No treatment is necessary and the patient should be advised that resolution will occur gradually over 2-3 weeks. If the haemorrhage fails to resolve, the patient should be referred to an ophthalmologist. Conjunctivitis Conjunctivitis is probably the most common ocular condition presenting to the GP. Conjunctivitis refers to the non-specific dilation of the superficial conjunctival vessels and may be associated with oedema of the conjunctiva (chemosis) or discharge. Conjunctivitis is not typically associated with severe pain or visual disturbance. Discerning the correct aetiology and treatment often revolves around taking a careful clinical history. Figure 4: Gonococcal conjunctivitis. Viral conjunctivitis The conjunctiva is the most commonly infected part of the eye and almost all infectious conjunctivitis is due to viral infection. The typical clinical history is of a recent URTI or contact with someone with a red eye. The infection typically starts in one eye and is followed a few days later with involvement of the contralateral eye. Viral conjunctivitis is most often caused by adenoviral infection and may be part of an epidemic. At times, adenoviral conjunctivitis can be very severe. Signs and symptoms. Patients may complain of redness, watery discharge or a burning irritation, but pain or visual disturbance is usually absent. Examination findings may include conjunctival redness, oedema, inferior fornix follicles and, rarely, pinpoint haemorrhages. Lid swelling is often present. The spectrum of presentation ranges from mild to severe. A palpable pre-auricular or submandibular lymph node is highly supportive of the diagnosis but is not always present. If the diagnosis is uncertain, a viral PCR swab of the inferior fornix can be taken to identify adenoviral DNA. Treatment. Viral conjunctivitis is typically self-limiting in nature and there is no substantial evidence that commonly used topical antibiotics or antiviral treatments improve outcomes. In clinical practice, topical antibiotics are often prescribed with the belief that bacterial superinfection is prevented or because patients do not readily accept a decision not to treat any presumed infection without antibiotics. Supportive treatment should be instituted with tear substitutes and cool compresses to the eyelids as needed for patient comfort. Patients often experience a worsening in their symptoms for the first 4-7 days after onset, and symptoms may not resolve for 2-3 weeks. Small subsets of patients develop sterile inflammatory corneal infiltrates, which can be visualised as small white opacities in the cornea and typically require a slit lamp to diagnose. These patients experience a prolonged disease course, often requiring steroid treatment. Hygiene. Patients require counselling about the highly infectious nature of the virus for a two-week period after the appearance of symptoms. They should avoid close contact, touching their eyes, sharing towels or washcloths, preparing foods, shaking hands, and swimming in communal pools. Patients may require up to two weeks away from work or school, depending on the severity of their symptoms and the risk of transmission. This advice is important to prevent outbreaks and should always be given. Frequent hand-washing is mandatory. Any surfaces touched during the examination, the examination room and any instruments should be decontaminated with topical alcohol. When to refer. Patients should be reviewed in 10-14 days, or earlier if their symptoms worsen. Severe cases and those with corneal involvement (keratitis) should be referred to an ophthalmologist for consideration of steroid treatment. Figure 5: Chlamydial conjunctivitis. Figure 6: Episcleritis. Chlamydial inclusion conjunctivitis Chlamydial infection can cause both trachoma (serotypes A-C) and inclusion conjunctivitis (serotypes D-K) (figure 5). Trachoma is a leading cause of blindness worldwide and is still endemic in Aboriginal communities in SA, WA, and the NT. In urban environments, chlamydial inclusion disease is an important cause of conjunctivitis. It is an ocular manifestation of a systemic STI and often causes chronic symptoms. Signs and symptoms. Chlaymdial disease should be strongly considered in chronic conjunctivitis but may also have an acute presentation. Patients complain of unilateral or bilateral redness, irritation and a stringy mucoid discharge. Patients are typically young and sexually active. The eye is mildly injected. The inferior fornix and superior tarsal conjunctiva will show a characteristic follicular response that can be appreciated by everting the upper lid or pulling down the lower lid. Lymphadenopathy may be present. The cornea is rarely involved. A swab of the conjunctiva for PCR to Bacterial conjunctivitis Bacterial conjunctivitis (figure 3) typically develops abruptly. Like viral conjunctivitis, it usually begins in one eye but may spread to the contralateral eye in 1-2 days. Unlike viral conjunctivitis, a mucopurulent discharge is often present, with mucoid inflammatory debris present in the inferior fornix and crusting along the eyelash base. Common infective organisms include Streptococcus pneumoniae and Staphylococcus aureus as well as gram-negative organisms such as Haemophilus influenzae, especially in children, the elderly and debilitated patients. Signs and Symptoms. Patients typically complain of redness, tearing and irritation, but not pain. Examination shows diffuse redness of the conjunctival vessels and debris in the inferior fornix. Lymphadenopathy is typically absent. The cornea may have mild punctate staining with fluorescein, which may decrease vision slightly to