Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
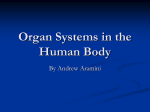
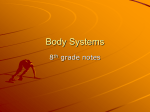
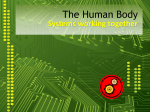
Journal of Gerontology: BIOLOGICAL SCIENCES 2000, Vol. 55A, No. 12, B593–B600 Copyright 2000 by The Gerontological Society of America Age Increases the Skeletal Versus Muscular Component of Lower Extremity Stiffness During Stepping Down Paul DeVita and Tibor Hortobagyi Biomechanics Laboratory, East Carolina University, Greenville, North Carolina. Elderly adults step down with greater lower extremity stiffness than young adults. The purpose of this study was to compare skeletal and muscular components of lower extremity stiffness between elderly and young adults during stepping down. Fourteen elderly (age, 70.1 years) and 16 young (age, 20.8 years) adults stepped down onto a force plate from 10% and 20% body heights while being videotaped. Lower extremity stiffness was defined as the ratio between the floor reaction force directed along the limb and limb compression. It was partitioned into skeletal and muscular components using the angular relationship () between the direction of the force and the line of the leg. Our results showed that was 21% smaller ( p ⬍ .03), the skeletal component was 48% larger ( p ⬍ .025), and the ratio of skeletal to muscular components was 32% larger ( p ⬍ .01) in elderly adults compared with young adults. Elderly adults rely more on their skeletal and less on their muscular systems when stepping down compared with young adults, producing a stiffer lower extremity. F LOOR contacts during daily locomotor movements apply forces onto the human musculoskeletal system that tend to cause the person to collapse. Contact with a step during stair descent, for example, applies loads of approximately twice the bodyweight onto the foot; these loads are transmitted upward through the skeletal system and tend to cause dorsiflexion at the ankle and flexion at the knee and hip joints (1). Initiating appropriate neuromuscular responses to these forces after the instant of floor contact will be unsuccessful because they are often applied too rapidly [i.e., in 100–150 ms (1–5)], particularly for elderly adults. Elderly men and women have longer reaction times (6) and neural modulation times (7), poorer joint proprioception (8), and slower rates of torque development compared with young adults (9–11). Thelen and colleagues (9), for example, showed that elderly women required 472 ms to reach a functional level of 60 Nm of plantarflexor torque at the ankle while young women required only 311 ms to generate the same torque. Since many adults—particularly elderly adults—are not able to respond quickly enough after the application of ground reaction forces during locomotion, the initial properties of their lower extremities at the onset of the load are critical for successful movement. Lower extremity stiffness, the intrinsic resistance of the limb to compressive external loads, will therefore influence how well a person locomotes (12–14). We recently reported that age increased lower extremity stiffness with healthy elderly adults using approximately 50% greater lower extremity stiffness while stepping down compared with healthy young adults (15). Lower extremity stiffness can be altered by changing the kinematics of the limb at touchdown and during the impact phase. Lower extremity stiffness is decreased with greater joint flexion, which alters the direction of the ground reaction force vector in relation to the limb segments and joints (14,16–21). Elderly adults stepped down with 42% less ankle dorsiflexion and 57% less knee flexion, maintaining a more erect posture com- pared with young adults (15). The more erect posture aligned the ground reaction force vector closer to the joint centers, reducing external torques and the contribution of the musculature to limb stiffness. Lower extremity stiffness is thus a function of skeletal and muscular components with stiffer limbs having a larger skeletal component. If the knee is fully extended and the ankle dorsiflexed while descending stairs and a purely vertical force is applied to the heel, the force passes directly along the tibia and femur and through the centers of the ankle, knee, and hip joints. Support would come entirely from the skeletal system, and force from the musculature would not be required (Figure 1). With greater knee flexion and ankle plantarflexion, the skeletal segments are no longer vertical, and the force vector would point across the foot, leg, and thigh and away from the joint centers. In such a limb orientation the muscular component of limb stiffness increases and the skeletal component decreases. The force applied to the limb during stair descent also has a horizontal component (1) that decreases the force magnitude applied along the longitudinal axis of the leg and thigh. The influence of the skeletal system on lower extremity stiffness has been investigated in young adults performing a variety of movements (12–21). The influence of the musculature on upper and lower extremity stiffness has been reported for young adults. These studies have shown that muscle stiffness is directly related to joint stiffness and to the control of limb