Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
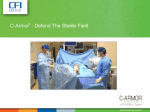
Objectives 1. Be more familiar with the potential breeches in asepsis in an A Review of Asepsis and Safe Medication Practices ASC. 2. Be able to discuss the 7 Principles of Surgical Asepsis 3. Describe safe medication practices in the ASC practice setting. Mary L. Gish, DNP, RN, NEA-BC Nurse Consultant III Center for Health Care Quality Licensing and Certification Asepsis ! Asepsis is the state of being free from disease-causing contaminants (such as bacteria, viruses, fungi, and parasites) or, preventing contact with microorganisms. The term asepsis often refers to those practices used to promote or induce asepsis in an operative field in surgery or medicine to prevent infection. Essential Components of Medical Asepsis ! ! ! ! Handwashing Utilizing gloves, gowns and masks as indicated Cleaning equipment Handling linens properly Medical vs Surgical Asepsis ! ! Medical asepsis or clean asepsis is the state of being free from disease causing microorganisms. Medical asepsis is concerned with eliminating the spread of microorganisms through facility practices. Surgical or Sterile Asepsis includes procedures to eliminate micro-organisms from an area and is practiced by the members of the surgical team in operating rooms and treatment areas. Hand Hygiene • • • • • • • • • Sanitizer or Hand Wash Before and after gloving (sterile or clean) Medication Administration Feeding residents (before and after) Any invasive procedure (catheterization, blood glucose) Contact with resident Are sinks and hand sanitizers readily available? Are gloves readily accessible? Hand wash only for dietary, GI symptoms 1 Aseptic Technique ! ! ! Chain of Infection Infectious Disease Cycle Aseptic technique refers to a procedure that is performed under sterile conditions. This includes medical and laboratory techniques, such as with cultures. Pathogen The largest example of aseptic techniques is in hospital operating suites. Host Reservoir Portal of Exit New Host (Disease) Aseptic technique is the effort taken to keep patients as free from micro-organisms as possible Portal of Entry Infection Process Mode of Transmission Agents • Bacteria ! Aerobic ! Anaerobic • Viruses ! HBV ! Influenza • Fungi ! Responsible for some of the most common infections • Protozoa Entrance of Microorganisms ! ! Skin is the first line of defense Depends on nature of the pathogen • Influenza (Respiratory Droplet) • MRSA (Contact) • HIV/HBV (Blood and Body Fluids) Mode of Transmission 1. Fomite • Inanimate objects • Stethoscope, thermometer, scissors 2. Vector • Living carrier • Human hands Infection Process ! Host • A micro-organism must accept the host • Infection develops as the strength and numbers grow in host • Immunizations have proved effective in providing additional protection against infectious disease 2 Medical Asepsis = Standard Precautions 1. 2. 3. 4. 5. 6. 7. Combines Universal Precautions and BSI Applies to all patient encounters Emphasizes hand hygiene Use of gloves, gown masks and eye protection depending on the anticipated exposure Safe injection practices Equipment or items in the resident environment likely to have been contaminated with infectious body fluids must be handled in a manner to prevent transmission Education and training are the foundation Transmission Based Precautions ! 3 Categories • Contact Precautions - excessive wound drainage, fecal incontinence, or other • Droplet Precautions – influenza, group A Strep • Airborne Precautions - TB Surgical Asepsis ! Requires the absence of all microorganisms, pathogens and spores from an object Standard Precautions Combines Universal Precautions and BSI Applies to all residents Emphasizes hand hygiene Use of gloves, gown masks and eye protection depending on the anticipated exposure Safe injection practices Equipment or items in the resident environment likely to have been contaminated with infectious body fluids must be handled in a manner to prevent transmission Education and training are the foundation 1. 2. 3. 4. 5. 6. 7. Hand Hygiene • • • • • • • • • Sanitizer or Hand Wash Before and after gloving (sterile or clean) Medication Administration Feeding residents (before and after) Any invasive procedure (catheterization, blood glucose) Contact with resident Are sinks and hand sanitizers readily available? Are gloves readily accessible? Hand wash only for dietary, GI symptoms Surgical Asepsis Principles of Sterile technique • A sterile object remains sterile until touched by another sterile object • Only sterile objects may be placed on a sterile field • A sterile object or field out of vision is contaminated • A sterile object or filed becomes contaminated by prolonged exposure to air 3 Surgical Asepsis Principles of Sterile technique • When a sterile surface comes in contact with a wet, contaminated surface, the sterile object of field becomes contaminated • Fluids flow in the direction of gravity • The edge of the sterile field or container is consider contaminated Surgical Asepsis ! Opening Sterile packages • Labels indicate the date that sterilization expires • Compromised packaging are no longer considered sterile • Providers follow strict handwashing protocol Surgical Asepsis Principles Surgical Asepsis Principles Principle # 1: Scrubbed persons function within a sterile field Principle #2 Sterile drapes are used to crate a sterile field ! ! ! ! ! ! Surgical team consists of sterile and non-sterile members Sterile=Scrubbed Non sterile remain in periphery All wear scrub attire Scrubbed persons wear sterile gown, mask, gloves, shields Sterile areas • Gown front from chest to sterile field level • Sleeves 2” above elbow to cuff ! ! ! ! ! ! ! Establish an aseptic barrier minimizing the passage of microorganisms Places on patient, furniture, and equipment to be included in the