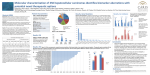
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
3rd Annual Association of Clinical Documentation Improvement Specialists Conference Inpatient Medicare Advantage: HCC Capture Through CDI Gloryanne Bryant, BS, RHIA, RHIT, CCS, CCDS Regional Managing Director of HIM NCAL Revenue Cycle Kaiser Foundation and Hospitals Goals/objectives • Provide an Overview of Hierarchical Condition Categories (HCC) and payment methodology • Learn the Similarities and Differences between MS-DRGs and HCCs • Understand the Documentation and Coding issues • Learn how to Incorporate MA into your CDI program and processes A little Medicare quiz #1 There are four types of Medicare coverage • True or False? #2 Medicare Advantage is also referred to as Medicare Risk, Medicare C, Medicare Managed Care • True or False? A little Medicare quiz #3 How many citizens were enrolled in Medicare in 2009? • 35 million, or 45 million, or 50 million, or 55 million #4 Medicare headquarters are in Washington, DC. True or False? #5 Of all Federal Government expenditures, Medicare is in the top 3. True or False? Medicare beneficiaries & chronic conditions Medicare • There are several types of Medicare Healthcare coverage: Medicare A, Medicare B, Medicare C, and Medicare D (or Rx plan). • Medicare Advantage is often referred to as MA, Medicare C, Medicare Risk, Medicare Capitation, and Managed Care. • 2009 it was reported that there were 45 million people on Medicare, with 22% of these being enrolled in private Medicare Advantage plan. Medicare Advantage plan enrollment 2009 Medicare Advantage enrollment Medicare Advantage (MA) model • To ensure a health-based risk assessment system, CMS monthly capitated payments need to take into consideration the severity of illness of the patient. • Diagnosis information is collected for each patient which will determine the payment for the following year. • The intended goal is to pay Health plans appropriately for the relative risk of their patients. • Promote fair payments and reward organizations for efficiency and excellent care for the chronically ill. What is Risk Adjustment? • Medicare Advantage adjusts their monthly per capita payments to Health Plans to take into account the relative health of their members; “Risk Adjustment.” • Health Plans receive less payment for healthier members/patients and more for sicker members. – The relative health or “risk adjustment factor” is based on diagnoses (coded data) submitted by the Health Plan in the prior year. – The “risk” score comes from the weight (assigned value) of the Hierarchical Condition Categories (HCC) 7 Reimbursement model from CMS Under CMS guidelines, providers are reimbursed based on that patient’s: • Membership/Patient – Age – Sex – Geographic Area • Risk for future healthcare costs • Each calendar year, based on diagnosis identified, documented, and coded (meeting the definition of a reportable condition) How does the model work? • CMS adjusts Medicare Advantage payments to private healthcare plans based on health expenditure risk of enrollees. • The “CMS-HCC model uses demographics and a diagnosis-based medical profile captured during all clinician encounters—both inpatient and outpatient—to produce a health-based measure of future medical need.” – Medical Care, Vol 43, Number 1, January 2005, pg. 34. • This methodology is used to calculate payments for Medicare managed care plans (Medicare Advantage or Medicare Part C). Why is this important to know? • The diagnoses captured predict the future care expenditures. • If we document, address, and capture/code these diagnoses: – Our patients receive better quality care – Clinical data represents the severity of our patients – Providers receive the appropriate reimbursement for the care we provide Sources of diagnostic information • Diagnosis information is collected from the following sources (continuum of care for the calendar year): – Hospital inpatient principal & secondary diagnoses (internal & external) – Hospital outpatient diagnoses (internal & external) – Physician diagnoses (internal & external) regardless of setting (e.g., could be from hospital rounding, SNF rounding, ICFs, Dialysis Centers, and home visits) – Diagnoses made by clinically trained non-physician providers (e.g., psychologists, podiatrists, nurse practitioners, physician assistants) • Although most Medicare Advantage diagnoses for HCCs are made in the ambulatory setting, there are some “specific” HCCs in the inpatient setting with opportunity. 