movements, limb length, and limb stiffness (17,22–26). McIntyre and colleagues (26), for example, investigated control strategies for maintaining stable upper extremity postures under applied loads. Limb stiffness and limb stability were maintained by increasing joint stiffness. Joint stiffness was increased by increasing muscle force, which increased muscle stiffness. Grillner (24) showed that gastrocnemius muscle stiffness can be used to stabilize the length of the extremity during locomotion because of the stretch imposed on the muscle, which increases B593 B594 DEVITA AND HORTOBAGYI no subjects withdrew from the study because of an inability to step down. All subjects provided written informed consent prior to testing. Figure 1. If the knee is fully extended and the ankle is dorsiflexed while descending stairs and a purely vertical force is applied to the heel, the force passes directly along the tibia and femur and through the centers of ankle, knee, and hip joints. Support would come entirely from the skeletal system, A. With greater knee flexion and ankle plantarflexion, the skeletal segments are no longer vertical, and the force vector would point across the foot, leg, and thigh and away from the joint centers. In such a limb orientiation the muscular component of limb stiffness increases and the skeletal component decreases, B. muscle stiffness. Gottlieb (23) and Millner and colleagues (25) showed that increasing cocontraction of muscle groups on two sides of a skeletal joint increases joint stiffness and therefore the stability of the extremity. Little is known, however, about the combined contribution of each component to lower extremity stiffness during daily activities in any population. The purpose of this study was to compare the skeletal and muscular components of lower extremity stiffness between elderly and young adults during step-down movements. Along with the age-related delays in neuromuscular function described above, most elderly adults have lower muscle strength and power capabilities than young adults (27–31). Because of these declines in muscular capabilities with age, we hypothesize that elderly adults will rely more on their skeletal system than young adults and will therefore have a larger ratio of skeletal-to-muscular components of lower extremity stiffness compared with young adults. METHODS Subjects Fourteen elderly and 16 young adults volunteered. Elderly adults were, on average, 49.3 years older than young adults (elderly mean ⫾ SD, 70.1 ⫾ 6.7 years; young mean ⫾ SD, 20.8 ⫾ 1.8 years). Mass and height were similar between the groups: Elderly adults averaged 69.9 ⫾ 16.1 kg and 1.61 ⫾ 0.09 m, and young adults averaged 65.7 ⫾ 8.7 kg and 1.67 ⫾ 0.08 m in mass and height. All subjects were apparently healthy, and elderly subjects provided a physician’s approval to participate in the study. The elderly subjects lived independently and reported that they performed activities of daily living with little or no difficulty. We observed that the elderly subjects moved around the laboratory with confidence and without balance-related problems. The testing protocol was readily performed by all subjects, and Experimental Set-up One of two wooden platforms was positioned next to a force plate (AMTI; model LG 6-4-1, Newton, MA). Heights of the wooden platforms were 10% and 20% of the subject’s standing height. The 10% height, which averaged 0.164 m, was similar to a normal stairway step, and the 20% height represented a relatively large step-down distance. The force plate measured vertical and anteroposterior floor reaction forces and the mediolateral force plate moment under the forward stepping limb at 1000 Hz. Sagittal plane video recordings (SONY CCD-Iris camera, Tokyo, Japan, and JVC VCR model HR S5100, Elmwood Park, NJ) were made of the stepping-down movement at 60 Hz. The field of view for the video image was approximately 1.5 m high and 2.5 m wide, which maximized the image size of the lower extremity. Testing Protocol Subjects wore black spandex bike shorts, a tight fitting t-shirt, and athletic shoes. Their height and mass were measured before the first trial. Reflective markers were placed on the subjects’ right side on the lateral border of their fifth metatarsal head, the heel of the shoe, lateral malleolus, lateral femoral epicondyle, and greater trochanter. All subjects practiced the step-down movements until they were comfortable, after which five successful step-down trials were recorded for each height. Each trial consisted of the subject standing on the front edge of the platform, stepping down with the right limb, and contacting the force plate with the forefoot. The subject then lifted the left foot off the raised platform and stepped forward past the force plate. The stepdown movements were generally easy to perform and did not present difficult balancing problems. No subjects reported fatigue during the test session. The order of stepping height tests was counterbalanced across subjects. Data Analysis Cartesian coordinates of the reflective markers were derived from the video records starting with the frame of forefoot contact with the force plate until the frame of maximum knee flexion using the Peak5 system (Peak Performance Technologies, Englewood, CO). High-frequency