Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
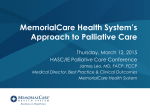
Support Care Cancer (2015) 23:1073–1080 DOI 10.1007/s00520-014-2460-4 ORIGINAL ARTICLE The oncology palliative care clinic at the Princess Margaret Cancer Centre: an early intervention model for patients with advanced cancer Breffni Hannon & Nadia Swami & Ashley Pope & Gary Rodin & Elizabeth Dougherty & Ernie Mak & Subrata Banerjee & John Bryson & Julia Ridley & Camilla Zimmermann Received: 2 May 2014 / Accepted: 22 September 2014 / Published online: 4 October 2014 # Springer-Verlag Berlin Heidelberg 2014 Abstract Several recently published randomized controlled trials have demonstrated the benefits of early palliative care involvement for patients with advanced cancer. In the oncology outpatient setting, palliative care clinics are an ideal site for the provision of early, collaborative support, which can be maintained throughout the cancer trajectory. Despite this, access to ambulatory palliative care clinics is limited, even at tertiary cancer centres. Existing programs for outpatient palliative care are variable in scope and are not well described in the literature. We describe the development and expansion of an outpatient palliative care clinic at the Princess Margaret Cancer Centre, Toronto, Canada, demonstrating how the clinic functions at a local and regional level. This clinic served as the intervention for a recent large cluster-randomized trial of early palliative care. The model for this service can be adapted by other palliative care programs that aim to provide early, integrated oncology care. B. Hannon : J. Bryson : C. Zimmermann Division of Medical Oncology & Hematology, Department of Medicine, University of Toronto, Toronto, Canada E. Mak : S. Banerjee : J. Ridley Division of Palliative Care, Department of Family and Community Medicine, University of Toronto, Toronto, Canada G. Rodin : C. Zimmermann Department of Psychiatry, University of Toronto, Toronto, Canada B. Hannon : N. Swami : A. Pope : G. Rodin : E. Dougherty : E. Mak : S. Banerjee : J. Bryson : J. Ridley : C. Zimmermann (*) Department of Psychosocial Oncology and Palliative Care, Princess Margaret Cancer Centre, University Health Network, 610 University Ave., 16-712, Toronto, Ontario M5G 2 M9, Canada e-mail: [email protected] G. Rodin : C. Zimmermann Campbell Family Cancer Research Institute, Princess Margaret Cancer Centre, University Health Network, Toronto, Canada Keywords Palliative care . Advanced cancer . Early intervention . Outpatient clinic Introduction Early integration of specialized palliative care for patients with advanced cancer leads to improved patient outcomes [1–4] and is increasingly recommended [5–7], but remains the exception rather than the norm. Specialized palliative care services have traditionally been provided for inpatients, in palliative care units and by consultation services [8]. However, most cancer care occurs on an outpatient basis, and in order for palliative care to be integrated early, outpatient palliative care consultations and follow-up are necessary. Palliative care clinics provide an ideal venue for early palliative care involvement and for the collaborative integration of palliative care into routine cancer care [1, 9–11]. However, many treatment centres still do not have outpatient palliative care clinics [9, 12], and there have been few descriptions of such clinics in the medical literature [13]. One narrative review of 20 clinics has been published, but this review presented summary statistics rather than describing the detailed operational functioning of individual clinics [14]. Here we describe the development and structure of an oncology palliative care clinic (OPCC) in Toronto, Canada, which is integrated within a palliative care program at a comprehensive cancer centre and university hospital. This clinic was the main venue for an early palliative care intervention, which resulted in improved quality of life and increased satisfaction with care for patients with a wide range of cancer types [3]. We will describe how the clinic functions and how it is integrated into the cancer program, both at the cancer centre and regionally, within the cancer system in Toronto and Ontario. 