15 ICD-9-CM and HCCs HCC list HCC Category Description • 1 HIV/AIDS See Appendix • 2 Septicemia/Shock • 5 Opportunistic Infections • 7 Metastatic Cancer and Acute Leukemia • 8 Lung Upper Digestive Tract and Other Severe Cancers • 9 Lymphatic Head and Neck Brain and Other Major Cancers • 10 Breast Prostate Colorectal and Other Cancers and Tumors • 15 Diabetes with Renal or Peripheral Circulatory Manifestation • 16 Diabetes with Neurologic or Other Specified Manifestation • 17 Diabetes with Acute Complications • 18 Diabetes with Ophthalmologic or Unspecified Manifestation • 19 Diabetes without Complication • 21 Protein-Calorie Malnutrition • 25 End-Stage Liver Disease • 26 Cirrhosis of Liver • 27 Chronic Hepatitis • 31 Intestinal Obstruction/Perforation • 32 Pancreatic Disease • 33 Inflammatory Bowel Disease • 37 Bone/Joint/Muscle Infections/Necrosis • 38 Rheumatoid Arthritis and Inflammatory Connective Tissue Disease • 44 Severe Hematological Disorders • 45 Disorders of Immunity51Drug/Alcohol Psychosis • 52 Drug/Alcohol Dependence54Schizophrenia • 55 Major Depressive Bipolar and Paranoid Disorders for Complete List of HCCs Hierarchical Condition Categories — related diseases • Hierarchies are established so that each patient is only paid for the most severe manifestation among related diseases. – For instance, ischemic heart disease diagnoses are organized in the Coronary Artery Disease (CAD) in the hierarchal category. • The CAD hierarchy consists of three Hierarchical Condition Categories (HCC) arranged in descending order by clinical severity and cost. – HCC 81 for Acute Myocardial Infarction (AMI) through HCC 83 for Coronary Atherosclerosis/Other Chronic Ischemic Heart Disease. – A patient with a diagnosis code in HCC 81 is excluded from the payment grouping in HCCs 82 and 83, even if these ICD-9-CM codes are present, as the hierarchy is applied. 18 Disease hierarchies • 33 of the 70 HCCs are in hierarchies: – Hierarchy: group of HCCs with same disease at sequential levels of severity (and costs) – Example: Diabetes = HCC 15, 16, 17, 18, 19 depending on type of complications – Purposes: • Diagnoses are clinically related and ranked by cost • Takes into account the cost of the lower HCCs reducing the need for coding proliferation – Risk factors within a hierarchy are additive; the highest “trumps” the lower conditions CMS Model Categories and Hierarchies (HCCs) — examples Diabetes 1) Diabetes w/Renal or Peripheral Circulatory Manifestation 2) Diabetes w/Neurologic or Other Specified Manifestation 3) Diabetes w/Acute Complications 4) Diabetes w/Ophthalmologic or Unspecified Manifestations 5) Diabetes w/o Complications Cancer 1) Metastasis Cancer & Acute Leukemia 2) Lung, Upper Digestive Tract, & Other Severe Cancers 3) Lymphatic, Head & Neck, Brain, & Other Cancers & Tumors 4) Breast, Prostate, Colorectal & Other Cancers & Tumors Kidney Disease 1) Dialysis Status 2) Renal Failure 3) Nephritis Vascular Disease 1) Vascular Disease w/Complications 2) Vascular Disease 3) Chronic Ulcer of Skin, Except pressure (decubitus) Hierarchical Condition Categories — unrelated diseases • For unrelated diseases, HCCs accumulate. – For instance, a patient with heart disease, stroke, and cancer will have three separate HCCs (payments) totaled together for the year. • The predicted cost will reflect increments for each of these three HCC categories. • This model also considers the fact that some diseases interact and that the predicted cost may be more than the sum of the separate increments. – For instance, the presence of both CHF and COPD leads to a higher cost than the predicted cost for the sum of these conditions. CMS calls this an “interaction term.” • To improve clinical validity and predictive accuracy, the interaction among common and high-cost chronic diseases was considered. – These include diabetes, cerebrovascular disease, vascular disease, COPD, CHF, and renal failure. 21 CMS reimbursement is based on the Hierarchical Condition Categories (HCC) – Providers are reimbursed based on the most severe diagnosis within each category. – Disease categories are accumulated — that is, reimbursements are based on the sum of all chronic conditions diagnosed in different hierarchical categories. Medicare Advantage HCC annual payment methodology — example RISK FACTOR No Risk Adjustment Factor Atrial Fibrillation CHF DM II W/ Diabetic CKD, Stage III $4,000.00 $4,000.00 $4,000.00 $4,000.00 $2,000.00 $2,000.00 $2,000.00 $2,000.00 $7,000.00 $7,000.00 $7,000.00 $4,000.00 $4,000.00 History of MI Base payment Age $4,000.00 History of MI Sepsis CHF DM II W/ Diabetic CKD, Stage III TOTAL ANNUAL REIMBURSEMENT $10,000.00 $4,000.00 $6,000.00 $13,000.00 $17,000.00 * Dollar amounts are rounded estimates and do not reflect actual reimbursement rates $27,000.00 Medicare Advantage HCC annual payment methodology — example (cont.) RISK FACTOR Age No Chronic Conditions Cancer Lung Metastatic Bone Cancer Protein Calorie Malnutrition (PCM) Pressure Ulcer, Hip $4,000.00 $4,000.00 $4,000.00 $4,000.00 $22,000.00 $22,000.00 $22,000.00 $8,000.00 $8,000.00 Base Payment $4,000.00 Cancer Lung $10,000.00 Metastasis to Bone Protein Calorie Malnutrition (PCM) Pressure Ulcer, Hip TOTAL ANNUAL REIMBURSEMENT $11,000.00 $4,000.00 $14,000.00 $26,000.00 * Dollar amounts are rounded estimates and do not reflect actual reimbursement rates $34,000.00 $45,000.00 HCCs that often are seen in the inpatient setting Note: a weight of 0.267 would = $2,507 approx reimbursement Documentation is a focus • It’s a QUALITY issue: – All diagnoses considered in the medical decision-making process need to be documented. – Explicit documentation makes the diagnosis apparent to other providers and ensures that internal and external reporting accurately reflects the quality of care provided. • It’s a REIMBURSEMENT issue: – Appropriate CMS reimbursement is received only if the diagnoses are documented and coded appropriately. Requires greater efficiencies ICD-9-CM codes selected • Under Medicare Advantage certain conditions and/or disease have been identified to be “higher risk,” higher cost and resources. • Annually CMS reviews the list of ICD-9CM codes that are considered to be conditions that are classified under MA as “risk.” • There are similarities to MCC/CCs and overlap. ICD-9-CM codes into HCCs • The selected ICD-9-CM codes are then “clustered” into categories or hierarchy condition codes (remind you of grouping of DRGs) • For example, HIV/AIDS is within HCC 2 for ICD-9-CM codes: ICD-9-CM HCC list Specific payment for HCCs • Adjustments are made for HCC payment – Only for diagnosis NOT procedures • This is an “ANNUAL” payment and covers both hospital, outpatient and physician. • Most conditions/diagnoses appear in the outpatient physician clinic setting. • HOWEVER, certain diagnoses are most likely to occur in the acute care hospital setting. – These include: Sepsis, Acute respiratory Failure, Malnutrition, Aspiration pneumonia General rules for other (additional) diagnoses • For reporting purposes, the definition for “other diagnoses” is interpreted as additional conditions that affect patient care in terms of requiring: – clinical evaluation; or therapeutic treatment; or diagnostic procedures; or extended length of hospital stay; or increased nursing care and/or monitoring. The UHDDS item #11-b • Other diagnoses as “all conditions that coexist at the time of admission, that develop subsequently, or that affect the treatment received and/or the length of stay. Diagnoses that relate to an earlier episode which have no bearing on the current hospital stay are to be excluded.” Example from a recent audit • 75-yr-old patient admitted with Sepsis (this is documented, and was coded), in addition, the patient also has a history of hypertension as well as glaucoma, which is documented and coded. • On admit to ICU, the patient was put on a Bipap, and ABGs were abnormal x2 over 24 hrs. (No documentation of possible or confirmed respiratory compromise in the chart by the provider). Patient was treated with antibiotics and progress note lists “PNA,” but the patient continues downhill after 5 days. – What was the risk of mortality? – Was this patient sicker than the data shows? – Did we get the accurate reimbursement? – Were all HCCs documented? • Action: Query or discuss with the physician • Result: Respiratory Failure = 518.81 (ICD-9-CM) = HCC 79 Example from a recent audit • 86-year-old with CHF admitted with SOB, edema, and weakness. Hx of diabetes type II. Put on O2, and Respiratory therapist noted the patient was hypoxic but no documentation by the provider of this. (Cannot code from the Respiratory Therapy note.) Per nursing assessment, patient has diabetic peripheral neuropathy, and blood sugar was 350 on sliding scale. Blood sugar drawn over 3 days, not documented by the provider (cannot code from nursing notes but they do provide clues). – – – – What was the risk of mortality? Was this patient sicker than the data shows? Did we get the accurate reimbursement? Were all conditions addressed? • Action: Query or Discuss with the physician • Result: – Hypoxemia = 799.02 (ICD-9-CM) = $5427 HCC 79 – Diabetic peripheral neuropathy = 250.70 (ICD-9-CM) = $4769 HCC 15 Risk score • Male, 80 