error was removed from the digitized coordinates with an automatic, low-pass digital filter using an average cut-off frequency of about 7 Hz. The lower extremity was modeled as a linear spring and was defined as the line between the metatarsal head and the hip joint (Figure 2) (15). Lower extremity stiffness was measured during the impact phase of stepping down, which was the period between initial contact with the force plate and the occurrence of the maximum ground reaction force. Stiffness was computed as the ratio of the maximum force applied to the lower extremity during the impact phase (Fmax) and the resultant shortening of the lower extremity (Xmax) (12,13,17,18). Fmax was the component of the ground reaction force vector applied at the metatarsal head AGE AND LOWER EXTREMITY STIFFNESS and directed along the line to the hip joint (Figure 2). Xmax was calculated as the difference in the length of the distance between the metatarsal head and hip from initial contact until the occurrence of Fmax. The center of pressure was used to validate the application of the force to the metatarsal head and indicated that the floor reaction force was applied within 1 cm of this position. Lower extremity stiffness represents the combined stiffness of all tissues in the extremity but is primarily an assessment of the skeletal and muscular contributions to support against collapse. Fmax tends to cause the extremity to flex at one or more joints, and therefore the distance between the hip joint and metatarsal heads shortens. The amount of shortening will be proportional to the muscular stiffness crossing the joint or joints (17,24) and to the skeletal kinematics in relation to the point of application and direction of the applied force (14,16,17,19). A model was developed to partition the observed stiffness into skeletal and muscular components on the basis of the position of the lower extremity segments and the direction of Fmax. Skeletal and muscular components of lower extremity stiffness were calculated as a function of the angle between Fmax and the leg with 2 2 k = k cos φ + k sin φ, (1) where k ⫽ observed lower extremity stiffness, ⫽ the angle between Fmax and the leg, k cos2 ⫽ the skeletal component, and k sin2 ⫽ the muscular component (Figure 2). A completely extended and vertically oriented extremity impacting the floor after a vertical descent would have ⫽ 0 and all stiffness due to the skeletal component. The muscular component increases as knee flexion and ankle plantar- Figure 2. Stepping down begins with floor contact in a relatively erect position, A, and proceeds to a more flexed position with an applied force, B. Skeletal and muscular components of lower limb stiffness were calculated as a function of the angle between Fmax and the leg with: k ⫽ k cos2 ⫹ k sin2 , where k ⫽ observed lower extremity stiffness, ⫽ angle between Fmax and the leg, k cos2 ⫽ skeletal component, and k sin2 ⫽ muscular component. A completely extended and vertically oriented limb impacting the floor after a vertical descent would have ⫽ 0 and all stiffness due to the skeletal component. The muscular component increases as knee flexion and ankle plantarflexion increase, and the descent trajectory includes a horizontal component, making ⬎ 0. B595 flexion increase, and the descent trajectory includes a horizontal component, making ⬎ 0. The relative contribution of skeletal to muscular components was assessed by a ratio of the two components (skeletal/muscular). Our pilot data indicated the angles between the leg and force vector and between the thigh and force vector were within a few degrees of each other. The femoral and tibial influences to the skeletal component are therefore both accounted for in the model. Validity of Stiffness Calculation Both groups had similar kinematics at initial contact with the force plate. The mean lengths of the lower extremity for young and elderly subjects across both step heights were 0.916 m and 0.915 m, respectively, at floor contact. The length of the lower extremity was reduced during the impact phase of the step-down movement because of ankle dorsiflexion and knee flexion (Figures 3 and 4). The extremity shortened during the application of the ground reaction force, and maximum shortening was attained at about the same time as the occurrence of Fmax. The displacement and force characteristics observed during the impact phase of stepping down therefore were fundamentally identical to those observed during the impact phases of hopping and running. The assessment of lower extremity stiffness in stepping down seems appropriate. We compared our method of calculating stiffness with that of Farley and Gonzalez (13) during both running and step-down movements. Running analyses were based on Laboratory data (n ⫽ 12). The results from the present method were in close agreement with those from Farley and Gonzalez. Lower extremity stiffness during running was highly correlated with both stiffness coefficients predicted by the Farley and Gonzalez method (r for kleg ⫽ 0.827, r for kvert ⫽ 0.838). The slope of the regression line between our method and kvert was close to unity (1.09), and the y-inter- Figure 3. Ankle and knee joint positions during the impact phase of stepping