Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
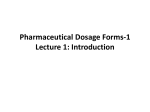
World Journal of Pharmaceutical Research Bhatt et al. World Journal of Pharmaceutical SJIFResearch Impact Factor 5.990 Volume 4, Issue 8, 871-882. Review Article ISSN 2277– 7105 ORAL SUSTAINED RELEASE DRUG DELIVERY SYSTEM: A CONCISE REVIEW Kamal Bhatt*, Divya juyal, Shivani kala and Meenakshi mehra Himalayan Institute of Pharmacy & Research, Dehradun, 248001(Uttarakhand). Article Received on 06 June 2015, Revised on 29 June 2015, Accepted on 19 July 2015 ABSTRACT Oral drug delivery system is the most preferred any convenient option as the oral route provide maximum active surface area among all drug delivery system. Pharmaceutical reinvention and research are increasingly focusing on delivery system, which enhance desirable *Correspondence for therapeutic objectives while minimizing side effect in the recent years, Author focus on the development of oral controlled release drug delivery Kamal Bhatt system has increased. The principal goal of sustained release dosage Department of Pharmaceutical Science,Himalayan form is the improvement of drug therapy assessed by the relationship between advantages and disadvantages of the use of sustained release Institute of Pharmacy & system. Sustained release dosages forms are designed to release a drug Research, Dehradun, at a predetermined rate by maintaining a constant drug level for a 248001(Uttarakhand). specific period of time with minimum side effect. KEYWORDS: Pharmaceutical Reinvention, Sustained Release Dosage and Formulation Methods, Factors Influcing, Factors Governing The Design of Sustained Release Dosage Form. INTRODUCTION The drug delivery systems that are designed to achieve a prolonged therapeutic effect by continuously releasing medication over an extended period of time after administration of single dose of drug,[1] probably the earliest work in the area of sustained drug delivery dosage forms can be traced to the 1938 patent of Israel Lipowski. This work involved coated pallets for prolonged release of drug and was presumably forerunner to the development of the coated particle approach to sustained drug delivery that introduced in the early 1950s. Ideally, a drug should arrive rapidly at the site of action (receptor) in the optimum concentration, remain for the desired time, be excluded from other sites, and be rapidly removed from the www.wjpr.net Vol 4, Issue 08, 2015 871 Bhatt et al. World Journal of Pharmaceutical Research site when indicated i.e. the basic goal of the therapy is to achieve steady state blood level that is therapeutically effective and non-toxic for an extended period of time. Generally, the time course of a dosage form (pharmacokinetics) in man is considered to be controlled by the chemical structure of the drug. Decreasing the rate of absorption and/ or changing the dosage form provide a useful adjunct. When it is feasible or desirable to modify the drug compound on a molecular level, often sought is a product that will require less frequent administration to obtain the required biologic activity time profile; for example, a tablet that has the same clinical effect when administered every twelve hours. In another instance, it may be desirable to decrease the absorption rate in order to obtain a more acceptable clinical response.[2] During the last two decades there has been remarkable increase in interest in sustained release drug delivery system. This has been due to various factor viz. the prohibitive cost of developing new drug entities, expiration of existing international patents, discovery of new polymeric materials suitable for prolonging the drug release, and the improvement in therapeutic efficiency and safety achieved by these delivery systems. Now-a-days the technology of sustained release is also applied for veterinary products. These systems also provide a slow release of drug over an extended period of time and also can provide some control, whether this be of a temporal or spatial nature, or both, of drug release in the body.[3] MERITS OF SUSTAINED RELEASE DOSAGE FORM[4, 5, 6, 7] 1. Decreased local and systemic side effects: Reduced Gastrointestinal Irritation. 2. Better drug utilization: Reduction in total amount of drug used. Minimum drug accumulation on chronic dosing. 3. Improved efficiency in treatment: Optimized therapy. Less reduction in drug activity with chronic use. 4. Improved patient compliance: Less frequent dosing Reduced night-time dosing 5. Economical to the health care providers and the Patients www.wjpr.net Vol 4, Issue 08, 2015 872 Bhatt et al. World Journal of Pharmaceutical Research DEMERITS OF CONVENTIONAL RELEASE DOSAGE FORM 1. If the drug has short half-life, it has to be administered frequently, so there are chances of Missing the dose. 2. If the drug is not taken at periodic interval, peak valley plasma concentration time profile Obtained is not steady. 3. The fluctuations of drug plasma level that occurs during conventional release may producer Overmedication. 