the 6/7.5-6/9 range. Treatment. Almost all cases of acute bacterial conjunctivitis are of limited 42 | Australian Doctor | 11 June 2004 duration, even without specific therapy. With effective topical treatment, both the morbidity and duration of disease are reduced. Treatment consists of a broadspectrum antibiotic such as topical chloramphenicol (0.5%) qid, which provides excellent coverage of the most common pathogens. Newer fluoroquinolone antibiotics should be reserved for unresponsive or severe keratitis. Conjunctival swabs for culture are not warranted except for severe cases and those that fail to respond to treatment. When to refer. Patients should be reviewed in two days initially and then every 3-5 days until infection resolves. Severe cases, clinical worsening, corneal involvement, infections in contact-lens wearers, a history of recent eye surgery, or lack of improvement within one week warrant prompt referral. What not to miss. Severe hyperacute bacterial conjunctivitis with an abrupt onset within 24 hours of initial discomfort is often associated with gonococcal infection in sexually active individuals. This infection is characterised by a copious purulent discharge, a bright-red, severely inflamed conjunctiva (figure 4), conjunctival papillae, marked lid swelling and tenderness, and lymphadenopathy. There is often a membrane of inflammatory material overlying the tarsal conjunctiva. Immediate referral to an ophthalmologist is required because gonococcal bacteria have the ability to penetrate the cornea and rapidly cause visual loss. Conjunctival swabs are mandatory, followed by the initiation of topical broad-spectrum antibiotics such as a fluoroquinolone (ciprofloxacin, one drop hourly) in addition to systemic treatment with a broad-spectrum antibiotic such as ceftriaxone (1g IM daily for five days) A thorough sexual history should be taken, with appropriate followup and treatment of sexual partners arranged. www.australiandoctor.com.au detect the chlamydial antigen can be used to confirm the diagnosis. Treatment. Patients require a workup for evidence of systemic infection, including urethritis, vaginitis, or cervicitis. It is essential that sexual partners be identified and treated promptly. Treatment is with oral antibiotics such as azithromycin (Zithromax) (1g orally). Topical antibiotics and steroid treatments are ineffective and will not treat the underlying systemic disease. When to refer. Refer in severe cases or when the diagnosis is in doubt. Episcleritis Episcleritis (figure 6) is a relatively benign self-limiting condition, presumed to be an autoimmune process. It most often affects women aged 20-50. Signs and symptoms Episcleritis generally has an acute onset and is characterised by a mild ache and focal areas of redness. Vision is normal and the patient may be asymptomatic. Examination shows a focal, nonraised, often well-defined patch of dilated episcleral vessels with underlying unaffected sclera. The condition may be confused with an inflamed pterygium. Treatment Patients should be reassured that the condition does not threaten vision and should clear in several weeks. Prescription of an oral NSAID often assists with symptoms and may speed resolution. Artificial tears can also be prescribed for comfort. When to refer Episcleritis that persists, worsens or frequently recurs should be referred. Topical corticosteroids may be considered by an ophthalmologist to speed resolution. Scleritis Scleritis is not simply a more severe form of episcleritis. These two conditions are quite distinct. Scleritis is often associated with an underlying connective tissue disease (most commonly rheumatoid arthritis). Infectious scleritis, typically with Gram-negative bacteria, may occur after beta irradiation after pterygium removal (figure 7). This can occur many years after the original surgery in avascular portions of sclera. Signs and symptoms Patients complain of moderate to severe deep ocular pain, tearing and photophobia. The eye may be exquisitely tender to palpation. There is often fiery or brick-red inflammation of the sclera, episclera and conjunctiva that can be localised or diffuse. The underlying sclera may exhibit a bluish discoloration. The conjunctival blood vessels can be seen overlying the deeper inflammation. Management Patients should be referred promptly to an ophthalmologist, who may investigate with a systemic workup. Treatment typically involves systemic corticosteroids or other forms of immune suppression. Patients are often co-managed AD_HTT_39_46___JUN11_04 7/6/04 9:06 AM by the GP or a rheumatologist as well as the ophthalmologist. Infectious scleritis requires systemic antibiotic treatment. Dry-eye syndrome A stable film of tears is required to maintain a healthy ocular surface. Dry eye is typically associated with a deficiency in aqueous tear production, known as keratoconjunctivitis sicca (KCS). Other causes such as meibomian gland dysfunction from blepharitis, or mechanical eyelid problems such as ectropion causing corneal exposure, must also be considered. Dry eye may also be associated with systemic immune dysfunction from diseases such as rheumatoid arthritis and Sjögren’s syndrome. Dry eyes are common in postmenopausal women and can be exacerbated by HRT. Drugs such as tricyclic antidepressants, beta blockers, oral contraceptives and antihistamines can also exacerbate dryness. Signs and symptoms Patients often complain of bilateral constant and disabling eye burning, foreign-body sensation, redness or having “tired” eyes. Paradoxically, some experience copious reflex tearing and may complain of watery eyes. Patients with Sjögren’s