sterile field Only incisional area is exposed Only scrubbed personnel handle drapes Held higher than the OR table, from incision out Not moved or rearranged Top surface is only area sterile Surgical Asepsis Principles Surgical Asepsis Principles Principle #3: All items used on a field must be sterile Principle #4: All items introduced to the sterile field should be opened, dispensed, and transferred by methods that maintain sterility and integrity ! ! ! ! Sterile and non sterile never mix Sterility is determined by events not by time Items are inspected for package integrity and indicators Otherwise considered contaminated ! ! ! Non-sterile personnel (i.e. Circ Nurse) uses good judgment when dispensing items Tossing may compromise field by tearing, displacing The 5 minute rule does not apply 4 Surgical Asepsis Principles Principle #4 Principle #4 continued ! ! ! ! ! Open the top wrapper away first, then open the flaps to each side The last wrapper flap is pulled toward the nonsterile person opened the package Once opened contents are sterile up to 1 inch outer edge Margin of safety Double wrapped relies on institution policy Surgical Asepsis Principles Surgical Asepsis Principles Principle #5: A sterile field should be maintained and monitored constantly Principle #6: Personnel should move around the field in a manner that maintains sterility ! ! ! ! ! ! Must be monitored by all members of OR team Sterility cannot be guaranteed but team must be vigilant Breeches require immediate action to correct Prepared as close to the OR time as possible Time and exposure are risk factors Risks: personnel, airborne contaminants, insects and liquids ! ! ! ! ! Establish safe distance or margin of safety between sterile and nonsterile areas Non-sterile personnel remain in non sterile areas Always face the field Never walk between two sterile fields Never reach over or risk contact of touching sterile field Surgical Asepsis Principles Surgical Asepsis Principles Principle #6: Personnel should move around the field in a manner that maintains sterility Principle #7: Policies and Procedures for maintenance of sterile field should written, reviewed annually and available in practice setting ! ! ! ! ! Patient is the center with scrubbed personnel close without movement away Move from sterile to sterile only Scrub personnel keep distance and pass face to fact or back to back Scrubbed keep same position throughout procedure Arms and hands always in the field ! ! ! Included in initial orientation and ongoing education of staff Training of aseptic technique and practices by skilled members to new and inexperienced. Mentors and preceptors 5 New Work Being Done Safe Injection Practices Pharmacy Guidelines Never re-use needles Never share lancet holders Never share insulin pens Never use finger stick devices for more than one person Never use a blood glucose meter for more than one person without cleaning and disinfecting it in between uses • Never use insulin pens for more than one person • Never fail to change gloves and perform hand hygiene between finger stick procedures • • • • • ASHP(2013). Drug Distribution and Control: Preparation and Handling–Guidelines. ASHP Guidelines on Compounding Sterile Preparations, retrieved 10/24/2014 from http://www.ashp.org/ doclibrary/bestpractices/prepgdlcsp.aspx Pharmacy Guidelines Medication Safety What is a multi-dose vial? ! ! Multiple dose vials my be used for more than on patients as long as they are not accessed in a patient care area. ASHP (2013). Drug Distribution and Control: Preparation and Handling–Guidelines. ASHP Guidelines on Compounding Sterile Preparations, retrieved 10/24/2014 from http://www.ashp.org/doclibrary/bestpractices/prepgdlcsp.aspx ! A multi-dose vial is a vial of liquid parenteral medication (injection or infusion) that contains more than one dose of medication. Multi-dose vials are labeled as such by the manufacturer and typically contain an antimicrobial preservative to help prevent the growth of bacteria. The preservative has no effect on viruses 6 Medication Safety Can multi-dose vials be used for more than one patient? How? ! ! ! Dedicated to a single ! Examples of the immediate patient treatment area include patient rooms or bays, hallways and operating rooms. If a multi-dose vial enters the immediate patient treatment area, it should be dedicated to that patient only and discarded after use. ! When should multi-dose vials be discarded? ! Whenever sterility is compromised or questionable. ! What are examples of the “immediate patient treatment area”? More than one patient not kept or accessed in the immediate patient treatment area. Medication Safety ! Medication Safety Medication Safety Video If a multi-dose has been opened or accessed (28 days or manufacturer’s date, soonest) Unopened = manufacturer’s expiration date. Tools Available for Use ! ! CMS Exhibit 351 Infection Prevention Checklist for Outpatient Settings: Minimum Expectation for Safe Care 7 8 9 10 References ! ! ! ! ! ! ! ASHP(2013). Drug Distribution and Control: Preparation and Handling–Guidelines. ASHP Guidelines on Compounding Sterile Preparations, retrieved 10/24/2014 from http://www.ashp.org/doclibrary/bestpractices/prepgdlcsp.aspx http://oneandonlycampaign.org/content/audio-video http://antt.org/ANTT_Site/resources.html http://www.cdc.gov/injectionsafety/providers/provider_faqs_multivials.html Leopold, J. (2014)Aseptic Technique: Principles and Practices. AORN Journal, Volume 94 , Issue 2 , 213 – 214 http://www.ismp.org/selfassessments/default.asp http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/ som107_exhibit_351.pdf AORN Journal 2011 94, 213-214DOI: (10.1016/j.aorn.2011.04.018) Copyright © 2011 AORN, Inc Nurse Consultant Infection Prevention and Control Mary Gish, DNP, RN, NEA-BC Nurse Consultant III, Infection Control 916-552-8636 [email protected] Thank You! 11