years old: demographic score – 0.597 HCC 18 – Diabetes with Ophtho – 0.259 HCC 80 – Congestive Heart Failure – 0.410 HCC 108 – COPD – 0.399 • Total Risk score = 1.665 • Divide by normalization factor of 1.03, risk score = 1.616 Data submission is vital • Data submission occurs rather than individual UB-04 claims • Data is submitted twice a year usually • Retrospective resubmission of data is allowed • Retrospective documentation and coding audits should be routine – The time limit IS NOT the same as MS-DRGs – 2008 data resubmission can occur up to the end of 2009 and so on Risk Adjustment vs. Fee for Service (FFS) • Key differences between Risk Adjustment and Fee for Service: – Ambulatory FFS payments are driven by visit/volume and number and level of procedures (including CPT E/M) whereas ambulatory risk adjustment payment is driven by ICD-9-CM diagnoses. – For risk adjustment, each diagnosis must be captured once per calendar year in a face-to-face visit with a CMS recognized provider (physician, NP, PA, etc.). Visit volume is not relevant. – Inpatient FFS payments are driven by DRGs assigned which are grouped for each discharge. Principal diagnosis and secondary diagnosis are key. Risk adjustment, DRGs are not relevant but the diagnosis and secondary Dx count on an annual basis. – For risk adjustment, payment does not vary based on site of service. Diagnosis sources are inpatient & outpatient hospital and physician settings. FFS payment methodology varies by site or setting. National healthcare budget perspective NCAL Kaiser CDI program Get the right information, in the right place, at the right time EHR CDI mission and vision • To provide and sustain accurate, timely, and complete clinical documentation in support of – Patient safety and quality of care – Improved coding and data for internal and external users and reporting – Accurate and comprehensive reimbursement CDI goals • Understand the importance of documenting the patient’s acuity of illness by capturing the severity of illness (SOI) and risk of mortality (ROM) – the patient’s overall disease burden • Accurately capture this information in the medical record • Become familiar with ICD-9-CM codes that impact reimbursement in the CMS-HCC model • Understand IPPS MS-DRG payment methodology and the impact of MCC/CCs • Ensure that updated diagnoses (e.g., obtained through diagnostic studies) are added to the medical record • Ensure that information documented in the inpatient medical record is translated into specific, codable diagnoses Clinical Documentation Integrity Program • Initiatives – Provide HCC training for CDI Consultants – Perform concurrent chart reviews to ensure documentation reflects the severity of illness of patients – Work with the providers when documentation is incomplete or vague • Results – Documentation will more accurately reflect the severity of illness of the patient – Reimbursement will be more appropriate for the care that is rendered to each patient What will the clinical documentation program NOT do? • It does not challenge the physician's medical decision-making • It does not make the physician into a coder • It does not make the CDI consultant into a physician or into a hospital coder • It does not require more time to document completely • It does not alter – but rather enhances – documentation The CDI compliance connection • Clinical documentation improvement and the role of the Clinical Documentation Integrity Consultants (CDIC) staff are an important component of our regional compliance program. – Senior Consultant and Consultant – partnership of clinical and HIM professional • By communicating, promoting, and partnering with physicians for improved clinical documentation, the hospital may reduce the risk for submitting claims that are insufficient, incorrect, or lack medical necessity. Documentation • Document – To document a chronic, co-existing condition is to list it in the encounter note as a condition that exists and is considered in the Medical Decision-Making process in determining treatment. • Address – To address the condition is to provide a written statement of the condition and its status. It is not necessary to treat the condition to address its status. • Capture – To capture the diagnoses is to add the diagnoses to the encounter or to choose a diagnosis from the KPHealthConnect (EMR) that best describes and represents the condition. It can also be added to the patient condition problem list. Implementation approach • Phase I – Medicare Advantage Admissions – HCC Focus – 20 specific diagnostic categories • Phase II – All Medicare Admissions – Medicare Advantage – Medicare Cost and Fee-for-service – HCCs, MS-DRGs, APR-DRGs • Phase III – All Hospital Admissions – This will depend on staffing requirements PHASE I – HCC focus • Medicare Advantage Reimbursement is based on the Hierarchical Condition Categories (HCC): – We are reimbursed based on the most severe diagnoses within each category (HCC) – Disease categories are additive — that is, reimbursements are based on the sum of all chronic conditions diagnosed in different categories – Concurrent query and QA process PHASE II – Case Mix Index (DRG-based) • The average of all DRG relative weights (RW) for all discharged cases within a given time frame • For Medicare – Can be multiplied times the hospital blended rate to render – – – – an expected Medicare reimbursement revenue. (RW x blended rate = payment) Reflects the severity of the patient population served; a tertiary hospital should have an increased CMI in comparison to a rural hospital Is dependent upon the documentation within the medical record Is generally used as a benchmark measure for senior leadership This can indicate documentation or coding problems exist PHASE III – all payers (Case Mix Index impacted) • Review of all payers – inpatient setting • Target those that impact quality and outcomes • All inpatient cases are grouped to MSDRG • Review OSHPD (Office State Hospital Discharge) – California specific quality indicators PHASE I, II, and III – principal and secondary diagnosis Principal Diagnosis • That condition established after study, determined to have caused the patient’s admission to the hospital (UHDDS). Documentation that is codable Secondary Diagnosis • Secondary diagnosis is any condition that is documented by the physician and one of the following: (1) Clinically evaluated, or (2) Diagnostically tested, or (3) Therapeutically treated, or (4) Causes an increased Length of Stay (LOS) or nursing care Roles and responsibilities: Clinical Documentation Integrity Sr Consultant (CDISC) • Reviews the medical record on a concurrent basis to identify and ensure all diagnoses are documented. • Identify and communicate trends, lessons learned, and issues. • Engage Physicians to promote documentation best practices. – Partner with Physician Champion to ensure program success. • Align program goals with coding requirements: – Maintain current knowledge of coding guidelines (AHA Coding Clinic). – Maintain ongoing communication regarding Clinical Documentation Integrity Program progress with coding team. – Serve as liaison between physicians and HIM inpatient coding professionals. CDI program role clarity • Clinical Documentation Integrity Director – Regional – • Clinical Documentation Integrity Managers (2) – Regional – • Responsibilities per job description. Medical Center sponsor for CDIP. Interact and communicate with CDI staff on a regular basis. Coordinate and Participate in CDIP meetings Coding Supervisor – Medical Center HIM Department – • Conduct QA review on CDI queries, check wording for compliance, provide guidance and feedback. HIM Director – Medical Center HIM Department – • Oversee CDI QA Staff and Review on Clinical Documentation Integrity Program (CDIP) work. Gather and present Regional CDIP QA data to appropriate audience. Attend physician meetings and present data/stats. CDI QA Consultants – Regional – • Conduct oversight and supervisor CDI consultant staff within Clinical Documentation Integrity Program (CDIP). Gather and present Regional CDIP data to appropriate audience. Develop and provided education as needed to CDIC staff. Attend physician meetings and present data/stats. Clinical Documentation Integrity QA Manager (1) – Regional – • Overall responsibility for the Clinical Documentation Integrity Program in the NCal Region. Oversight of day to day operations of CDI program and staff. Lead regional CDI Steering Committee. Responsibilities per job description. Participate in CDIP Meetings. HIM Inpatient Coding Staff – Medical Center HIM Department – Abstract and Code inpatient charts as per job description. Participate in CDIP meetings as requested. Roles and responsibilities: Physician champion & treating physicians Treating Physicians • Document diagnoses to the highest level of specificity. • Maintain complete and accurate medical record documentation. • Work with CDI Consultant to respond to queries. Physician Champion • Provide leadership to the facility and regional CDI team. • Facilitates the integration of accurate, comprehensive, and concurrent documentation into daily practices for physicians and