syndrome have concurrent dry mouth symptoms. Similar symptoms may also occur after work and reading in those with inadequately corrected presbyopia. A new pair of reading glasses can often help those in their 40s or 50s with symptoms. Signs of dryness include a decreased tear film height or increased mucus production in the inferior fornix. Tear film height is best evaluated at a slit lamp, where the tear meniscus normally measures 0.5mm above the lower eyelid margin. Punctate staining of the conjunctiva and the cornea in the interpalpebral zone with either Rose Bengal or fluorescein dye can be commonly seen (figure 8). Treatment Tear supplements are available as drops, ointments or gels and should be started. Most older lubricating drops (Murine or Tears Naturale) contain preservatives that can be toxic to the ocular surface, particularly with often and prolonged use. Newer products with less toxic preservatives (GenTeal or Polytears), unpreserved Murine or Tears Naturale, or single-dose lubricants (Cellufresh or Celluvisc) are recommended if prescribed more than four times a day. Medications that contribute to dryness should be discontinued and patients should be counselled to avoid dry or windy environments. Any concurrent blepharitis should be treated. A severe dry mouth or systemic signs of rheumatological disease should prompt investigation of serological inflammatory markers to look for systemic disease. When to refer Patient who are refractory to treatment and require excessive Page 43 amounts of lubricants should be referred. Temporary or permanent occlusion of the lacrimal puncti is often performed by an ophthalmologist, who will also perform tests to quantify tear production. Figure 7: Infectious scleritis after beta irradiation for pterygium. steroid-sparing systemic treatments may also be indicated. Recently, topical cyclosporin has shown promise as a steroid-sparing agent for severe allergic eye disease. Toxic conjunctivitis (figure 10) Allergy The eye is a frequent target of inflammation in both local and systemic allergic reactions, with the conjunctiva most often involved. There are several types of allergic conjunctivitis. Figure 8: Dry eye stained with Rose Bengal dye. Seasonal allergic conjunctivitis The most common form of ocular allergy, this condition is a type I (IgE-mediated) hypersensitivity response to environmental allergens such as pollen, dust or animal dander. It is often associated with allergic rhinitis and may be associated with eczema or asthma. Seasonal recurrences are most frequent in the spring and summer (figure 9). Signs and symptoms. Patients complain of itching, watery or stringy discharge, seasonal recurrences, tearing and nasal discharge and typically have a history of allergies or atopy. Critical signs include bilateral red and oedematous eyelids, conjunctival oedema and tarsal conjunctival papillae. Vision is unaffected and lymphadenopathy is absent. Treatment. Efforts should be made to determine and eliminate the inciting allergen. Cool compresses and topical artificial tear substitutes will often provide symptomatic relief. Topical antihistamines such as levocabastine 0.5% (Livostin) are useful to limit itching. Mast-cell stabilisers such as lodoxamide 0.1% (Lomide) can also be useful for allergy prophylaxis but require up to two weeks of continued treatment to gain an effect. Newer medications such as olopatadine 0.1% (Patanol) that combine an antihistamine and a mast-cell stabiliser are highly effective. Oral antihistamines have little benefit for ocular symptoms and may exacerbate a concomitant dry eye. What not to miss. Atopic keratoconjunctivitis is a sight-threatening allergic eye disease in people with severe atopic skin disease. The skin and lids are always affected, often being thickened, erythematous and fissured. Patients are often chronic eye-rubbers. Untreated cases can lead to longterm corneal vascularisation and scarring. Patients should be referred early to an allergist as well as an ophthalmologist. Vernal keratoconjunctivitis, which can have a seasonal component, occurs most often in male children. It is characterised by severe redness of the eye, vascularisation of the cornea and corneal ulcers. The condition often resolves in the teenage years. When to refer. Severe seasonal allergic eye disease and cases of atopic keratoconjunctivitis should be referred to an ophthalmologist. Topical steroids and mast-cell stabilisers are typically needed to control more severe ocular allergy. Systemic immune suppression with oral corticosteroids or other Figure 9: Seasonal allergic conjunctivitis. Figure 10: Toxic conjunctivitis. Figure 11: Conjunctival foreign body. Conjunctival redness may be caused by numerous environmental factors, including smoke, smog or chemical fumes, wind and ultraviolet radiation. Topical medications such as over-the-counter vasoconstrictors, tear substitutes and glaucoma medications, especially those with preservatives, can damage ocular surface cells and inhibit function. Cosmetic and hair-care products and contact lens solutions can also cause ocular surface toxicity. Signs and symptoms. Take a careful history for use of topical ocular medications or cosmetics, as these are the most common offenders and can be easily overlooked. Irritation, tearing, redness, itching, burning and aching eyes are common complaints. Multiple punctate lesions of the corneal surface that stain with fluoroscein dye are common but may require the use of a slit lamp to visualise. Erythema and swelling of the lids may be present. Treatment. Avoiding or minimising exposure is the best remedy. Tear substitutes, especially