Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
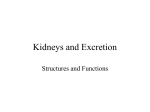
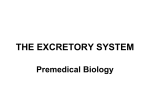
The Renal System David Carroll [email protected] https://www.davidontheinter.net Learning Objectives What you need to pass your exam Anatomy Physiology Pharmacology Pathophysiology Renal Anatomy Renal Anatomy • Each kidney has outer cortex and inner medulla. • Urine is formed within functional subunits known as nephrons. Renal Anatomy • Each kidney has outer cortex and inner medulla. • Urine is formed within functional subunits known as nephrons. • Each nephron contains a glomerulus, consisting of a tuft of capillaries with an afferent and efferent arteriole. • The glomerulus is surrounded by epithelium of the Bowman’s capsule. • Glomerulus and Bowman’s capsule form renal corpuscle. Renal Anatomy • This initial filtrate is then modified by a variety of secretory and reabsorptive processes as it passes through: 1. Proximal convoluted tubule 2. Loop of Henle 3. Distal convoluted tubule 4. Collecting duct • The glomeruli and convoluted tubules lie within outer cortex and loop of Henle and collecting duct extend into medullary region. • End product, urine, is delivered via renal pelvis to ureter. What does the kidney do? Removal of waste products Maintenance of fluids & electrolytes Acid-base balance What does the kidney do? Endocrine functions: 1. Blood pressure – Renin-angiotensin-aldosterone system 2. Haemoglobin – Erythropoeitin 3. Calcium & phosphate– Vitamin D activation The Nephron Functional unit of the kidney (1,000,000) Made up of: Responsible for urine formation - Afferent and Efferent arterioles - Glomerulus - Proximal Tubule - Loop of Henle - Distal Tubule - Collecting Duct Functions of the Nephron Filtration Reabsorption Secretion Excretion Filtration Kidneys alone receive approximately 25% of cardiac output (sv X hr) Cells, proteins, and other large molecules are filtered out of the glomerulus (driven by Starling forces) by a process of ultrafiltration, leaving an ultrafiltrate that resembles plasma (except that the ultrafiltrate has negligible plasma proteins) to enter Bowman's space. Reabsorption Active Transport (requires ATP) – Na+, K+ ATP pumps Passive Transport – Na+ symporters (glucose, amino acids, etc) – Na+ antiporters (H+) – Ion channels – Osmosis Reabsorption Proximal tubule - reabsorbs 65 % of filtered Na+ as well as Cl-, Ca2+, PO4, HCO3-. 75-90% of H20. Glucose, carbohydrates, amino acids, and small proteins are also reabsorbed here Loop of Henle - reabsorbs 25% of filtered Na+. Descending loop impermeable to only water. Distal tubule - reabsorbs 10% of filtered Na+ and reabsorbs HCO3Collecting duct - reabsorbs the remaining 2% of Na+ only if the hormone aldosterone is present. H20 depending on hormone ADH Secretion Proximal tubule – uric acid, bile salts, metabolites, some drugs, some creatinine Distal tubule – Most active secretion takes place here including organic acids, K+, H+ and drugs Regulation of Fluids & Electrolytes Fluid balance is the concept of homeostasis, that the amount of fluid lost is equal to the amount taken in. Euvolaemia is the state of normal body fluid volume. The major source of fluid loss is urine. Fluid loss is regulated in the kidney hormonally. Largely through RAAS and ADH. Regulation of Fluids & Electrolytes Na+ in particular is the major driving force of fluid shifts in the body – it maintains ECF volume. Therefore it is hugely important to maintain an appropriate Na+ balance. + 99% of Na filtered in the glomerulus is reabsorbed. Transport proteins in the renal tubule mediate Na+ reabsorption. Na+ concentration gradient along the tubule allows sodium to + move into tubule cells. The gradient is maintained by the Na / K+ ATPase pump. Renin Secreted in response to renal hypoperfusion from juxta-glomerular apparatus – macula densa Converts of angiotensinogen to angiotensin I Direct Effects Vasodilatation of afferent arteriole + Direct Na loss Aldosterone High [K+] or low [Na+] stimulates the secretion of aldosterone from adrenal cortex Acts on DCT causing reabsorption of Na+ & water increasing ECF and increases blood pressure Final [K+] controlled in collecting duct by aldosterone, when aldosterone is absent, no K+ is excreted in the urine (Only means by which K+ is secreted) Since water is passively reabsorbed down the osmotic gradient generated by Na+ transport, water reabsorption is also affected. This means that while it affects ECF volume it has little effect on ECF [Na+], since reabsorbed Na+ is followed by a proportionate amount of water. Anti - Diuretic Hormone Secreted from posterior pituitary Secretion is ↑ if: 1. ↑ osmolality (ECF) 2. ↓ volume 3. ↓ atrial pressure Promotes water reabsorption in the distal convoluted tubule and collecting duct Also known as vasopressin – a direct vasoconstrictor Acid Base Regulation • H+ levels are regulated through two buffering systems: – Chemical buffers – binds to H+ e.g. Bicarbonate buffering system – Physiological buffer – controls excretion of acids or bases (kidneys) or volatile acids (lungs) • Bicarbonate buffering