4. Poor patient compliance PARAMETERS FOR DRUG TO BE FORMULATED IN SUSTAINED RELEASE DOSAGE FORM Physicochemical parameters for the drug selection There are some physiochemical parameters for drug selection to be formulated in sustained release dosage form which mainly includes the knowledge on the absorption mechanism of the drug from the gastro intestinal tract, its general absorbability, the drug molecular weight, solubility at different PH and apparent partition coefficient as shown in table 1.[10-12] Parameter Molecular weight/size Solubility Apparent partition coefficient Absorption mechanism Diffusion From all GI segments Preferred value < 1000 Daltons > 0.1 mg/ml for pH 1 to pH 7.8 High Diffusion General absorbability Release Pharmacokinetic parameter for drug selection The pharmacokinetic evaluation requires knowledge on a drug’s elimination half-life, total clearance, absolute bioavailability, possible first-pass effect, and the desired steady concentrations for peak and trough. Table.2.[12] Parameter Elimination half life Total clearance Elimination rate constant Apparent volume of distribution Vd Intrinsic absorption rate Therapeutic concentration Cssav Absolute bioavailability Toxic concentration www.wjpr.net Preferred value Preferably between 0.5 and 8 Should not be dose dependent Required for design The larger Vd and MEC, the larger will be the required dose size. Must be greater than release rate The lower Cssav and smaller Vd, the loss among of drug required Should be 75% or more Apart the values of MTC and MEC, safer the dosage form. Also suitable for drugs with very short half-life. Vol 4, Issue 08, 2015 873 Bhatt et al. World Journal of Pharmaceutical Research Design and Formulation of Oral Sustained Release Drug Delivery System Sustained (zero-order) drug release has been attempted to be achieved, by following classes of Sustained drug delivery system. A) Diffusion sustained system. i) Reservoir type. ii) Matrix type B) Dissolution sustained system. i) Reservoir type. ii) Matrix type C) Methods using Ion-exchange. D) Methods using osmotic pressure. E) PH independent formulations. F) Altered density formulations A) Diffusion sustained system[13, 14, 15, and 16] Basically diffusion process shows the movement of drug molecules from a region of a higher concentration to one of lower concentration. The flux of the drug J (in amount / area -time), across a membrane in the direction of decreasing concentration is given by Fick’s law. J= - D dc/dx. D = diffusion coefficient in area/ time dc /dx = change of concentration 'c' with distance 'x' (i)Reservoir type In the system, a water insoluble polymeric material encases a core of drug. Drug will partition into the membrane and exchange with the fluid surrounding the particle or tablet. Additional drug will enter the polymer, diffuse to the periphery and exchange with the surrounding media. Figure 1. Schematic representation of a reservoir diffusional device. www.wjpr.net Vol 4, Issue 08, 2015 874 Bhatt et al. World Journal of Pharmaceutical Research ii) Matrix type A solid drug is dispersed in an insoluble matrix and the rate of release of drug is dependent on the rate of drug diffusion and not on the rate of solid dissolution. Higuchi has derived the appropriate equation for drug release for this system, Fig2: Schematic representation of diffusion sustained drug release: matrix system. Q = D / T [2 A – Cs] Cst ½ Where; Q = weight in grams of drug released per unit area of surface at time t D = Diffusion coefficient of drug in the release medium = porosity of the matrix Cs = solubility of drug in release medium T= Tortuosity of the matrix A = concentration of drug in the tablet, as gm/ ml B) Dissolution sustained systems[15, 16] A drug with a slow dissolution rate is inherently sustained and for those drugs with high water solubility, one can decrease dissolution through appropriate salt or derivative formation. These systems are most commonly employed in the production of enteric coated dosage forms. To the stomach from the effects of drugs such as Aspirin, i) Reservoir type Drug is coated with a given thickness coating, which is slowly dissolved in the contents of gastrointestinal tract. The maintenance of drug levels at late times will be achieved from those with thicker coating. This is the principle of the spansule capsule. Cellulose nitrate phthalate was www.wjpr.net Vol 4, Issue 08, 2015 875 Bhatt et al. World Journal of Pharmaceutical Research Synthesized and used as an enteric coating agent for acetyl salicylic acid tablets. ii) Matrix type The more common types of dissolution sustained dosage form as shown in figure 3. It can be either a drug impregnated sphere or a drug impregnated tablet, which will be subjected to slow erosion. Two types of dissolution- sustained pulsed delivery systems: A) Single bead– type device with alternating drug and rate-controlling layer B) Beads containing drug with differing thickness of dissolving Figure 3. Two types of dissolution-controlled delivery system C) Methods using lon Exchange[14, 15, 17, 18] It is based on the formation of drug resin complex formed when a ionic solution is kept in contact with ionic resins. The drug from this complex gets exchanged in gastrointestinal tract