1074 Palliative care in Toronto, Canada Toronto is the capital of the province of Ontario, and the largest city in Canada, with a population of approximately 3 million (5.5 million in the Greater Toronto Area). Ontario is divided into 14 health regions, or Local Health Integration Networks (LHINs), which are responsible for health services in their communities, including hospitals and community care services. The latter are provided by Community Care Access Centres (CCACs), which organize and coordinate home care provided by nurses, physiotherapists, social workers, dietitians, occupational therapists, personal support workers and others, as well as providing home equipment and a drug benefit program. Application for CCAC services requires completion of an electronic referral form, and the CCAC staff work in close collaboration with the referring physician, who may be a specialist or family physician, with an office- or community-based practice. The range of services and maximum nursing time provided are based on prognosis (estimated by the referring physician) and on performance status, as measured by the Palliative Performance Scale (PPS) [15, 16]. Palliative care in Toronto is provided by hospital-based palliative care services, in acute and community palliative care units, in hospices and at home. Home palliative care, including 24-h on-call coverage, is provided mainly by community-based groups of physicians dedicated to providing palliative care for patients in their community. These physicians work closely with the CCAC and family physicians in their area and provide either primary palliative care or consultative care. Because most family physicians in Toronto have office-based practices and rarely do house calls, specialized home palliative care physicians provide most of the home palliative care in Toronto. However, Cancer Care Ontario, the provincial cancer control agency, has recently undertaken several initiatives to increase the palliative care involvement of primary care physicians [17]. Support Care Cancer (2015) 23:1073–1080 The palliative care program at PM is housed within the Department of Psychosocial Oncology and Palliative Care. In addition to daily palliative care clinics, the palliative care program also has a 12-bed acute palliative care unit (the Lederman Palliative Care Centre) [18] and a 10-bed residential hospice (Kensington Hospice). It is also part of the larger UHN palliative care program that includes inpatient consultation services at all sites [19]. This represents one of the most comprehensive programs available in a North American cancer centre and encompasses all of the key operational features for hospital palliative care programs as outlined by the Center to Advance Palliative Care [8]. Philosophy and evolution of the oncology palliative care clinic The OPCC provides a venue for specialized early palliative care of ambulatory patients with cancer. The emphasis is on timely, collaborative care, and on fluid communication with the various individuals and programs involved in the patient’s ongoing care; mainly, these are the patient and family, the referring oncology team, CCAC care providers and the patient’s family physician (Fig. 1). For this reason, care is provided longitudinally, rather than in a single consultation, and telephone follow-up with patients and care providers is a crucial component of care. The OPCC was established in 2002, with a single physician providing consultations and follow-up in a once-weekly clinic. At that time, clinic space and a receptionist were shared Structure of the palliative care program at the Princess Margaret Cancer Centre The Princess Margaret Cancer Centre (PM) is the largest centre in Canada for cancer care and research and is a part of the University Health Network (UHN). The UHN also includes three other academic hospitals: Toronto General Hospital (TGH), Toronto Western Hospital (TWH) and Toronto Rehabilitation Institute (TRI), all of which are affiliated with the University of Toronto. PM is located in the Toronto Central LHIN, which serves approximately 1.15 million residents. However, because PM is a tertiary cancer centre, the majority of patients attending the cancer centre reside in neighbouring Toronto LHINs or elsewhere in the province. Fig. 1 Main providers of longitudinal care for ambulatory patients with advanced cancer. OPCC Oncology Palliative Care Clinic, CCAC Community Care Access Centre Support Care Cancer (2015) 23:1073–1080 with an oncology clinic. With a yearly increase in referrals, the clinic quickly grew in size. Currently, there are 22 half-day clinics, including daily “stat” clinics for urgent referrals, to accommodate the increased demand for both scheduled and urgent same-day consultations. There are now six palliative care physicians, four palliative care nurses, one social worker and three to five residents and fellows who work in the OPCC. Physicians and nurses follow their own patients longitudinally, to ensure consistency and continuity of care. The referral process Over the past decade, there has been a progressive