residents and other clinical personnel. • Facilitates standard uniform documentation practices in all settings. Concurrent vs. retrospective queries • Concurrent Queries – Pose questions “real time” – Generally reduce the amount of HIM Coding rebill and retrospective queries – Focus is on “Dear Doctor” queries via EMR • Pre-Bill Queries – Generally posed by coding professional following discharge (after the chart is closed, but before the claim is billed) – Risk for delay in billing; and increase in discharged not final billed accounts (DNFB) pending query response • Retrospective Queries – After the coding has been completed and the claim/acct has been billed or paid • Disadvantages of Retrospective Queries – Physician recall compromised due to timing – Generally time consuming to place query and await follow-up Concurrent query example • Scenario – The CDI Consultant examines a chart day 3 of the patient’s hospital stay. The patient presented with a fever of 101, productive cough, pleuritic pain, and was diagnosed with pneumonia. He has a history of COPD on home 02. The patient was being treated with Zithromax for a vague URI outpatient prior to admission. The patient is now placed on two IV antibiotics; both having gram negative coverage properties. • Risk Factor – COPD with home 02 (tubing is a breeding ground for bacteria) • Sign/Symptoms-fever, productive cough, pleuritic pain, failed outpatient treatment • Treatment-Acute hospitalization, multiple IV antibiotics • Query – The CDI Consultant queries the physician, asks to clarify and document whether she is empirically treating a suspected specific type of pneumonia (listing choices provided) Concurrent query example • Scenario – The CDI Consultants examines a chart day 3 of the patient’s hospital stay. She notes that the patient was admitted via the ED for an ORIF of his tibia/fibula fracture. The progress note indicates the patient has rales on the second day post-op and a slight fever with oral antibiotics started. • Query – The CDI Consultant concurrently queried the physician asking for the clinical diagnosis related to the postoperative rales, fever, and antibiotics ordered. When to query • The following situations are examples of when it is appropriate to query the physician for documentation clarification: – Clinical indicators of a diagnosis, but no documentation of the – – – – – diagnosis Clinical evidence for a higher degree of specificity or severity A cause-and-effect relationship between two conditions or organisms An “underlying cause” when admitted with symptoms The treatment is documented, but not the associated diagnosis Present on Admission (POA) indicator status for a documented diagnosis AHIMA. Practice Brief, “Managing an Effective Query Process" Journal of AHIMA 79, no.10 (October 2008): 83-88 When to query (cont.) • It is appropriate to query the healthcare provider for clarification and additional documentation regarding: – Conflicting, incomplete, or ambiguous information in the health record. – Abnormal findings (laboratory, x-ray, pathologic, and other diagnostic results), which cannot be coded and reported unless the healthcare provider indicates their clinical significance. – Secondary conditions or diagnoses noted by nurses and/or other ancillary personnel, which cannot be coded and reported unless the healthcare provider documents that they are clinically significant as a current diagnosis. When NOT to query • Queries should not be used to question a provider’s clinical judgment, but rather to clarify documentation when it fails to meet criteria for completeness, clarity, consistency, or precision. • Queries may not be appropriate simply because the clinical information or clinical picture does not appear to support the provider’s documentation of a condition or procedure. – Example: documentation of acute respiratory failure in a patient whose laboratory findings do not appear to support this diagnosis. VIA EMR … ‘Dear Doctor’ note process HCC and diagnosis focus areas – common for inpatient setting HCC Condition Body System/Disease Group 1 2 Sepsis (w/ pneumonia), SIRS, shock, UTI Infectious Disease 2 7 Metastatic Cancer (all) Neoplasm 3 10 Cancer: Prostate, Breast, Colorectal, and other cancers and tumors Neoplasm 4 15 Diabetes w/ CKD or PVD Endocrine/Nutrition & Metabolic 5 16 Diabetes w/ Neuropathy and other manifestations Endocrine/Nutrition & Metabolic 6 21 Protein Calorie Malnutrition (type/degree) Nutrition & Metabolic 7 79 Respiratory Failure (all) Respiratory System 8 105 PVD (with and without Complication) Vascular System 9 131 