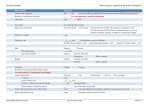
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Skin Block • Introduction To Diseases Of The Skin • Acneiform, Alopecias, and Pigmentary Disorders • Eczemas, Papulosquamous, and Vesiculobullous Skin Disease • Skin Neoplasms • Drug Eruptions • Skin Signs of Systemic Disease Learning Objectives At the end of the session the students will be able to: • Describe the layers of the skin, including the layers of the epidermis • Utilize the dermatology vernacular to allow the appropriate description of lesions • Model a comprehensive dermatologic exam, including lesion description and distribution Introduction to Skin Kerri E. Rieger, MD, PhD Stanford Dermatology and Pathology Why study the skin… Clinical Definitions in Dermatology: Morphology MACULE ‐ small, flat, non‐palpable lesion ‐ <10 mm in diameter PATCH ‐ small, flat, non‐palpable lesion ‐ <10 mm in diameter PAPULE ‐ small, superficial, circumscribed, palpable lesion elevated above the skin surface ‐ <10 mm in diameter PLAQUE ‐ palpable lesion, elevated above the skin surface ‐ >10 mm NODULE ‐ firm (indurated) lesion that is thicker or deeper than the average papule or plaque (a nodule that is subcutaneous might not elevate the skin surface) VESICLE ‐ elevated lesion that contains clear fluid ‐ a small blister ‐ < 10 mm in diameter BULLAE ‐ elevated lesion that contains clear fluid ‐ >10 mm in diameter PUSTULE • superficial elevated lesion that contains yellow fluid (pus) Macule flat lesion <1cm Papule elevated lesion <1cm Nodule palpable lesion, usually >1cm and deeper in the dermis or subcutis Patch Flat lesion >1cm Plaque elevated lesion >1cm Vesicle fluid filled lesion <1cm Pustule purulent exudate filled lesion Bulla fluid filled lesion >1cm Macule flat lesion <1cm Papule elevated lesion <1cm Nodule palpable lesion, usually >1cm and deeper in the dermis or subcutis Patch Flat lesion >1cm Plaque elevated lesion >1cm Vesicle fluid filled lesion <1cm Pustule purulent exudate filled lesion Bulla fluid filled lesion >1cm Approach to morphological description Size Measure in cm Color Black, white, blue, purple, brown, tan, red, pink, yellow, .. violaceous, erythematous, hypopigmented, hyperpigmented, dusky Basic/primary morphology Macule, patch, papule, plaque, nodule, tumor, vesicle, bullae, pustule Secondary morphology Scale, crust, erosion, ulceration, excoriation, eschar, lichenification, atrophy Demarcation Well‐demarcated, poorly‐demarcated Arrangement/conf Linear, grouped, scattered, reticular, arcuate, iguration annular Distribution Generalized, unilateral, bilateral, chest, back, face, upper or extremities, sun‐exposed Approach to morphological description Size Measure in cm Color Black, white, blue, purple, brown, tan, red, pink, yellow, .. violaceous, erythematous, hypopigmented, hyperpigmented, dusky Basic/primary morphology Macule, patch, papule, plaque, nodule, tumor, vesicle, bullae, pustule Secondary morphology Scale, crust, erosion, ulceration, excoriation, eschar, lichenification, atrophy Demarcation Well‐demarcated, poorly‐demarcated Arrangement/conf Linear, grouped, scattered, reticular, arcuate, iguration annular Distribution Generalized, unilateral, bilateral, chest, back, face, upper or extremities, sun‐exposed “The skin examination is notable for (____)cm (_________) , (____________) size color primary lesion with (________) in a (__________) configuration, located over the (__________).” secondary changes configuration distribution “The skin examination is notable for (____)cm (_________) , (____________) size color primary lesion with (________) in a (__________) configuration, located over the (__________).” secondary changes configuration distribution “The skin examination is notable for (____)cm (_________) , (____________) size color primary lesion with (________) in a (__________) configuration, located over the (__________).” secondary changes configuration distribution “The skin examination is notable for (____)cm (_________) , (____________) size color primary lesion with (________) in a (__________) configuration, located over the (__________).” secondary changes configuration distribution “The skin examination is notable for (____)cm (_________) , (____________) size color primary lesion with (________) in a (__________) configuration, located over the (__________).” secondary changes configuration distribution ABCDEs Approach to full body skin examination • Have an adequately lit room • Have the patient fully gowned will improve your exam • Have a systematic order that you follow consistently, so that you don’t forget to check easy‐to‐miss locations (e.g. the conchal bowl, in the mouth, alar creases, interdigital spaces, intergluteal cleft, soles, etc) • Consider an integrated skin examination (internist can perform full skin check on chest/back while listening to heart/lungs; face while feeling for lymphadenopathy; legs while checking reflexes and edema Skin structure and function Histology of Skin Histology of Skin e = epidermis d = dermis h = hair follicle g = eccrine sweat gland s = sebaceous gland lc = Langerhans cell m = Merkel cell b = basal cell f = fibroblast mc = mast cell dc = dendritic cell v = blood vessel sc = stratum corneum Normal Epidermal Histology Stratum Corneum Stratum Granulosum Stratum Spinosum Stratum Basale Dermis Components of the Epidermis • Epidermis – Keratinocytes – Melanocytes – Langerhans Cells – Merkel Cells Keratinocyte • Form functional barrier against environment • Contain keratins (intermediate filaments) Hemiesmosomes Desmosomes Melanocyte • Melanin producing cells found in skin, inner ear, choroid and iris of the eye • Ratio of melanocytes to basal cells = 1:4‐ 1:10 • Form melanosomes (distinct organelle) and transfer to keratinocytes Melanosome on EM Langerhans Cells • Distinct population of antigen presenting cells; function as intra‐epidermal macrophages • Will migrate to regional lymph nodes when stimulated Birbeck Granules Merkel Cells • Located in basal layer • Found mainly on tactile areas of hair‐bearing skin, taste buds, anal canal, labial epithelium, and around eccrine glands • Involved in touch sensation – one free nerve ending from dermis touches up to 50 Merkel cells to form a “Merkel cell‐neurite” complex CK20 DEFINITIONS IN DERMATOPATHOLOGY Hyperplasia Increase in the number of cells of the epidermis Hyperkeratosis Thickening of the stratum corneum Parakeratosis Flattened and retained keratinocyte nuclei within the stratum corneum Follicular plugging Hyperkeratosis within hair follicle Hyper/Hypogranulosis Increased/decreased thickness in the granular layer Acanthosis Thickened squamous/spinous cell layer Papillomatosis Elevation of adjacent dermal papillae above the surrounding epidermal surface Spongiosis Intercellular edema Exocytosis Inflammatory cells within epidermis, usually with spongiosis (usually refers to lymphocytes, and implies a benign process) Epidermotropism Abnormal cells within the epidermis without significant spongiosis (seen in Mycosis Fungoides, Melanoma mets) Acantholysis Separation & rounding up of keratinocytes because of loss of intercellular adhesions Dyskeratosis Abnormally or prematurely keratinised eosinophilic keratinocytes, identified by prominent eosinophilic (red‐staining) cytoplasm Vacuolar degeneration Damage to the basal layer, with intracellular oedema and vacuoles. May be associated with colloid body formation and clear spaces at the dermal‐ epidermal junction, sometimes resulting in a subepidermal blister. Basket Weave Orthokeratosis Compact Orthokeratosis Hyperkeratosis Parakeratosis Acanthosis Papillomatosis Hyper‐ and Hypogranulosis Necrotic Keratinocytes = Civatte Bodies (or Colloid Bodies in the dermis) Acantholysis Tissue Reaction Patterns in Dermpath The Spongiotic Reaction Pattern • • • • Widening of intercellular spaces Elongation of intercellular bridges (desmosomes) Inflammatory cells in the epidermis: lymphs, eos, neuts Seen commonly in “eczema” Wide Intercellular Spaces/Eosinophils Lymphocyte Collections in Epidermis Neutrophils Within the Spongiosis Intense Spongiosis with Vesiculation NOTE: Smooth Borders Subacute Spongiotic Dermatitis Chronic Spongiotic Dermatitis Irregular Length of Rete Ridges, Jagged Edges The Psoriasiform Reaction Pattern Regular Elongation of Rete Ridges The Lichenoid Reaction Pattern Band‐like infiltrate that hugs the dermoepidermal junction The Vesiculobullous Reaction Pattern Biopsy techniques Thank you!