system: – CO2 + H2O H2CO3 H+ + HCO3- • The kidney acts as a physiological buffer: – When pH is low excess H+ ions are secreted in the tubules via the Na+/H+ exchanger and more bicarbonate is reabsorbed. – When pH is high less bicarbonate is reabsorbed. Assessment of renal function Measure waste products of protein metabolism - Measurement of plasma [urea] and [creatinine] Creatinine clearance = UV/P • U=urinary [creatinine] • V= urinary output in 24 hours • P= plasma [creatinine] Glomerular Filtration Rate Normal values are: 90-110 ml/min 80-125ml/min In clinical practice an estimated GFR (eGFR) is provided based on: - Plasma [creatinine] Age Gender Ethnicity Renal Pharmacology Loop Diuretics MOA: Na/K/2Cl co-transporter blocker Indications: oedema e.g. HF, resistant hypertension Cautions: can worsen gout, diabetes Contra-indications: hypok+, anuria Side effects: postural hypotension, hypok+, hypona+, hypomg+ Thiazide Diuretics MOA: inhibit Na reabsorption in DCT Indications: Hypertension, heart failure Cautions: can worsen gout, diabetes NOT IN PREGNANCY Side effects: postural hypotension, hypok+ , hypona+, hypomg+, hyperca2+, gout (hyperuricaemia) Potassium Sparing MOA: aldosterone receptor antagonist Indications: oedema/ascites from liver cirrhosis, heart failure, primary hyperaldosteronism Cautions: look out for hyperk+ Contra-indications: hyperk+, Addison’s disease Side effects: gynacomastia, testicular atrophy, menstrual disorders, alopecia, hirsutism Drugs that make kidneys sad Should be avoided in renal failure e.g. NSAIDs, ACE-I, ARBs, aminoglycosides, large doses of penicillins, ciclophosphamide, ciclosporine A, gold, penicillamine What are the general principles of prescribing in renal failure? • Reduced dose and/or increase the dosage interval according to renal function, especially with drugs which have a small therapeutic index • Base changes on measures of renal function i.e. glomerular filtration rate, serum creatinine • Use plasma levels if possible – digoxin, gentamicin, ciclosporin. • Avoid drugs which are nephrotoxic Pathophysiology Urinary Tract Infections Causes: Typically E. Coli (also Proteus, Klebsiella, Staph e.g. epidermidis) Risk Factors: • Gender (ascending infectionshorter urethra in females) • Stasis of urine (eg renal calculi, reflux, tumours) • Medical plastic (catheters) P/C: Symptoms: Lower UTI (cystitis & urtheritis)frequency, urgency, dysuria Upper UTI (pyelonephritis)- as above plus fever, loin pain, rigors Ix: • Pre-treatment MSSU for microscopy & culture. Urine dipstick • May need structural /functional imaging to rule of reflux & renal scarring if UTIs recurrent Acute Kidney Injury Acute Kidney Injury (AKI) is common, expensive to manage, prolongs hospitalization and is associated with increased mortality AKI is defined by an acute reduction in kidney function as identified by an increase in the serum creatinine and reduction in urine output. Symptoms: Anorexia, nausea & vomiting Pruritis Confusion, reduced consciousness Acute Kidney Injury Pre-Renal • • Volume depletion • Dehydration • Blood loss Hypotension • Sepsis • Medications • Cardiac failure Renal Post-Renal • Acute Tubular Injury • Bladder outlet obstruction • Interstitial nephritis • • Glomeruloneph ritis Bilateral ureteric obstruction. • Obstruction of a single functioning kidney • Vasculitis “Hidden” causes of CKD Hypertension Infection Diabetes Drugs Kidney damage or reduced GFR for more than 3 months Exotica Nephritides • 70% cases caused by diabetes, hypertension and atherosclerosis. Chronic Kidney Disease Reduced GFR •Fluid retention – tissue oedema and heart failure •Reduced metabolite excretion – uraemia, increased lipids, increased plasma urate and [creatinine] Reduced tubular function •Reduced fluid reabsorption causing polyuria •Reduced K+ secretion resulting in hyperkalaemia •Reduced acid secretion resulting in metabolic acidosis Anaemia •Reduced erythropoietin production – normocytic normochromic anaemia Renal bone disease •Reduced vitamin D activation leads to decreased Ca2+ absorption from GIT •Plasma phosphate elevated due to reduced renal excretion and reduced calcium •Reduced levels of vitamin D and reduced calcium stimulate parathormone secretion hyperparathyroidism Cardiovascular complications hypertension •Activation of RAAS – increases PR •Fluid retention leading to heart failure atherosclerosis •Increased cholesterol secondary Management of CKD Renoprotection • Maintain normal BP and restrict proteinuria • Reducing angiotensin II activity – ACE inhibitors • Reducing BP – diuretics and calcium channel blockers • Manage other pathogenic conditions e.g. smoking, diabetes Treat complications • Anaemia - EPO • Hyperlipidaemia - statins • Hyperkalaemia – restrict intake • Acidosis – oral bicarbonate • Hyperphosphataemia – phosphate binders • Ostemomalacia & secondary hyperparathyroidism – activated vit D analogues Haemodialysis • Deals with waste products and fluid/electrolyte overload Acknowledgements All images available via Wikimedia Commons. Questions? Slides + supplementary notes will be online https://www.davidontheinter.net/notes/