acceptance within PM of the philosophy of early palliative care. Currently, approximately 75 % of the 1,300 new referrals yearly to the PM palliative care program are first seen in the OPCC. Referral criteria are broad: Any patient with advanced and progressive cancer in the UHN cancer program may be referred, with no limitation on prognosis. Referrals are made by a physician (generally the patient’s primary oncologist), using a standardized form. All consult requests are screened and triaged daily by a palliative care physician prior to booking the appointment. For routine consultations, the median time from referral to consultation is approximately 2 weeks. Same-day referrals are accommodated in daily “stat” clinics. The initial palliative care consultation At the initial consultation, a palliative care physician and nurse conduct a thorough assessment and physical exam, taking 60 to 90 minutes. The philosophy of palliative care is outlined at the initial clinic visit, including the multidisciplinary approach to pain and symptom management, with an emphasis on improving quality of life and providing continuity of care. Reassurance of close collaboration and ongoing communication with the patient’s oncology team is reinforced. The palliative care nurse administers the Edmonton Symptom Assessment System (ESAS) scale [20, 21] and takes a brief history; the physician undertakes a complete chart review, medical and psychosocial history. The patient’s performance status is recorded, using both the PPS [15, 16] and the Eastern Cooperative Oncology Group (ECOG) [22] measures. Nursing and medical recommendations for treatment, education and counselling are then discussed with the patient and family. These may include changes to medications, referral to community services, and equipment and lifestyle techniques to help with symptom control. In general, the initial visit tends to focus on introducing the palliative care team and addressing physical and psychological symptoms, and discussions around advance care planning are deferred to subsequent visits. Involvement of the palliative care social worker is 1075 sought if there are specific social issues to address, such as facilitating financial and advance care planning, or providing counselling for families with young children. Referrals are made, as needed, to services such as palliative radiation oncology, psychosocial oncology and interventional radiology, amongst others (Fig. 2). Most patients referred to the clinic require some form of home assistance, which may involve wound care, personal care, supervision of medications, and symptom assessment. This is arranged through a referral to the patient’s local CCAC service. Patients are provided with a resource binder that contains contact details for the palliative care team; information on palliative care, spiritual care, community resources and advance care planning; and the Canadian Cancer Society booklet, “Living with Advanced Cancer” [23]. A complete note is dictated for the patient’s electronic medical record and a copy is sent to the patient’s oncologist and family physician. Follow-up in the OPCC After the initial consultation, patients who are still receiving chemotherapy or radiation at the PM are followed in the OPCC, generally at intervals of 1–3 months. Follow-up is carried out in the OPCC, by telephone, and at times in the oncologist’s office or chemotherapy day care centre, if this is more convenient for the patient. The PM palliative care team communicates regularly with the CCAC home care nurses. All clinic patients have access to a 24-h on-call service staffed by palliative care physicians, so that urgent symptom issues can be readily addressed. Advance care planning is carried out according to the needs and readiness of the individual patient and family. This may include discussion of resuscitation and completion of a “no CPR” form, assignment of a power of attorney for medical care, and completion of paperwork for local community palliative care units. Although most patients express a desire to die at home if possible, this paperwork is done as a “backup” for the possibility of eventual transfer to an inpatient setting. Patients work with the social worker to choose up to three community units, based on factors such as location and proximity to family or friends, the level of care required, and estimated prognosis [24]. Transition of care at the end of life Figure 3 shows typical pathways of care, culminating in endof-life care either at home or at a palliative care unit or hospice. While early palliative care involves integrated, shared care by the palliative care team with oncologists, family physicians and community services, patients eventually require transfer of care from the outpatient clinic setting to 1076 Support Care Cancer (2015) 23:1073–1080 Fig. 2 Typical referrals made from the OPCC. 1Community Care Access Centre services include nursing, personal support, physical therapy, occupational therapy and equipment such as hospital bed, walker and wheelchair. 