down from representative trials in the 20% height condition. Positive ankle position is plantarflexion and negative knee position is flexion. Young and elderly subjects had similar amounts of ankle plantarflexion and knee flexion as they contacted the force plate. Young subjects dorsiflexed more at the ankle and flexed more at the knee during a longer impact phase compared with elderly subjects. B596 DEVITA AND HORTOBAGYI Figure 4. Ground reaction force (GRF) and the resultant shortening of the extremity during the impact phase from the trials in Figure 3. Fmax values were similar between age groups, but the elderly subjects reached Fmax in less time. Young subjects shortened their lower extremity more during the impact phase, and maximum shortening occurred at about the same time as Fmax, as indicated by the arrows. Xmax was calculated as the amount of shortening between initial contact (time ⫽ 0.0 s) and Fmax. Xmax values for these trials were 0.075 m for young subjects and 0.040 m for elderly subjects. cept (⫺2.6 kN/m) was close to zero. The mean lower extremity stiffness for the present method (24.9 kN/m) was within 2% of kvert from Farley and Gonzalez’s method (24.6 kN/m) over all trials. We had to modify Farley and Gonzalez’s (13) methods to calculate the center of mass displacement during the stepdown movement. Trials from five subjects were redigitized using 15 body points from which the vertical position and displacement of the body center of mass were calculated during the impact phase. Present lower extremity stiffness (mean, 21.9 kN/m) and kvert (mean, 19.9 kN/m) were within 7% on a trial-by-trial basis. The correlation coefficient between these methods was excellent (r ⫽ 0.982), the slope of the regression line was good (1.24), and the y-intercept (–2.9 kN/m) was relatively close to zero. We conclude that the present methods for calculating lower extremity stiffness were reasonable and valid. Statistical Analysis Four variables, , skeletal and muscular stiffness components, and the ratio of the components, were averaged across the five trials for each subject and condition set of trials. The mean values were then entered as the subject scores into a two-way analysis of variance (ANOVA). The two factors were age (independent factor) and step height (repeated factor),and the alpha level was set at .05. RESULTS We previously reported (15) that lower extremity stiffness was 50% larger and that lower extremity compression was 28% lower (both p ⫽ .0001) in the elderly adults compared with the young adults tested in this study (Table 1). In contrast, the maximum force was only 3% larger in the elderly subjects and not significantly different. We also reported that step height had statistically significant effects on Xmax and Fmax. Xmax was 27% larger and Fmax was about 50% larger (both p ⬍ .0001) with the 20% step height compared with the 10% height. The increased force was offset by the larger amount of limb shortening such that lower extremity stiffness was not significantly different between step heights. The important variable in the assessment of skeletal and muscular components of lower extremity stiffness was the angle between the leg and Fmax, . ANOVA revealed no significant interaction effect for the angle , but it did reveal significant main effects for age and step height (Figure 5). Angle was 16% smaller (F ⫽ 5.64, p ⬍ .03) in elderly adults (16.0 ⫾ 3.0⬚) compared with young adults (19.0 ⫾ 4.3⬚), and it was 29% larger (F ⫽ 65.9, p ⬍ .0001) in the 20% step height (20.0 ⫾ 3.5⬚) compared with the 10% (15.5 ⫾ 2.8⬚) step height. There were no significant interaction or step height effects for the skeletal component to lower extremity stiffness, but there was a significant age effect (Figure 6). The skeletal component was 48% larger (F ⫽ 7.63, p ⬍ .025) in elderly adults (30.8 ⫾ 13.6 kN/m) compared with young adults (20.8 ⫾ 5.4 kN/m). There were no significant interaction or age effects for the muscular component to lower extremity stiffness, but there was a significant step height effect (Figure 7). The muscular component was 78% larger (F ⫽ 52.9, p ⬍ .0001) in the 20% step (3.2 ⫾ 1.1 kN/m) compared with the 10% step (1.8 ⫾ 0.6 kN/m). There was no significant interaction effect for the ratio of skeletal to muscular components of lower extremity stiffness, but there were significant age and step height effects (Figure 8). The ratio was 32% larger (F ⫽ 8.64, p ⬍ .01) in elderly adults (12.7 ⫾ 4.4) compared with young adults (9.6 ⫾ 3.9), and it was 38% less (F ⫽ 60.1, p ⬍ .0001) in the 20% step height (8.5 ⫾ 3.2) condition compared with the 10% step height condition (13.8). DISCUSSION The present study identified the contribution of skeletal and muscular components to total lower extremity stiffness. The basic premise was that through the combined action of skeletal and muscular components, the lower extremity resists the compressive effect or tendency of external forces. Partitioning lower extremity stiffness into the two components provides a method to assess a person’s reliance on passive skeletal and active muscular components to support the body during locomotion. This assessment is novel and has not been reported previously. Such an analytical method may provide a tool for