Renal Failure/disease (include dialysis status) Renal/Urinary system HCC and diagnosis focus areas (cont.) HCC** 10 111, 112 11 80, 81, 82, 83, 92 12 148, 149 Condition Body System/Disease Group Pneumonia * Respiratory System Cardiac (heart failure*/shock, cardiac Cardiac/Circulatory System arrhythmia, acute MI,* old MI, angina) Pressure ulcers (Cellulitis and all other Disease of the Skin chronic ulcers) 13 75, 95, 96 Stroke*/CVA/Hemorrhage (coma) Nervous System 14 100 Stroke*/CVA residual deficit Nervous System 15 154, 155 Head Injuries (Trauma) Trauma/Injury 16 157 Vertebral Fractures (Trauma) Trauma/Injury 17 158 Hip Fractures (Trauma) Musculoskeletal System 18 161 Traumatic Amputation (include status) Injury 19 176 Artificial Opening feeding/Ostomies 2nd Dx (status) 20 177 * Core Measures Amputation Status and Complications 2nd Dx Using the problem list – capturing systemic diagnosis – correlates with AHA Coding Clinic • Per KP policy (from National Compliance) a systemic condition is defined as one which: – It is always present, even though it may have been stabilized; AND – By its very nature (because of its impact on the patient), requires that it be considered by the physician in evaluating the patient’s chief complaint; AND – The condition affects a major body system (and typically, more than one major body system) which include the following: • • • • • • Cardiovascular; and/or Respiratory; and/or Renal; and/or Hematolgocia/Lymphatic/Immunologic; and/or Neurologic; and/or Psychiatric CDI tools 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. Clinical Documentation Integrity Review Sheet Clinical Documentation Integrity Tracking Log Hospital Census Report Shared Patient List Report Medical Diagnosis Prompt Report Hospital Discharge Report CDI QA Review Sheet CDI QA Tracking Log CMS MA HCC & ICD-9-CM List 3M Encoder Software DRG Expert (Ingenix) AHIMA Practice Brief “Managing the Physician Query Process” Tracking log CDI QA audit and processes • The quality assurance audits will monitor, measure and/or evaluate the following: – The accuracy of HCC assignment and presence or absence of – – – – – – – documentation The appropriateness and rationale for issuing a query The adequacy of documentation to support the MS-DRG assignment The identification of secondary diagnoses that support Severity of Illness (SOI) The validation of the HCC after the chart has been coded The identification of potential compliance issues such as leading queries The timeliness, response rate, and agreement rate of the physician staff The identification of additional CDISC staff individual or group training needs CDI QA • The quality assurance standards for CDISC staff are as follows: – Week 1 onsite at Medical Center: 100% of charts reviewed by the CDISC staff will be audited by the Clinical Documentation Integrity Consultant (CDIC) QA staff. Results will be documented and summarized in the CDI QA tool. CDISC staff must perform at 95% or higher as reported in the CDI QA summary report. • If the 95% target is achieved as a result of the Week 1 audit, 50% of the charts reviewed by • • the CDISC staff will be audited by the CDIC QA staff during Week 2. If the 95% target is maintained as demonstrated by the Week 2 audit results, for Week 3 and Week 4, 25% of the charts reviewed by the CDISC staff will be audited by the CDIC QA staff. If the 95% target is maintained for Weeks 1 through 4, audits will be on a regular schedule: 5% of charts reviewed or 25 charts per CDISC. – If the 95% target is not reached as shown by the Week 1 audit results, 100% of the charts reviewed by the CDISC staff will be audited by the CDIC QA staff during Weeks 2, 3, and 4 or until the 95% target is achieved. – During the initial four weeks, targeted education will be provided to CDISC staff to help address any deficiencies found during the quality assurance audits. Expected CDI outcomes Improved & Increased Compliance Accurate Capture of Severity/Acuity Improved Quality Scores and Report Cards Improved Patient Outcomes/Care Strong Documentation Program More Accurate HCC and DRG Assignment More Appropriate Reimbursement Accurate Capture of Risk of Mortality Greater Documentation Specificity in Chart CDI stats (week ending 2/19/2010) Week Total Number of Charts Audited Number of HCCs Validated Valid HCCs Found Dec-2009 Jan-10 Week 10 (1/30 - 2/5) Week 11 (2/6 - 2/12) Week 12 (2/13 - 2/19) Month-To-Date Totals Year-To-Date Totals 0 119 44 70 23 137 256 0 54 23 9 11 43 97 0 35 10 7 6 23 58 % of Charts Audited vs. Admissions 38.55% % HCC % Valid Validated vs. HCCs Found