those without preservatives, can be prescribed for symptomatic relief. What not to miss. Patients often treat redness with topical vasoconstrictor medicines such as naphazoline to “get the red out”. These can lead to rebound vasodilation, requiring a pattern of escalating frequency of use and resultant surface toxicity. The repetitive longterm use of these agents should be strongly discouraged. The frequent application of topical anaesthetics is highly toxic to the eye. Anaesthetics should not be prescribed to patients and should only be used to facilitate examination. Trauma Oral antihistamines have little benefit for ocular symptoms and may exacerbate a concomitant dry eye. Superficial injuries to the conjunctiva are common and usually heal rapidly. Common injuries include metallic foreign bodies from hammering or drilling, glass particles from shattered spectacles, damage from sticks or debris while gardening, or from assault, and chemical splash injuries. Although superficial conjunctival epithelial injury usually resolves within 24 hours, a thorough examination is imperative to look for penetrating eye injuries or retained foreign bodies. Chemical injuries are an ocular emergency. Conjunctival foreign bodies and lacerations Signs and symptoms. A conjunctival foreign body causes unilateral irritation, redness and tearing. A decrease in vision, a distorted pupil or shallowing of the anterior chamber should raise suspicion of a penetrating injury (figure 11). Examination techniques. After applying topical anaesthetic, the fornices should be carefully examined. The upper lid should be everted to facilitate examination of the superior fornix. A cotton bud www.australiandoctor.com.au can be used to sweep the fornices for any unseen foreign body. Fluorescein should be applied and the cornea examined for foreign bodies. Treatment. Superficial conjunctival foreign bodies can be irrigated away, wiped away with a cotton bud or lifted from the conjunctiva with the tip of a 25-gauge needle. If the epithelium of the conjunctiva has been disrupted, such as with a conjunctival laceration, a broad-spectrum antibiotic such as chloramphenicol should be administered qid until the epithelium has healed. Patching is not required. When to refer. Any suspicion of a retained foreign body or penetrating injury necessitates prompt referral. What not to miss. A CT scan or X-ray may be indicated if there is any concern about a retained foreign body. Chemical injury Acute chemical burns with alkali and acid can permanently damage the ocular surface function and constitute an ophthalmic emergency. Splash injuries can occur at work, in the home from household cleaning chemicals, or from assault. They are often bilateral. The extent of injury and ultimate outcome depends on the pH of the chemical, the degree of exposure, and the timing and quality of the initial treatment. Alkaline injuries tend to penetrate tissues more deeply than acidic injuries and traditionally fare worse. Signs and symptoms. There is acute onset of pain, redness, tearing and photophobia. Vision is often decreased if the cornea has been involved. After eye irrigation, assess the degree of corneal and conjunctival epithelial loss with fluorescein staining, and the clarity of the cornea. Treatment. The most vital aspect of treatment is immediate and thorough irrigation of the eye. This cannot be overemphasised and is hard to overdo. Litmus paper should be placed in the inferior fornix to document normalisation of pH, and pH should be retested five minutes after stopping the irrigation. Irrigation should continue for 10 minutes and several litres of fluid should be used. Remove any particulate matter from the conjunctival fornices with forceps. When to refer. Small corneal or conjunctival epithelial defects can be safely treated with a topical antibiotic such as chloromycetin until the epithelium has healed. Any injury that involves large portions of the ocular surface, crosses the limbus, reduces corneal clarity, or has retained particulate matter requires immediate referral and possible hospital admission. What not to miss. Beware of complete corneal epithelial defects, which may be difficult to appreciate with fluorescein staining because of lack of a normal-toabnormal transition zone. Large splash injuries (cement mixing or spray injuries at close range with any type of chemical) can cause a complete loss of the epithelium. cont’d next page 11 June 2004 | Australian Doctor | 43 AD_HTT_39_46___JUN11_04 7/6/04 9:07 AM Page 44 how to treat - conjunctival conditions Summary Eye conditions in general, and conjunctival conditions in particular, are common reasons patients visit their GP. Many of the conditions reviewed above are selflimiting. Take-home points: ■ Viral conjunctivitis is highly contagious and appropriate hygiene measures should be taken; ■ Never prescribe a topical anaesthetic; ■ Topical corticosteroids should be prescribed in rare instances only; ■ ■ Topical fluoroquinolone use should be reserved for severe corneal infections; Refer promptly cases in which there is an inflamed eye with decreased visual acuity, a corneal infiltrate or severe pain. Evidence base for treatment of bacterial conjunctivitis* Evidence for the benefit of treatment of culturepositive bacterial conjunctivitis ■ One systematic review has found that antibiotics (polymyxin-bacitracin, ciprofloxacin or ofloxacin) increase rates of clinical and microbiological cure, compared with placebo; ■ Four RCTs comparing use of antibiotics for culturepositive bacterial conjunctivitis found no significant difference among antibiotics in clinical or microbiological