2Medical/surgical specialists may include neurosurgery, ophthalmology and dentistry. 3Other supportive care services at the cancer centre include spiritual care, wound care, dietitian, music therapy, and occupational or physical therapy. OPCC Oncology Palliative Care Clinic, CCAC Community Care Access Centre Fig. 3 Pathways of palliative care upon referral to Oncology Palliative Care Clinic. Note that referrals to other services by Oncology Palliative Care Clinic staff are not included in this figure. Longitudinal follow-up is usually weeks to months, but may be days to years. Transfers of care to community palliative care units, hospices or home palliative care are for transitional and endof-life care; transfers to the Lederman Center may be for endof-life care or symptom control Referral to Palliave Care Clinic Early Palliave Care Community PCU/ Residenal Hospice Lederman Palliave Care Centre Home Palliave Care Transional and end of life care Support Care Cancer (2015) 23:1073–1080 either the home setting or a hospice or palliative care unit. If a patient is able to manage at home, but not well enough to come back and forth to the clinic, an enquiry is made whether the patient’s family physician is willing to make home visits and provide 24-h on-call care. If not, patients are referred to a specialized home palliative care physician providing care in their community (either shared with the family physician or as the most responsible physician). Some patients are quite ill at the initial OPCC consultation and are transferred directly to the Lederman Palliative Care Centre [18]. Waiting lists for home palliative care physicians can range from 2 to 6 weeks, or longer. The OPCC palliative care team continues to follow patients until they have been seen by the home palliative care physician, at which time there is an official sign-over of care. However, patients are often referred back to the PM palliative care service for admission to the Lederman Palliative Care Centre, either for urgent symptom control or for terminal care. The OPCC palliative care team continues to follow patients living in areas without access to a home palliative care physician, either in person or by telephone in conjunction with community-based nurse practitioners, until their death or the time of admission to an inpatient facility. Characteristics of patients referred to the OPCC Table 1 shows the demographic characteristics and performance status of the patients referred to the OPCC in 2012. Most patients were referred for general symptom management (57 %) or more specifically, for pain control (32 %). Smaller numbers were referred for advance care planning (9 %) or for terminal care (2 %). Forty-nine percent were female, the median age was 65 years (range 18–96), and the majority were from the gastrointestinal (26 %), lung (19 %) and gynaecological (12 %) disease sites. In terms of performance status, the majority of patients had an ECOG score of 1 or 2 (39 and 42 %, respectively), or a PPS score of 60–70 % (70 % of patients). Most patients were referred by medical oncology (61 %) or radiation oncology (24 %). Table 2 shows the ESAS scores of patients before their first consultation. The median ESAS Distress Score was 37 (range 0–86) with the worst symptoms out of 10 being tiredness (median 7), and a median of 5 each for pain, drowsiness, appetite, well-being and sleep. Most patients (97 %) had moderate to severe symptom ratings (i.e. rated greater than 4 on the ESAS scale) [25] and two patients were asymptomatic (i.e. rated “0” for all symptoms). Academic activities in the OPCC The OPCC is not only a clinical service but also a site for the education of physicians, nurses and other health professionals 1077 who desire training in outpatient palliative care. Residents undertaking clinical electives may come from diverse disciplines including medical, surgical or radiation oncology, internal medicine, family medicine, anaesthesia and psychiatry. Fellows enrolled in 2-year research fellowships also follow patients in the OPCC on a longitudinal basis several days a week, with supervision. The outpatient setting provides a venue for education in aspects that are less available in traditional rotations in the palliative care unit or inpatient consultation services, such as monitoring