quantitatively assessing decline in functional performance with aging or with a sedentary lifeTable 1. Mean (⫾SD) Lower Extremity Stiffness Values From Reference (15) Group Elderly adults Young adults 10% Height 20% Height Stiffness (kN/m) Xmax (m) Fmax (N) 33.4 ⫾ 14.3* 22.4 ⫾ 6.2 26.5 ⫾ 10.4 28.0 ⫾ 13.3 0.041 ⫾ 0.015* 0.057 ⫾ 0.016 0.043 ⫾ 0.015** 0.055 ⫾ 0.017 1255 ⫾ 476 1219 ⫾ 302 972 ⫾283** 1454 ⫾ 325 *Elderly adults significantly different from young adults, p ⬍ .05. **10% height significantly different from 20% height, p ⬍ .05. AGE AND LOWER EXTREMITY STIFFNESS Figure 5. Group means (SD) for the angle between Fmax vector and the leg. was 21% smaller (p ⬍ .03) in elderly adults (n ⫽ 14) compared with young adults (n ⫽ 16), and it was 29% larger (p ⬍ .0001) in the 20% step height compared with the 10% step height. The interaction effect was not significant. style and improvements in functional performance in the elderly population with training or rehabilitation. It is well established that stair descent is difficult for some elderly adults and that many accidents occur during this activity (32,33). It is also well known that resistance training increases muscular strength in elderly adults (34–36) but that strength improvements may or may not lead to improvements in functional tasks (34,35,37–39). The application of the current methods to stair descent and other movements may provide an assessment of the mechanism for any improved or unaffected performance by identifying the amount of increase or lack of increase in the muscular component to limb support. We propose that the optimal ratio of skeletal and muscular components enables safe, successful movement while an inappropriate ratio creates balance problems and excessive stress on the skeletal or muscular systems. This ratio has yet to be determined. Elderly adults clearly relied more on their skeletal system to support themselves during stepping down than did young adults. The skeletal component to lower extremity stiffness was nearly 1.5 times larger, and the ratio of skeletal to muscular components was about 1.3 times larger in elderly Figure 6. Group means (SD) for the skeletal component of lower extremity stiffness. Skeletal component was 48% larger (p ⬍ .025) in elderly adults (n ⫽ 14) compared with young adults (n ⫽ 16). Step height had no effect on the skeletal component, and the interaction effect was not significant. B597 Figure 7. Group means (SD) for the muscular component of lower extremity stiffness. The muscular component was 74% larger ( p ⬍ .0001) in the 20% step compared with the 10% step (n ⫽ 30) while age had no effect on the muscular component. The interaction effect was not significant. adults compared with young adults. This ratio identifies the relative functional dependence each group had on their skeletal and muscular systems. Elderly adults increased the skeletal component by keeping Fmax closer to or more in line with the leg. They performed stepping down in a more erect posture. This posture shortened the moment arm for Fmax at the knee and therefore reduced the flexor torque that tended to cause collapse (13,15,16,18,21). This strategy enabled the elderly adults to step down with a smaller muscular contribution to lower extremity stiffness. The observed age-related adaptations are thought to have been previously learned and used during daily step-down movements and are not due solely to the step-down task in the study. Elderly adults probably selected this strategy for several reasons. First, the elderly subjects had lower muscle strength compared with the young subjects. These subjects were tested isokinetically as part of another study, and the peak concentric and eccentric torques were 47% and 23% Figure 8. Group means (SD) for the ratio of skeletal-to-muscular components of lower extremity stiffness. The ratio was 32% larger (p ⬍ .01) in elderly adults (n ⫽ 14) compared with young adults (n ⫽ 16), and it was 38% less (p ⬍ .0001) in the 20% step height condition compared with the 10% step height condition. Elderly adults had a greater relative reliance on their skeletal system compared with their musculature for lower extremity stiffness during stepping down compared with young adults. The interaction effect was not significant. B598 DEVITA AND HORTOBAGYI lower in the elderly group (unpublished data). Along with this difference, present elderly subjects probably had lower muscle power (40–42) and a lower rate of muscle force and torque production (9–11) compared with the young subjects. The stiffer movement strategy reduced the load on the muscular component and therefore reduced the possibility of collapse in the elderly subjects. Second, stepping down requires mostly eccentric muscle contraction to control and stop the downward motion of the body (1). Elderly adults have been shown to retain eccentric muscle function more so than concentric function [present subjects and (10,43,44)]. Porter and colleagues (10), in fact, showed only a 3% reduction in peak eccentric plantarflexor torque in a group of 67-year-old subjects compared with a group of 27year-old subjects. Although elderly adults may have reasonable eccentric muscle capabilities, the present data suggest that elderly subjects may not fully employ them in functional activities. The increased limb stiffness may be the result of the aged neuromuscular system’s attempt to reduce the range of flexion and dorsiflexion in order to resolve the control complexity of eccentric contractions by the extensor and plantarflexor muscles (15,45). Third, elderly adults may have selected this movement strategy to reduce compressive forces inside the knee joint even though these subjects did not have histories of knee joint degeneration. Most of the compressive, bone-on-bone force inside lower extremity joints is due to the force developed by muscular contraction (46–48). The elderly subjects may perceive greater comfort and less joint stress with the stiffer strategy and a greater reliance on skeletal rather than muscular components to lower extremity stiffness. Finally, elderly adults may select a stiffer, more skeletal-oriented strategy to reduce the contractile effort of the muscles and the development of muscle fatigue. Alexander (21) demonstrated that humans and other animals would perform less mechanical work and expend less metabolic energy if they were to keep the ground reaction force vector closer to the leg and hip and if they were to walk erect with little joint flexion. DeVita and Skelly (16) demonstrated that joint torques generated by the musculature do less work in stiffer, more erect landings than in less stiff landings with more joint flexion. We do not mean that elderly subjects became fatigued during the present tests but that they used a previously learned strategy in this study. One negative consequence of these age-related adaptations is that they may increase the incidence of falling accidents during stepping down or while descending stairs. The reduced reliance on muscles may provide safer movements for elderly adults in well-performed step-down movements. However, in a single movement that is performed poorly, the stiffer, skeletal-oriented strategy may reduce the ability of the person to take corrective actions before falling. For example, a single step may be lower than others in the stairway and cause a larger-than-normal and off-balance impact onto the person. Stepping down with a larger muscular component may enable the person to absorb the unexpected impact successfully (16,19,20), whereas a person using a greater skeletal component may be forced off balance because impacts to stiffer lower extremities occur in shorter times compared with impacts to less stiff limbs (13,14,18). Indeed, the elderly subjects performed the movement from initial contact to maximum force in 18% less time (p ⬍ .05) compared with the young subjects (elderly, 0.095 ⫾ 0.024 s; young, 0.116 ⫾ .027 s), showing that the elderly subjects have less time to adapt to any unexpected forces. We previously reported that step height had no significant effect on lower extremity stiffness (15). Step height did affect the biomechanics of stepping down, however, and the components of lower extremity stiffness. Stepping down from the taller step caused the subjects to flex 45% more at the knee (10%: 18.2 ⫾ 4.5° vs 20%: 26.4 ⫾ 5.8°; F ⫽ 109, p ⬍ .0001) to compensate for the 50% increase (F ⫽ 95.8, p ⬍ .0001) in Fmax (15). This altered strategy increased the muscular component 74% and decreased the skeletal-tomuscular ratio 38% in the taller step. Young and elderly humans respond to increased impact forces in stepping down by altering their lower extremity kinematics and by increasing the muscular contribution to lower extremity stiffness and support. Stepping down from taller steps, therefore, can be problematic for elderly adults because they rely more on their skeletal component. The results suggest that stairway design can be improved for elderly adults if it incorporates lower step heights compared with standard heights used in homes and buildings. The present analytical approach is new, and its assumptions warrant discussion. It is generally accepted that muscles, and not other passive tissues, are mainly responsible for the generation of net muscle moments around joints. This assumption has been accepted in gait and other fullbody movement studies (1,16,49,50), in isokinetic tests of joint torques (51), in motor control studies on joint stiffness (25), and in studies on muscle stiffness and its relationship to joint torques (22,24). Vrahas and colleagues (50) directly investigated the contribution of various tissues to torque generation at the hip joint. They reported that passive structures such as joint capsules and ligaments contribute a small portion to the total torque, usually less than 10%, when compared with the torque produced by the muscular system. Because the muscles are the main torque producers that control joint rotations and the overall orientation of the lower extremity, it is reasonable to propose that the muscular component contributes to lower extremity stiffness. The skeletal component to lower extremity stiffness has been indirectly demonstrated in several studies (12–17,19). Each of these studies identified the relationship between lower extremity stiffness and the kinematics of the skeletal system during movement. The fundamental result was that as joint flexion decreased, lower extremity stiffness increased. Farley and colleagues (17) demonstrated this relationship in hopping as did DeVita and Skelly (16) in landing from a jump. Lower extremity stiffness was increased by reducing the amount of knee flexion and by reducing the moment arm of Fmax. This kinematic adjustment brought the force vector more parallel to the leg, shortening its moment arm and reducing the need for muscular contribution. This adjustment effectively increased the skeletal component to lower extremity stiffness. If the knee joint were completely extended, the muscular component would be eliminated, and the skeletal component would be maximized. However, this strategy is not used in normal human movement be- AGE AND LOWER EXTREMITY STIFFNESS cause the skeleton would reach yield strength and fail (fracture). As knee flexion increases and the skeletal segments are no longer vertically positioned, the muscular component will be increased and the skeletal component will be decreased with a vertically applied force. On the basis of the biomechanics literature concerning many types of impacts to the lower extremities, it seems reasonable to attribute lower extremity stiffness to skeletal and muscular components. 11. 12. 13. 14. 15. Conclusions We previously reported that lower extremity stiffness was 50% greater in elderly adults compared with young adults (15). The present results identify one mechanism used by elderly adults to increase their lower extremity stiffness. Changes in lower extremity stiffness with age were due to a shift in the relative contribution of the components of lower extremity stiffness. Elderly adults increased their dependence on the skeletal system and reduced their dependence on the muscular system leading to a greater skeletalto-muscular ratio. This strategy was achieved by decreasing the amount of flexion in the joints and by reducing the angle between the maximum force vector and the leg. The results supported the hypothesis that elderly adults will have greater relative skeletal and lower relative muscular components of lower extremity stiffness compared with young adults. The age-related adaptations allowed the elderly subjects to successfully step down from a height used in stairways and from a taller height despite having reduced neuromuscular capabilities compared with young adults. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. Acknowledgments This work was supported in part by Research and Creative Activity grants from East Carolina University (P.D. and T.H.), a North Carolina Institute on Aging grant (P.D.), and a National Institute of Child Health and Human Development Grant 30422 (T.H.). We thank Mr. Jeff Money and Mr. Jason Barrier for their work in the data collection and analysis portions of the study. We also thank Dr. Robert Hickner and Dr. Kevin O’Brien for their constructive comments on the procedures used in this work. Address correspondence to Paul DeVita, PhD, Department of Exercise and Sport Science, East Carolina University, Greenville, NC 27858. E-mail: [email protected] 26. 27. 28. 29. 30. References 1. McFadyen B, Winter D. An integrated biomechanical analysis of normal stair ascent and descent. J Biomech. 1988;21:733–744. 2. Elftman H. Forces and energy changes in the leg during walking. Am J Physiol. 1939;125:339–356. 3. Bressler B, Frankel JP. The forces and moments in the leg during level walking. Trans ASME. 1950;72:27–36. 4. Hamill J, McNiven S. Reliability of selected ground reaction force parameters during walking. Human Movt Sci. 1990;9:117–131. 5. Giakas G, Baltzopoulos V. Time and frequency domain analysis of ground reaction forces during walking: an investigation of variability and symmetry. Gait Posture. 1997;5:189–197. 6. Welford AT. Reaction time, speed of performance and age. Ann NY Acad Sci. 1988;515:1–17. 7. Leonard CT, Matsumoto T, Diedrich PM, McMillan JA. Changes in neural modulation and motor control during voluntary movement of older individuals. J Gerontol Med Sci. 1997;52A:M320–M325. 8. Petrella RJ, Lattanzio PJ, Nelson MG. Effect of age and activity on knee joint proprioception. Am J Phys Med Rehabil. 1997;76:235–241. 9. Thelen DG, Schultz AB, Alexander NB, Ashton-Miller JA. Effects of age on rapid ankle torque development. J Gerontol Med Sci. 1996; 51A:M226–M232. 10. Porter MM, Vandervoort AV, Kramer JF. Eccentric peak torque of the 31. 32. 33. 34. 35. 36. 37. B599 plantar and dorsiflexors is maintained in older women. J Gerontol Biol Sci. 1997;52A:B125–B131. Davies CTM, Thomas DO, White MJ. Mechanical properties of young and elderly human muscle. Acta Med Scand. (suppl) 1986;711:219–226. Blickhan R. The spring-mass model for running and hopping. J Biomech. 1989;22:1217–1227. Farley CT, Gonzalez O. Leg stiffness and stride frequency in human running. J Biomech. 1996;29:181–186. McMahon TA, Valiant G, Frederick EC. Groucho running. J Appl Physiol. 1987;62:2326–2337. Hortobagyi T, DeVita P. Altered movement strategy increases lower extremity stiffness during stepping down in the aged. J Gerontol Biol Sci. 1999;54A:B63–B70. DeVita P, Skelly WA. Effect of landing stiffness on joint kinetics and energetics in the lower extremity. Med Sci Sports Exerc. 1992;24:108–115. Farley CT, Houdijk JH, van Strien C, Louie M. Mechanism of leg stiffness adjustment for hopping on surfaces of different stiffnesses. J Appl Physiol. 