cure. Evidence for the benefit of empirical treatment of suspected bacterial conjunctivitis ■ One systematic review found limited evidence from one RCT that topical norfloxacin increased rates of clinical and microbiological improvement or cure after five days compared with placebo. ■ RCTs comparing different topical antibiotics have found no significant difference in rates of clinical or microbiological cure. *Source: Smith J. Bacterial conjunctivitis. Clinical Evidence Concise 2003; 131. from previous page Figure 14: Conjunctival lymphoma. Figure 15: Conjunctival intraepithelial neoplasia. Immediately on presentation the eye should be irrigated with copious quantities of tap water or sterile saline if available. Irrigation must continue until the return of the pH to normal (7.0). Tumours Conjunctival tumours can be divided into lymphoid, epithelial, and pigmented categories. The overall incidence of primary conjunctival malignancy is relatively low, and metastatic lesions to the conjunctiva are rare. de novo during or after middle age are suspicious of malignancy (primaryacquired melanosis). Be especially wary of new pigmented lesions in fairskinned people. These should always be referred to an ophthalmologist for possible biopsy. Conjunctival naevus Conjunctival naevi are benign neoplasms, most commonly on the bulbar conjunctiva, and typically they develop during puberty. They are usually flat, well demarcated, mobile and can be heavily pigmented or amelanotic (figure 13). The degree of pigmentation may fluctuate with time and the naevus may enlarge, especially during puberty. Only rarely does a naevus malignantly transform into a melanoma. Treatment. A baseline photograph should be taken and yearly reviews conducted to monitor for growth. Patients should be advised to return for examination earlier if there is any change in the size or colour of the lesion. When to refer. Flat brown patches of conjunctival pigmentation that arise Conjunctival lymphoma Figure 13: Conjunctival naevus. Lymphoid tumors of the conjunctiva are rare (<1/100,000) and occur on a spectrum from benign lymphoid hyperplasia to lymphoma. Patients are typically young to middle aged. Signs and symptoms. Patients are usually asymptomatic, but the patient or a relative may notice the enlarging mass. A unilateral, salmon-coloured diffuse mass is present in the subconjunctival space (figure 14). Treatment. An excisional biopsy is performed by the ophthalmologist, and immunohistochemical studies initiated. An oncologist typically conducts a workup for any systemic lymphoma. Local radiotherapy may be used if malignancy is suspected. Conjunctival intraepithelial neoplasia Squamous neoplasms of the conjunctiva are associated with excessive sun exposure. They are typically slow growing and locally invasive, only rarely causing metastatic disease. Previous terms for this include Bowen’s disease, dysplasia and carcinoma in situ. Signs and symptoms. Patients often complain of an enlarging mass on their eye, which may cause irritation or blurred vision. On examination a gelatinous, raised vascular mass is present that is typically grey-white in colour. It most often originates at the limbus and may have a ‘stuck-on’ appearance. At other times the changes are more plaque-like (figure 15). Treatment. Early referral is warranted to confirm the diagnosis. The tumour is typically cured by simple excision. Diffuse lesions may require supplemental topical antimetabolite treatments with agents such as Mitomycin C. Author’s case study JIM, 42, presents to his GP complaining of eye redness, irritation, mild photophobia and a watery discharge in both eyes for three days. He has had symptoms of a viral respiratory infection for the last week. His symptoms began in the right eye and were followed by left eye involvement two days later. He thinks several people at his work may have had “pink eye” recently. There is no relevant social or sexual history. On examination, vision is 6/6 in each eye and each eye appears as in figure 16. There is mild lid swelling of both upper eyelids, and follicles are noted on the inferior tarsal conjunctiva. A tender right pre-auricular lymph node is palpated. Acknowledgements: National Eye Institute web site: www.nei.nih.gov | Australian Doctor | 11 June 2004 two weeks later. He notes the redness, discharge and irritation in both eyes has significantly improved. However, he complains of a slow deterioration in his visual acuity in the past few days and that some light sensitivity and mild foreign-body sensation persist. On examination, vision in each eye is now 6/9. The conjunctiva appears quiet and there is minimal follic- MR M, a 45-year-old engineer, presented to a country doctor with an acutely “itchy, painful, sore right eye”. The country doctor recognised there was something of concern and correctly referred him to an ophthalmologist. For practitioners For patients Comment The GP correctly diagnoses a viral conjunctivitis. Jim is prescribed topical artificial tears qid for symptomatic relief, as well as cold compresses. He is counselled regarding the infectious nature of viral conjunctivitis and the need for careful hygiene, and advised that the disease is selflimiting and should slowly resolve over the next two weeks. Jim returns for follow-up Case study Online resources Wills Eye Manual. Rhee, 1999: http://pco.ovid.com/lrppco/ index.html Gills, JP. Ophthalmology. eMedicine, Inc., 2000: www.emedicine.com/oph/ index.shtml to viral conjunctivitis. A mild topical steroid (fluoromethalone 0.1% [Flarex, Flucon, FML] qid both eyes) is prescribed and slowly tapered over the next few months. Jim’s