and titrating pain and symptom medications on an outpatient basis; advance care planning; and early and ongoing communication with the patient, family and other health care providers regarding the changing goals of care. The clinic is also an important venue for research, including for clinical trials, prospective, retrospective and descriptive studies, and the validation or development of measures [26–33]. Discussion There is increasing evidence for the effectiveness of introducing palliative care early in the disease trajectory for patients with advanced cancer. OPCCs are the obvious site for such care to be initiated and provided in a complementary fashion with concurrent anticancer treatment. We have described the model of care for the OPCC at our centre. This model has been shown to improve quality of life, satisfaction with care, and symptom control, both in a phase II trial and in a recent cluster-randomized controlled trial of early palliative care versus standard oncology care [3, 10]. Reported barriers to early palliative care referral include a lack of available palliative care services, and the requirement by some of these services that patients have stopped chemotherapy [34, 35]. Ongoing anticancer treatment should not preclude referral to palliative care services [5], particularly because increasing numbers of patients continue to receive treatment up until the last weeks to months of life [36]. This trend is likely to continue, given the advent of targeted treatments that are effective later in the disease trajectory [37]. A Canadian survey confirmed that a higher referral frequency was seen when palliative care services accepted patients receiving ongoing chemotherapy [34]. We encourage early referral of patients receiving chemotherapy, and our service has grown to accommodate increased and earlier referrals. There is ongoing debate about the wisdom of renaming the specialty or individual palliative care services “supportive care”. In a recent national survey of Canadian oncologists, one third stated that they would refer to palliative care earlier if it were renamed “supportive care” [34]. Similarly, a recently published randomized trial reported that the term “supportive care” was viewed more 1078 Support Care Cancer (2015) 23:1073–1080 favourably than “palliative care” by patients with advanced cancer [38]. The palliative care service at MD Anderson Cancer Center has observed earlier outpatient referrals since changing its name from palliative care to supportive care in 2007 [39], although oncologists at that centre did not think that the name change had influenced their referral practices [40]. Other services have taken the stance that education, rather than a name change, is the way forward [41]. We have taken the latter approach, in that we explicitly call our clinic the Oncology Palliative Care Clinic, but also encourage early referrals and promote the message Table 1 Characteristics of patients attending the Oncology Palliative Care Clinic (N=849) Patient characteristics Number (%), Mean [SD] Table 1 (continued) Patient characteristics Number (%), Mean [SD] 60–70 492 (70) 40–50 148 (21) 10–30 3 (<1) Data are for the year 2012. Performance status scores are those reported on the first visit SD standard deviation a Other includes palliative care physician from another University Health Network (UHN) hospital site (N=9), psychosocial oncology department (6), other UHN physician (3), family physician (2) or unknown (2) b ECOG=Eastern Cooperative Oncology Group. An ECOG score of 0=fully active at pre-disease performance, 1=ambulatory but restricted in physically strenuous activity, 2=not fully ambulatory and lying/sitting <50 % of the day, 3=capable of limited self-care and lying/sitting >50 % of the day, 4= completely disabled, unable to self-care and confined to lying/sitting [20] c Sex Male 437 (51) Female 412 (49) Age, in years 64 [13] Cancer type Gastrointestinal 217 (26) Lung 163 (19) Gynaecologic 105 (12) Palliative Performance Scale (PPS) score of 80–100=fully ambulatory, 60–70=reduced ambulation, 40–50=mainly lying/sitting and 10–30= bedbound [30] Table 2 Self-reported symptoms by patients attending the Oncology Palliative Care Clinic (N=806) Mean (SD) Median (range) Number (%) of patients rating ≥4 Genitourinary 84 (10) Head and neck 59 (7) Symptom Breast 56 (7) Pain 5.23 (3.24) 5 (0–10) 541 (67) 45 (5) Tiredness 6.28 (2.58) 7 (0–10) 685 (85) 44 (5) Nausea 2.24 (2.83) 1 (0–10) 220 (27) 26 (3) Depression 3.22 (2.97) 3 (0–10) 342 (42) 22 (3) Anxiety 3.58 (2.99) 3 (0–10) 388 (48) 18 (2) Drowsiness 4.28 (2.93) 5 (0–10) 486 (60) 10 (1) Appetite problems 5.00 (3.12) 5 (0–10) 542 (67) Hematologic