1998;85:1044–1055. Ferris DP, Farley CT. Interaction of leg stiffness and surface stiffness during human hopping. J Appl Physiol. 1997;82:15–22. Lafortune MA, Lake MJ, Hennig EM. Differential shock transmission response of the human body to impact severity and lower limb posture. J Biomech. 1996;29:1531–1537. Derrick T, Hamill J, Caldwell G. Energy absorption of impacts during running at various stride lengths. Med Sci Sports Exerc. 1998;30:128–135. Alexander RM. Energy saving mechanisms in walking and running. J Exp Biol. 1991;160:55–69. Gollhofer A, Schmidtbleicher D, Dietz V. Regulation of muscle stiffness in human locomotion. Int J Sports Med. 1984;5:19–22. Gottlieb GL. Muscle compliance: implications for the control of movement. In: Holloszy J, ed. Exercise and Sport Science Reviews. Baltimore, MD: Williams and Wilkins; 1996:1–34. Grillner S. The role of muscle stiffness in meeting the changing postural and locomotor requirements for force development by the ankle extensors. Acta Physiol Scand. 1972;86:92–108. Milner TE, Cloutier C, Leger AB, Franklin DW. Inability to activate muscles maximally during cocontraction and the effect on joint stiffness. Exp Brain Res. 1995;107:293–305. McIntyre J, Mussa-Ivaldi FA, Bizzi E. The control of stable postures in the mulitjoint arm. Exp Brain Res. 1996;110:248–264. Bassey EJ. Longitudinal changes in selected physical capabilities: muscle strength flexibility and body size. Age and Aging. 1998; 27(suppl 3):12–16. Vandervoort AA, Kramer JF, Wharram ER. Eccentric knee strength of elderly females. J Gerontol Biol Sci. 1990;45:B125–B128. Metter EJ, Conwit R, Tobin J, Fozard JL. Age-associated loss of power and strength in the upper extremities in women and men. J Gerontol Biol Sci. 1997;52A:B267–B276. Larsson L, Grimby G, Karlsson J. Muscle strength and speed of movement in relation to age and muscle morphology. J Appl Physiol. 1979; 46:451–456. Seiler KS, Spirduso WW, Martin JC. Gender differences in rowing performance and power with aging. Med Sci Sports Exerc. 1998;30: 121–127. Tinetti ME, Doucette JT, Claus EB. The contribution of predisposing and situational risk factors to serious fall injuries. J Am Geriatr Soc. 1995;43:1207–1213. Archea JC. Environmental factors associated with stair accidents by the elderly. Clin Geriatr Med. 1985;1:555–568. Buchner DM, Cress ME, de Lateur BJ, et al. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J Gerontol Med Sci. 1997;52A:M218– M224. Chandler JM, Duncan PW, Kochersberger G, Studenski S. Is lower extremity strength gain associated with improvement in physical performance and disability in frail, community-dwelling elders? Arch Phys Med Rehabil. 1998;79:24–30. Sipila S, Multanen J, Kallinen M, Era P, Suominen H. Effects of strength and endurance training on isometric muscle strength and walking speed in elderly women. Acta Physiol Scand. 1996;156:457–464. Brown M, Holloszy JO. Effects of low intensity exercise program on selected physical performance characteristics of 60 to 71 year olds. Aging. 1991;3:129–139. B600 DEVITA AND HORTOBAGYI 38. Brown M, Sinacore DR, Host HH. The relationship of strength to function in the older adult. J Gerontol Med Sci. 1995;50A:M55–M59. 39. Judge JO, Underwood M, Gennosa T. Exercise to improve gait velocity in older persons. Arch Phys Med Rehabil. 1993;74:400–406. 40. Bassey EJ. Measurement of muscle strength and power. Muscle Nerve. 1997;5(suppl):S44–S46. 41. DeVito G, Bernardi M, Forte R, Pulejo C, Macaluso A, Figura F. Determinants of maximal instantaneous muscle power in women aged 50–75 years. Eur J Appl Physiol. 1998;78:59–64. 42. Metter EJ, Conwit R, Tobin J, Fozard JL. Age-associated loss of power and strength in the upper extremities in women and men. J Gerontol Biol Sci. 1997;52A:B267–B276. 43. Hortobagyi T, Zheng D, Weidner M, Lambert NJ, Westbrook S, Houmard JA. The influence of aging on muscle strength and muscle fiber characteristics with special reference to eccentric strength. J Gerontol Biol Sci. 1995;50A:B399–B406. 44. Poulin MJ, Vandervoort AA, Paterson DH, Kramer JF, Cunningham DA. Eccentric and concentric torques of knee and elbow extension in young and older men. Can J Sport Sci. 1992;17:3–7. 45. Enoka RM. Eccentric contractions require unique activation strategies by the nervous system. J Appl Physiol. 1996;81:2339–2346. 46. Glitsch U, Bauman W. The three dimensional determination of internal loads in the lower extremity. J Biomech. 1997;30:1123–1131. 47. Scott SH, Winter DA. Internal forces at chronic running injury sites. Med Sci Sports Exerc. 1990;22:357–369. 48. Simpson KJ, Kanter L. Jump distance of dance landings influencing internal joint forces: I. axial forces. Med Sci Sports Exerc. 1997;29: 916–927. 49. Winter DA. Overall principle of lower limb support during stance phase of gait. J Biomech. 1980;13:923–927. 50. Vrahas MS, Brand RA, Brown TD, Andrews JG. Contribution of passive tissues to the intersegmental moments at the hip. J Biomech. 1990;23:357–362. 51. Hortobagyi T, Barrier J, Beard D, et al. Greater initial adaptations to submaximal muscle lengthening than maximal shortening. J Appl Physiol. 1996;81:1677–1682. Received March 12, 1999 Accepted June 9, 2000 Decision Editor: Jay Roberts, PhD