vision returns to normal and the infiltrates resolve. Figure 17: Subepithelial infiltrates in viral conjunctivitis. Figure 16: Viral conjunctivitis. ular reaction in each fornix. Slit-lamp examination reveals several round, white subepithelial opacities in the central cornea of each eye (figure 17). There is no staining with flourescein dye. Jim is referred to a collaborating ophthalmologist. He is seen by the ophthalmologist and diagnosed with decreased vision from subepithelial infiltrates secondary Almost all viral conjunctivitis resolves without adverse sequelae. Fewer than 10% of patients develop an immunological reaction to residual viral particles in the cornea, resulting in the development of sterile corneal lymphocytic infiltrates 2-4 weeks after the onset of infection. Any persistent decrease in vision after viral conjunctivitis should prompt referral. GP’s contribution All photos generously supplied by Medical Photography Imaging Centre, Royal Victorian Eye and Ear Hospital, Melbourne. 44 Figure 12: Alkaline burn. Ocular emergency — chemical burns (figure 12) nosed by the ophthalmologist as having iritis. Is there any link between iritis and allergy? No. Is iritis something that runs in the family? It is typically sporadic. DR JEREMY THOMSON Fairlight, NSW From his presenting complaint, what diagnosis first comes to mind? Trauma and infection are the primary concerns, given the complaint of pain. Mr M had a strong family history of glaucoma, and a grandfather had iritis. He had a past and current history of asthma and hay fever. Mr M was diagwww.australiandoctor.com.au I had thought that an itchy eye generally meant allergy. Is this true? Can itch be a symptom of iritis or any other significant eye condition? Itching (usually bilateral) is the hallmark of all types of allergic eye disease. Patients sometimes complain of mild itching with conjunctivitis, blepharitis or dry eye. Iritis usually presents with redness, discomfort, and photophobia, and itching would be atypical. If the country doctor had no access to an ophthalmologist, would it be appropriate to prescribe steroid drops and, if so, what should Mr M be careful of? The diagnosis of iritis requires a slit lamp examination to check for inflammatory cells in the anterior chamber. If the diagnosis is confirmed, steroid drops should be started. Steroids can elevate intraocular pressure, predispose to infection and increase the risk of cataract formation in the long term. Mr M had no history of any medical or arthritic conditions apart from cont’d page 46 AD_HTT_39_46___JUN11_04 7/6/04 9:07 AM Page 46 how to treat - conjunctival conditions from page 44 some backache. The ophthalmologist ordered extensive blood tests, which were all normal. Mr M was treated with steroids orally and as eye drops, and recovered fully. Is it normal practice to prescribe oral steroids for iritis? Most iritis can be controlled with intensive topical steroids. If this fails, oral steroids or local steroid injections are typically added. A backache in the context of iritis could be suggestive of ankylosing spondylitis, and radiographs should be ordered. A year later Mr M presented again with possible iritis. The doctor referred him to an ophthalmologist, who diagnosed “anterior uveitis and episcleritis”. Two years later Mr M had similar symptoms but this time slit-lamp examination was normal. What is the difference in the terms iritis, uveitis and scleritis? Do they share similar pathologies and treatments? Is it important for GPs to differentiate between them? Uveitis is a general term describing inflammation anywhere along the uveal tract (choroid, ciliary body or iris). Iritis is a type of uveitis implying the ocular inflammation is confined to the anterior segment of the eye. Scleritis is an inflammatory condition of the sclera that is typically severe and associated with either infection or a systemic inflammatory condition. It can occur with or without a coexisting uveitis. Differentiating and treating types of uveitis and scleritis requires advanced examination techniques and is difficult in general practice. Steroids may help symptoms of viral conjunctivitis but can also prolong the disease course and enhance viral replication. bilateral necessitates a workup for an associated systemic condition. About half the time (different studies vary considerably) a systemic condition will be found, most commonly an HLA-B27 associated spondyloarthropathy. wind. Mild steroid eye drops can then be added for unresponsive patients on a shortterm basis. Long-term steroid use necessitates monitoring by an eye care provider for side effects (such as high intraocular pressure). General questions for the author Is there a role for mild steroid drops for viral conjunctivitis? Which are the best drops to use for symptomatic relief? Cold compresses and tear substitutes often help with symptom relief. Steroids may help symptoms but can also prolong the course of the disease and may enhance viral replication. Steroids are not typically used except for severe cases. I fairly often prescribe FML eye drops for allergic conjunctivitis and for eye irritation due to pterygia. I realise this is not without some risks. What would you suggest as a good approach to these common conditions? In both conditions treatment should start with lubricating eye drops for symptomatic relief. A trial of topical mast-cell stabilisers and/or antihistamines should be added for allergic conjunctivitis. Pterygium patients should try to avoid excessive UV exposure and What percentage of patients with iritis will have, or develop, another immune disorder? Iritis that is