Central nervous system Skin Sarcoma Unknown primary Neuroendocrine Well-being 5.19 (2.65) 5 (0–10) 593 (74) General symptom management 484 (57) Shortness of breath 3.25 (3.09) 3 (0–10) 345 (43) Pain control 276 (32) Constipation 3.30 (3.34) 3 (0–10) 340 (42) Palliative care planning 76 (9) Sleep difficulties 4.50 (3.27) 5 (0–10) Terminal care 13 (2) Primary reasons for referral Referring service Medical oncology 518 (61) Radiation oncology 201 (24) Surgical oncology 64 (7) Haematology 44 (5) Othera 22 (3) Number (%) of patients with at least one symptom ≥4 Number (%) of patients who are asymptomatic (all “0” scores) ESAS Distress Scorea ECOG performance status (N=698)b 456 (57) - 783 (97) - 2 (<1) Median (range) 37 (0–86) - Mean (SD) 38.24 (16.63) - 0 6 (1) Data are for the year 2012; symptoms are those reported on the first visit 1 273 (39) SD standard deviation, ESAS Edmonton Symptom Assessment System scale 2 292 (42) a 3 119 (17) 4 8 (1) Palliative Performance Scale (N=699)c 80–100 56 (8) ESAS Distress Score (EDS) is calculated by summing all items except constipation and sleep difficulties, multiplying by the total number of items (9), and dividing by the total number of items answered, as long as >50 % of items are answered. EDS range is 0–90, with higher numbers representing worse symptom severity. Three patients who answered <50 % of items were excluded from the EDS calculation Support Care Cancer (2015) 23:1073–1080 that palliative care is relevant throughout the illness trajectory. The palliative care model at our institution is not necessarily reflective of service availability elsewhere. Access to daily OPCCs as well as an inpatient consultation team, an acute PCU and a residential hospice facilitates referral to the palliative care program at all stages of disease and is responsive to the needs of patients, their families and referring oncologists. However, our OPCC began as a single day clinic with one physician and expanded over time, based on demand and advocacy for additional resources [19, 42]. A model of a weekly half-day clinic may be more easily reproducible for smaller or newly established programs [43]. Other centres have adopted different approaches to delivering palliative care in the ambulatory setting. For example, in a model described at the MD Anderson Cancer Center, newly referred patients are seen sequentially over 4 to 5 h by various members of the multidisciplinary team. This process culminates in a team meeting and subsequent relaying of up to 13 different recommendations to patients and caregivers [42][13]. At our centre, while a variety of disciplines is available for patient support in the OPCC, individual patient needs are assessed at each visit by a nurse and physician, and referrals are made to other palliative care specialists as required. Irrespective of the precise model of care, it is important that palliative care services are amenable to early referral, do not have prohibitive policies such as lack of acceptance of patients on chemotherapy, and are fully integrated within their parent institution as well as within the local community. Early palliative care referral, and the opportunities this affords for earlier, phased discussions about end-of-life care preferences, may help to improve symptom control, increase satisfaction with care, clarify goals of care, reduce aggressiveness of care at the end of life and help more patients to die in a place of their preference. The model we have described is appropriate for cancer centres or hospitals with large outpatient cancer programs, and illustrates that a model of early outpatient palliative care is feasible and effective. This model can be modified for smaller centres, or to include patients with non-malignant diagnoses. Acknowledgments We extend our thanks to all the interdisciplinary palliative care team members who made the functioning of this clinic possible. Special thanks to Catherine Purcell, Christine Cameron, Malka Berman and Pat Cotman for their commitment to clinical and academic excellence in developing our outpatient palliative care service. This research was funded by the Canadian Cancer Society (grant #700862; CZ), and the Ontario Ministry of Health and Long Term Care. Dr. Zimmermann is supported by the Rose Family Chair in Supportive Care, Faculty of Medicine, University of Toronto. Conflict of interest There are no financial disclosures from any of the authors. 1079 References 1. Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, Dahlin CM, Blinderman CD, Jacobsen J, Pirl WF, Billings JA, Lynch TJ (2010) Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 363(8):733– 742. doi:10.1056/NEJMoa1000678 2. Bakitas M, Lyons KD, Hegel MT, Balan S, Brokaw FC, Seville J, Hull JG, Li Z, Tosteson TD, Byock IR, Ahles TA (2009) Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the Project ENABLE II randomized controlled trial. JAMA 302(7):741–749. doi:10.1001/jama.2009.1198 3. Zimmermann C, Swami N, Krzyzanowska M, Hannon B, Leighl N, Oza A, Moore M, Rydall A, Rodin G, Tannock I, Donner A (2014) Lo C (2014) Early palliative care for patients with advanced cancer: a cluster-randomised controlled trial. Lancet 383(9930):1721–30. doi: 10.1016/S0140-6736(13)62416-2 4. Mack JW, Cronin A, Keating NL, Taback N, Huskamp HA, Malin JL, Earle CC, Weeks JC (2012) Associations between end-of-life discussion characteristics and care received near death: a prospective cohort trial. J Clin Oncol 30(35):4387–95. doi:10.1200/JCO.2012. 43.6055 5. World Health Organisation (2010) WHO definition of palliative care. http://www.who.int/cancer/palliative/definition Accessed 17 December 2013 6. Smith TJ, Temin S, Alesi ER, Abernethy AP, Balboni TA, Basch EM, Ferrell BR, Loscalzo M, Meier DE, Paice JA, Peppercorn JM, Somerfield M, Stovall E, Von Roenn JH (2012) American Society of Clinical Oncology Provisional Clinical Opinion: the integration of palliative care into standard oncology care. J Clin Oncol 30(8):880– 887. doi:10.1200/JCO.2011.38.5161 7. Foley K, Gelband H (eds) (2001) Improving palliative care for cancer: summary and recommendations. National Academies Press, Washington DC 8. Weissman DE, Meier DE (2008) Operational features for hospital palliative care programs: consensus recommendations. J Palliat Med 11(9):1189–1194. doi:10.1089/jpm.2008.0149 9. Meier DE, Beresford L (2008) Outpatient clinics are a new frontier for palliative care. J Palliat Med 11(6):823–828. doi:10.1089/jpm. 2008.9886 10. Follwell M, Burman D, Le LW, Wakimoto K, Seccareccia D, Bryson J, Rodin G, Zimmermann C (2009) Phase II study of an outpatient palliative care intervention in patients with metastatic cancer. J Clin Oncol 27(2):206–213. doi:10.1200/JCO.2008.17.7568 11. Rabow M, Kvale E, Barbour L, Cassel JB, Cohen S, Jackson V, Luhrs C, Nguyen V, Rinaldi S, Stevens D, Spragens L, Weissman D (2013) Moving upstream: a review of the evidence of the impact of outpatient palliative care. J Palliat Med 16(12):1540–9. doi:10.1089/ jpm.2013.0153 12. Hui D, Elsayem A, De la Cruz M, Berger A, Zhukovsky DS, Palla S, Evans A, Fadul N, Palmer JL, Bruera E (2010) Availability and integration of palliative care at US cancer centres. JAMA 303: 1054–61. doi:10.1001/jama.2010.258 13. Strasser F, Sweeney C, Willey J, Benisch-Tolley S, Palmer JL, Bruera E (2010) Impact of a half-day multidisciplinary symptom control and palliative care outpatient clinic in a comprehensive cancer centre on recommendations, symptom intensity, and patient satisfaction: a retrospective descriptive study. J Pain Symptom Manag 27(6):481–91 14. Smith AK, Thai JN, Bakitas MA, Meier DE, Spragens LH, Temel JS, Weissman DE, Rabow MW (2013) The diverse landscape of palliative care clinics. J Palliat Med 16(6):661–8. doi:10.1089/jpm. 2012.0469 15. Anderson F, Downing GM (1996) Palliative Performance Scale (PPS): a new tool. J Palliat Care 12(1):5–11 1080 16. Ho F, Lau F, Downing MG, Lesperance M (2008) A reliability and validity study of the Palliative Performance Scale. BMC Palliat Care 7:10. doi:10.1186/1472-684X-7-10 17. Cancer Care Ontario (2013) Palliative Care Collaborative Care Plans (CCPs) End-of-Life Stage. Cancer Care Ontario. https://www. cancercare.on.ca/common/pages/UserFile.aspx?fileId=13620 Accessed 17 December 2013 18. Bryson J, Coe G, Swami N, Murphy-Kane P, Seccareccia D, Le LW, Rodin G, Zimmermann C (2010) Administrative outcomes five years after opening an acute palliative care unit at a comprehensive cancer centre. J Palliat Med 13(5):559–65. doi:10.1089/jpm.2009.0373 19. Zimmermann C, Seccareccia D, Clarke A, Warr D, Rodin G (2006) Bringing palliative care to a Canadian cancer centre: the palliative care program at Princess Margaret Hospital. Support Care Cancer 14(10):982–987 20. Bruera E (1991) The Edmonton Symptom Assessment System (ESAS): a simple method for the assessment of palliative care patients. J Palliat Care 7:6–9 21. Chang VT, Hwang SS, Feuerman M (2000) Validation of the Edmonton Symptom Assessment Scale. Cancer 88(9):2164–2171 22. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, Carbone PP (1982) Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 5:649–55 23. Canadian Cancer Society (2010) Living with Advanced Cancer. http://www.cancer.ca/en/support-and-services/resources/ publications/?region=on Accessed 09 March 2014 24. Towns K, Dougherty E, Kevork N, Wiljer D, Seccareccia D, Rodin G, Le LW, Zimmermann C (2012) Availability of services in Ontario hospices and hospitals providing inpatient palliative care. J Palliat Med 15(5):527–34. doi:10.1089/jpm.2011.0453 25. Selby D, Cascella A, Gardiner K, Do R, Morovan V, Myers J, Chow E (2010) A single set of numerical cutpoints to define moderate and severe symptoms for the Edmonton Symptom Assessment System. J Pain Symptom Manag 39(2):241–9. doi:10.1016/j.jpainsymman. 2009.06.010 26. Cheung WY, Le LW, Zimmermann C (2009) Symptom clusters in patients with advanced cancers. Support Care Cancer 17(9):1223–30. doi:10.1007/s00520-009-0577-7 27. Lo C, Burman D, Rodin G, Zimmermann C (2009) Measuring patient satisfaction in oncology palliative care: psychometric properties of the FAMCARE-Patient scale. Qual Life Res 16(6):747–52. doi:10.1007/s11136-009-9494-y 28. Zimmermann C, Burman D, Bandukwala S, Seecareccia D, Kaya E, Bryson J, Rodin G, Lo C (2010) Nurse and physician inter-rater agreement of three performance status measures in palliative care outpatients. Support Care Cancer 18(5):609–16. doi:10.1007/ s00520-009-0700-9 29. Riechelmann R, Burman D, Rodin G, Tannock I, Zimmermann C (2010) Phase II trial of mirtazapine for cancer-related cachexia. Am J Hosp Palliat Med 27(2):106–10. doi:10.1177/1049909109345685 30. Zimmermann C, Burman D, Follwell M, Wakimoto K, Seccareccia D, Bryson J, Le L, Rodin G (2010) Predictors of symptom severity and response in patients with metastatic cancer. Am J Hosp Palliat Med 27(3):175–81. doi:10.1177/1049909109346307 Support Care Cancer (2015) 23:1073–1080 31. Ma C, Bandukwala S, Burman D, Bryson J, Seccareccia D, Banerjee S, Myers J, Rodin G, Dudgeon D, Zimmermann C (2010) Interconversion of three measures of performance status: an empirical analysis. Eur J Cancer 46(18):3175–3183 32. Jang RW, Burman D, Swami N, Kotler J, Banerjee S, Ridley J, Mak E, Bryson J, Rodin G, Le LW, Zimmermann C (2013) Impact of an oncology palliative care clinic on access to home care services. Am J Hosp Palliat Med 30(5):425–31. doi:10.1177/1049909112452469 33. Jang RW, Caraiscos V, Swami N, Banerjee S, Mak E, Kaya E, Rodin G, Bryson J, Ridley J, Le LW, Zimmermann C A simple prognostic model for patients with advanced cancer based on performance status. J Oncol Pract (in press) 34. Wentlandt K, Krzyzanowska M, Swami N, Rodin G, Le L, Zimmermann C (2012) Referral practices of oncologists to specialized palliative care. J Clin Oncol 30(35):4380–6. doi:10.1200/JCO. 2012.44.0248 35. Schenker Y, Crowley-Matoka M, Dohan D, Rabow MW, Smith CB, White DB, Chu E, Tiver GA, Einhorn S, Arnold RM (2013) Oncologist factors that influence referrals to subspecialty palliative care clinics. J Oncol Practice [epub ahead of print] 36. Earle CC, Landrum MB, Souza JM, Neville BA, Weeks JC, Ayanian JZ (2008) Aggressiveness of cancer care near the end of life: is it a quality of care issue? J Clin Oncol 26(23):3860–3866. doi:10.1200/ JCO.2007.15.8253 37. Ho TH, Barbera L, Saskin R, Lu H, Neville BA, Earle CC (2011) Trends in the aggressiveness of end-of-life cancer care in the universal health care system of Ontario, Canada. J Clin Oncol 29(12):1587– 91. doi:10.1200/JCO.2010.31.9897 38. Maciasz RM, Arnold RM, Chu E, Park SY, White DB, Vater LB, Schenker Y (2013) Does it matter what you call it? A randomized trial of language used to describe palliative care services. Support Care Cancer 21:3411–3419. doi:10.1007/s00520-013-1919-z 39. Dalal S, Palla S, Hui D, Nguyen L, Chacko R, Li Z, Fadul N, Scott C, Thornton V, Coldman B, Amin Y, Bruera E (2011) Association between a name change from palliative to supportive care and the timing of patient referrals at a comprehensive cancer centre. Oncologist 16(1):105–11. doi:10.1634/theoncologist. 2010-0161 40. Rhondali W, Burt S, Wittenberg-Lyles E, Bruera E, Dalal S (2013) Medical oncologists’ perception of palliative care programs and the impact of name change to supportive care on communication with patients during the referral process. A qualitative study. Palliat Support Care 11(5):397–404. doi:10.1017/ S1478951512000685 41. Milne D, Jefford M, Schofield P, Aranda S (2013) Appropriate, timely referral to palliative care services: a name change will not help. J Clin Oncol 31(16):2055. doi:10.1200/JCO.2012.48.4493 42. Bruera E, Sweeney C (2001) The development of palliative care at the University of Texas M.D. Anderson Cancer Centre. Support Care Cancer 9(5):330–4 43. Muir JC, Daly F, Davis MS, Weinberg R, Heintz JS, Paivanas TA, Beveridge R (2010) Integrating palliative care into the outpatient, private practice oncology setting. J Pain Symptom Manag 40(1):126– 35. doi:10.1016/j.jpainsymman.2009.12.017