Total Number vs HCCs of Charts Validated Audited 37.89% 59.79% CDI stats Inpatient HCCs (week ending 2/19/2010) 2/19/2010 Description HCC 2 Septicemia/Shock HCC 7 Metastatic Cancer and Acute Leukemia HCC 10 Breast, Prostate, Colorectal and Other Cancers and Tumors HCC 15 Diabetes with Renal or Peripheral Circulatory Manifestation HCC 16 Diabetes with Neurologic or Other Specified Manifestation HCC 21 Protein-Calorie Malnutrition HCC 79 Cardio-Respiratory Failure and Shock HCC 105 Vascular Disease HCC 131 Renal Failure Queried Actual Validated Estimated Qty Qty Qty Reimbursement Found $ Value Agreed Valid $ Value $ Value $7,235 9 $65,115 3 $21,705 3 $21,705 $21,695 0 $0 0 $0 0 $0 $1,983 0 $0 $4,842 29 $3,889 $8,159 $5,509 $3,012 $3,508 3 36 14 0 7 0 $0 0 $0 $140,418 21 $101,682 12 $58,104 $11,667 $293,724 $77,126 $0 $24,556 2 $7,778 29 $236,611 11 $60,599 0 $0 5 $17,540 2 22 11 0 4 $7,778 $179,498 $60,599 $0 $14,032 Top 10 HCCs (week ending 2/19/2010) Frequency of HCCs 4 4 31 6 36 7 9 14 29 HCC 21 Protein-Calorie Malnutrition HCC 15 Diabetes with Renal or Peripheral Circulatory Manifestation HCC 79 Cardio-Respiratory Failure and Shock HCC 2 Septicemia/Shock HCC 131 Renal Failure HCC 148 Decubitus Ulcer of Skin HCC 111 Aspiration and Specified Bacterial Pneumonias HCC 80 Congestive Heart Failure HCC 16 Diabetes with Neurologic or Other Specified Manifestation HCC 157 Vertebral Fractures without Spinal Cord Injury 1422 charts reviewed; 115 queries submitted Documentation tip • Documenting “DM,” “NIDDM,” or “Diabetes controlled with meds” can create poor data, indicate a lower level of severity, and inaccurate payment • Clearly define the type of diabetes the patient has • Use the phraseology from the most appropriate ICD-9 codes, i.e., “type 1″ or “type 2″ diabetes and especially if the diabetes mellitus is controlled or not controlled • Document the manifestation of the diabetes also i.e., neuropathy Ask about Medicare Advantage • What % of your patients’ population are MA? • Conduct documentation and coding audits on MA • Data mining inpatient MA discharges • Increase awareness and education AHIMA CDI Practice Brief • Clinical Documentation Improvement Program... A Model Guidance • The following guidance does not replace the 2008 AHIMA Practice Brief, Managing an Effective Query Process, It is, however, intended to provide greater specificity and detail related to Clinical Documentation Improvement programs. • Healthcare consumers are unique. Each person has their own combination of medical conditions that must somehow be standardized for comparison. One way to capture this data is the translation of clinical documentation into codes (e.g., ICD-9-CM or CPT) which has traditionally been the domain of the Health Information Management (HIM) professional. The domain of the clinical professional has been the analysis of specific data quality elements and how that data impacts patient care and outcomes. Clinical Documentation Improvement Program.... A Model Guidance • Policies and Procedures • CDI Role, Competencies and Staffing Models • Role of the CDI Physician Advisor • Query (Clarification) • Leading/non-leading queries • Conclusion • CDI programs provide new opportunities for professionals in a changing healthcare environment. CDI professionals have the opportunity to lead their organizations in the documentation improvement process and be a champion for quality, timely documentation. Clinical Documentation Improvement Program.... A Model Guidance • This practice brief will provide an overview of key elements in establishing, maintaining and/or enhancing a CDI program. This can be achieved through a variety of methods and structure that are tailored to the unique needs of the healthcare entity. • This brief includes the following sections: – policies and procedures; • the role, competencies, and staffing models for the CDI professional; • physician leadership; and • query examples specific to CDI. Summary • Medicare Advantage is driven by documentation and coding • Understanding MA can help with hospital • CDI should be inclusive of all Medicare payers • Track the payer types within your CDI program Resources/References • Medical Care, Vol 43, Number 1, January 2005, pg. 34. • Medicare HCC Coding is Mission Critical for HMOs, Sep 1, 2007, Al Lewis • Risk Adjustment of Medicare Capitation Payments Using the CMS-HCC Model, Healthcare Financing Review, September 2004 • www.cms.hhs.gov/MMCAG/04_PartCRecon.asp • HCC Blog, Risk Adjustment and Medicare Advantage by – J. Matt Yuill, MD, CPC • Kaiser Family Foundation Thank you Questions?