recurrent or When a corneal foreign body has been removed, is it imperative to completely get rid of any rust stain that is not close to the pupil? Attempts should be made to remove all the rust because it will incite a significant inflammatory response in the cornea and delay recovery. A smallgauge needle, spatula or electric burr can be used to remove residual rust. Patients who think they have conjunctivitis often come back from the chemist with Bleph10 eye drops. Is chloromycetin a superior treatment? There is no literature comparing the two. Chloromycetin may be better tolerated by the patient and have a wider spectrum of antibiotic activity. In a child with an URTI, otitis media and conjunctivitis for which I am going to prescribe oral antibiotics, should I also prescribe chloromycetin drops? If bacterial conjunctivitis is suspected, chloromycetin drops should be added. Australian Doctor How To Treat CPD amount of watery discharge and minimal lid swelling . . . . . . . . . . . . . . . . . . . . . . . . . .❏ Instructions Earn 2 CPD points by completing this quiz online or on the attached card. Mark your answers on the card and drop in the post (no stamp required) or fax to (02) 9422 2844. For immediate feedback click the ‘Earn CPD pts’ link at www.australiandoctor.com.au Note that some questions have more than one correct answer. The mark required for CPD points is 80%. Your CPD activity will be updated on your RACGP records every January, April, July and October. 1. Jan, 43, has been aware of a red eye for one day. If the redness is caused by a condition affecting the conjunctiva, which TWO statements are most likely to be true? a) You would not expect to see hyperaemia of the bulbar conjunctiva . . . . . . . . . . . . . . . . ❏ b) You would expect to see inflammation of the superficial conjunctival vessels, which tend to increase in size away from the limbus . . . .❏ c) You would expect to see white sclera beneath if there was redness of the eye caused by inflammation of the conjunctiva . . . . . .❏ d) You may find lymphadenopathy affecting the occipital nodes . . . . . . . . . . . . . . . . . . . .❏ 2. In taking Jane’s history, which ONE factor is the least likely to help you establish the diagnosis? a) Her past medical history . . . . . . . . . . . .❏ b) Her ophthalmic history, such as the use of contact lenses . . . . . . . . . . . . . . . . . . . . .❏ c) Details of current and recent medications . . . . . . . . . . . . . . . . . . . . . . .❏ d) Her psychiatric history . . . . . . . . . . . . .❏ 3. When assessing Jane’s symptoms, which ONE statement is correct? a) If she has pain relieved by a topical anaesthetic, scleritis is a probable cause of her symptoms . . . . . . . . . . . . . . . . . . . . . . . .❏ b) If a topical anaesthetic does not relieve her pain, anterior uveitis is a probable cause of her symptoms . . . . . . . . . . . . . . . . . . . . . . . .❏ c) If she has severe itch, blepharitis is a probable cause of her symptoms . . . . . . .❏ 46 d) If she has mild itch, vernal keratoconjunctivitis is a probable cause of her symptoms . . . . . . . . . . . . . . . . . . . . . . . .❏ 4. When you examine Jane you notice conjunctival inflammation, and a macular rash with several vesicles affecting the eyelid. With regard to her rash, which ONE statement is least likely to be true? a) If she has herpes zoster ophthalmicus, she would probably give a history of a flu-like prodromal illness for about one week . . . .❏ b) If her rash is due to contact dermatitis, topical creams such as cosmetic products or sunscreen are unlikely causes . . . . . . . . .❏ c) If she has herpes zoster ophthalmicus, she is at risk of serious corneal complications and may require antiviral or steroid therapy . . .❏ d) If her symptoms are caused by rosacea, she is at risk of other ocular conditions such as conjunctivitis, blepharitis and chalazion . . .❏ 5. Diane, 36, complains of redness affecting one eye for a day. When considering the possible causes, which ONE statement is correct? a) If the redness is caused by a subconjunctival haemorrhage, you would expect her eye to be painful . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ b) If she has viral conjunctivitis you would expect both eyes to be red at this stage . .❏ c) If she has a bacterial conjunctivitis you would expect her to have a mucopurulent discharge . . . . . . . . . . . . . . . . . . . . . . . .❏ d) If the redness is due to a gonococcal infection, you would expect her to have a small 6. You diagnose viral conjunctivitis and treat her appropriately. She recovers but sees you two months later with discomfort in her left eye, which she thinks may be the start of the same problem. On examination, you note a patch of dilated episcleral vessels and consider she may have episcleritis. If this diagnosis is correct, which ONE statement is true? a) Episcleritis occurs more often in women over 50 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ b) If she has episcleritis, you would expect her visual acuity to be reduced to about 6/9 . .❏ c) If she has episcleritis, NSAIDs may improve her symptoms . . . . . . . . . . . . . . . . . . . . .❏ d) If she has episcleritis, you can reassure her that her symptoms will improve over the next 2-3 days . . . . . . . . . . . . . . . . . . . . . . . . .❏ 7. You see her again in a year. Now she complains of deep pain in the left eye, with watering and some mild photophobia. You are concerned that she may have scleritis. Which THREE features in her history, examination and investigation would support your diagnosis? a) A history of rheumatoid arthritis . . . . . .