Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
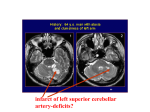
Clinical-Pathologic Conference From the Case Records of the New England Deaconess Hospital Date of Admission: November 17, 1985 Chief Complaint: Persistent cough and rash History of the Present Illness: A 64-year-old man was in his usual state of health until mid-December 1984, when he began experiencing productive cough and pleuritic chest pain without fevers, chills, sweats, or dyspnea. Shortly after the onset of his symptoms, he noted a painless, non-pruritic, purple lesion on the extensor surface of his right forearm. Although he did not seek medical care at that time, the description he provides suggests that the lesion coalesced into a pustule, spontaneously erupted and drained, crusted over, again formed a pustule, again spontaneously erupted and drained, and so on. In February 1985, he began experiencing progressive pain and swelling of his right thumb. In May, he developed a lesion over the proximal, ventral surface of his right thumb; this lesion followed a similar course to the right forearm lesion described above. In June 1985, he was seen by his primary care physician and was given an antibiotic, the name of which he does not recall. He also complained of new dysuria, urinary frequency, hesitancy, and urgency, all of which were attributed to age-associated benign prostatic hyperplasia. In October 1985, he presented to an outside hospital with acute urinary retention. He was hospitalized and ultimately underwent a transurethral resection of the prostate gland. Although the full operative note is not available, the resected prostate gland reportedly appeared inflamed. Post-operatively, he had improvement of his urinary symptoms, and his recovery was uneventful from a urological perspective. While hospitalized, he developed acute inflammation (pain, tenderness, erythema, and warmth) of his right ankle; this episode was treated with indomethacin and tetracycline. In November 1985, given his persistent pulmonary symptoms and ongoing rash, the patient sought a second opinion at “that great medical center out east.” His past medical history is notable for hypertension. He also has a history of exposure to tuberculosis; two aunts and two uncles reportedly died from complications of pulmonary tuberculosis. The patient had a negative PPD in September 1985. His past surgical history is notable for an open reduction of an open comminuted fracture of his distal right tibia and fibula following a propane explosion in 1968. A metal plate was inserted at that time; it was subsequently removed. His current medications include only Aldactazide (a combination of spironolactone and hydrochlorothiazide). He has no known drug allergies. Social History: He is a retired farmer. He was born and raised in Iowa, and has lived exclusively in Iowa and Minnesota throughout his life. He has never traveled elsewhere; he came to the NEDH only for the “second opinion” mentioned above. He does not smoke cigarettes, drink alcohol, or use illicit drugs. His family history is unremarkable. Physical Examination: On admission to the NEDH, his temperature was 98.3°F, pulse was 73 and regular, blood pressure was 121/74, respirations were 14 per minute, and oxygen saturation was 97% on room air. He was a pleasant, well-appearing man who looked his stated age. His sclerae were anicteric. His oropharynx was clear and without lesions. His neck was soft and supple. There was no cervical, axillary, or inguinal adenopathy. Cardiac auscultation demonstrated a regular rate and rhythm, normal S1 and S2 heart sounds, and no murmurs, rubs, or gallops. The lungs were clear to auscultation and percussion bilaterally. The abdomen was soft, non-tender, and non-distended; there were normal active bowel sounds, and there was no organomegaly. There was no spinal or costovertebral angle tenderness. The prostate was palpable and was moderately enlarged; it was firm and was not tender. There was no lower extremity edema. Pedal pulses were palpable bilaterally. Examination of the skin demonstrated a 4 x 4 cm, ulcerated lesion of the right forearm; this lesion is demonstrated in slide #1 of the attached power point presentation. There was a smaller lesion at the base of the right thumb; this lesion is demonstrated in slide #2. There was chronic-appearing scarring and hyperpigmentation over the anterior right lower tibia, and there was an area of erythematous swelling over the right lateral malleolus that was slightly tender. The remainder of the skin examination was normal. Initial Labs: On admission, there were 11,900 white blood cells per microliter with a normal WBC differential. The hematocrit was 36%; the MCV and RBC indicies were normal. There were 224,000 platelets per microliter. The serum chemistries were normal. The BUN was 19 mg/dL and the serum creatinine was 1.3 mg/dL. Liver enzymes, including ALT, AST, alkaline phosphatase, and total bilirubin, were normal. A urinalysis with sediment showed 3 WBC and 1 RBC per high-powered field; there were no bacteria. Imaging Studies: PA and lateral chest radiographs showed a prominent left ventricle with a tortuous aorta and linear fibrosis at the base of the left lung. A plain radiograph of the right ankle is shown in slide #3. Plain radiographs of the right forearm and thumb demonstrated a lytic defect in the cortex of the proximal phalanx of the right thumb. A bone scan showed intensely increased uptake in the distal fibula and moderately increased uptake in the proximal phalanx of the right thumb. A diagnostic procedure was performed. Questions: 1) What was the diagnostic procedure? 2) What is the diagnosis?