❏ b) The absence of tenderness on palpation of the eye . . . . . . . . . . . . . . . . . . . . . . . . . .❏ c) A history of previous pterygium treated with beta irradiation . . . . . . . . . . . . . . . . . . . . .❏ d) A bluish discoloration of the sclera beneath redness involving the episclera and conjunctiva . . . . . . . . . . . . . . . . . . . . . . .❏ 8. John, 62, has a history of asthma and allergic rhinitis. His work involves regular exposure to fumes. His main complaint is of watery itchy eyes. Which ONE of the following statements about his possible diagnoses is correct? a) When you find that he has enlarged preauricular nodes, you think he is most likely to have allergic conjunctivitis . . . . . . . . . . . .❏ b) When you notice marked thickening of the skin on his eyelids and constant eye-rubbing, you think he may have atopic keratoconjunctivitis . . . . . . . . . . . . . . . . .❏ c) You suspect seasonal allergic conjunctivitis, and so would expect this episode to respond quickly to treatment with a mast-cell stabiliser . . . . . . . . . . . . . . . . . . . . . . . . .❏ d) You explain that if he has toxic conjunctivitis he will need to use a topical vasoconstrictor on a regular ongoing basis . . . . . . . . . . . . . .❏ 9. You treat him for seasonal allergic conjunctivitis. He returns in two weeks and says his symptoms are worsening. If your diagnosis is correct, which TWO factors are most likely to have contributed to delay in his recovery? a) He has been using the same type of lubricating drops he has used intermittently for the past 15 years . . . . . . . . . . . . . . . . . . .❏ b) He has been regularly using artificial tears to lubricate the eyes . . . . . . . . . . . . . . . . . . .❏ c) He has been using an oral antihistamine regularly . . . . . . . . . . . . . . . . . . . . . . . . .❏ d) He has been using antihistamine drops . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ 10. John returns to your surgery a year later in distress. He has been working at home changing a battery and has acid burns to his face and eyes. Which TWO of the following statements regarding your treatment are most likely to be correct? a) You thoroughly irrigate his eye for 10 minutes using several litres of fluid, then pH test the eye five minutes after stopping the irrigation . .❏ b) You explain to him that acid injuries to the eye tend to be more severe than alkaline injuries . . . . . . . . . . . . . . . . . . . . . . . . . .❏ c) You use fluorescein to confidently exclude all significant epithelial defects . . . . . . . . . . .❏ d) If you see a small defect on fluorescein testing, you can safely treat him with a topical antibiotic such as chloromycetin, and review him regularly until the epithelium has healed . . . . . . . . . . . . . . . . . . . . . . . . . . .❏ HOW TO TREAT NEXT WEEK Editor: Dr Lynn Buglar Co-ordinator: Julian McAllan The next How to Treat enumerates the latest screening procedures and risk assessments of preconception health care. The author, Dr Lesley Cotterell, is a GP and medical educator with a special interest in reproductive health. | Australian Doctor | 11 June 2004 www.australiandoctor.com.au AD_HTT_39_46___JUN11_04 7/6/04 9:07 AM Page 47 AUSTRALIAN DOCTOR LAUNCHES Australian Doctor Education is a new three-tiered education and information package that brings together for the first time the relevance and user-friendliness of How to Treat — Australian Doctor's best-read section — with the freedom and convenience of web-based CPD programs, plus an authoritative series of seminars backed by some of Australia's most prestigious universities. 1 CPD in Australian Doctor Using the authority, relevance and popularity of How to Treat as a platform, Australian Doctor readers can earn 2 CPD points a week by answering a quiz on that week's How to Treat topic. Conveniently, entries can be made either online at Australian Doctor's new-look web site (www.australiandoctor.com.au or direct at www.australiandoctor.com.au/cpd) or manually on a reply-paid card inside the newspaper. Doctors will receive a certificate recording their participation. 2 3 Australian Doctor Seminars How to Treat Yearbook You asked for it, and we've delivered it — every How to Treat from the past 12 months, covering some of the most common clinical management challenges presenting to GPs, all redesigned to a handy A4 format and bound in a 600-page book. Published with a cover price of $99, the book will be sent free to GPs who correctly answer two week's worth of Australian Doctor CPD quizzes online, while stocks last. In association with the University of Sydney's Coppleson Committee for Continuing Medical Education and other leading educational institutions, Australian Doctor is proud to introduce a series of full-day seminars addressing some of the most complex and rapidly developing areas in general practice. To be held initially in Sydney and Melbourne in September and October this year, the lectures will be delivered by some of the country's most renowned experts in their field. Details of the first conference on paediatrics will be announced soon. If you would like to be sent details, e-mail [email protected] Check out... our CPD page at Australian Doctor's new-look web site, which now also features: www.australiandoctor.com.au • FASTER ACCESS to Australian Doctor's content, story archive and resources. • LINKS to clinical and patient resources from a broad range of local and overseas institutions. • AN IMPROVED SEARCH engine of all content and past stories, going back further than alternative sites. PLUS a search across our entire medical database. www.australiandoctor.com.au 11 June 2004 | Australian Doctor | 47