and released with excess of Na+ and Cl- present in gastrointestinal tract. Figure 4. Ion exchange system + - - Resin - drug + X resin + - = resin- - = X- + drug – Conversely, Resin- - drug+ + Y+ www.wjpr.net Y+ + drug+ Vol 4, Issue 08, 2015 876 Bhatt et al. World Journal of Pharmaceutical Research D) Methods using osmotic pressure[15, 19, 20, 21] A semi permeable membrane is placed around a tablet, particle or drug solution that allows transport of water into the tablet with eventual pumping of drug solution out of the tablet through a small delivery aperture in tablet coating. These types of system are also known as oros, which follows the mechanism of osmotic pressure where the drug is released at constant zero order rate. The reservoir is made up of the drug and osmotic agent like mannitol or KCl, which is surrounded by semi permeable membrane. These systems generally appear in two different forms. The first contains the drug as a solid core together with electrolyte, which is dissolved by the incoming water. The electrolyte provides the high osmotic pressure difference. The second system contains the drug in solution in an impermeable membrane within the device. Figure 5. Diagrammatic representation of two types of osmotically controlled system E) pH– Independent formulations[16, 22] Most drugs are either weak acids or weak bases, the release from sustained release formulations is pH dependent. However, buffers such as salts of amino acids, citric acid, phthalic acid phosphoric acid or tartaric acid can be added to the formulation, to help to maintain a constant pH thereby rendering pH independent drug release. A buffered sustained release formulations prepared by mixing a basic or acidic drug with one or more buffering agent, granulating with appropriate pharmaceutical excipients and coating with gastrointestinal fluid permeable film forming polymer. When gastrointestinal fluid permeates through the membrane, the buffering agents adjust the fluid inside to suitable constant pH thereby rendering a constant rate of drug release. www.wjpr.net Vol 4, Issue 08, 2015 877 Bhatt et al. World Journal of Pharmaceutical Research F) Altered density formulations[23, 24, 25, 26] It is reasonable to expect that unless a delivery system remains in the vicinity of the absorption site until most, if not all of its drug contents is released, it would have limited utility. To this end, several approaches have been developed to prolong the residence time of drug delivery system in the gastrointestinal tract. Globular shells which have density lower than that of gastric fluid used as a carrier of drug for sustained release purpose. High density approach: In this approach the density of the pellets should be more than that of normal stomach content and should therefore, be at least 1-4gm/cm3. In preparing such formulation drug can be coated on a heavy core or mixed with heavy inert materials such as barium sulfate titanium dioxide iron powder and zinc oxide. Globular shells which have density lower than that of gastric fluid used as a carrier of drug for sustained release purpose. The undercoated shell is then coated by mixture of drug with polymer such as ethyl cellulose and hydroxypropyl cellulose. Thus the final product floats on the gastric fluid for a prolonged period, while slow releasing drug. FACTORS GOVERNING THE DESIGN OF SUSTAINED RELEASE DOSAGE FORM Aqueous solubility A drug of high water solubility can dissolve in water or gastrointestinal fluid readily and tends to release its dosage form in a burst and thus is absorbed quickly leading to a sharp increase in the blood drug concentration compared to less soluble drug. Diffusion or dissolution will be depend on the solubility of drug in aqueous system. So the lower limit for the solubility of drug to be formulate in release system has been reported to be 0.1mg/ml.[27,28] Half life The half-life of a drug is an index of its residence time in the body. If the drug has short half (less than two hrs.) life, the dosage form require large quantity of drug. If drug have eliminated half-life more than eight hrs. are sufficient sustained in the body. This ideally the drug for sustained release should have half-life of three to four hours.[29, 30] Therapeutic index Drug have low therapeutic index are not suitable for sustained release drug delivery. If the system fails in the body, dose dumping may occur, which leads toxicity.[31] www.wjpr.net Vol 4, Issue 08, 2015 878 Bhatt et al. World Journal of Pharmaceutical Research T.I. (therapeutic index)=TD50/ED50 Longer the value of T.I. the safer is the drug. Drug is considered to be safer if its T.I. value is greater than 10.[32] Absorption window Certain drugs when administered orally are absorbed only from a specific part of gastrointestinal tract. This part is referred to as the ‘absorption window’. These candidates are also not suitable for SRDDS.[33] Plasma concentration response relationship Generally, plasma drug concentration is more responsible for pharmacological activity rather than dose. But the drug having pharmacological activity independent of plasma concentrations, are poor candidate for oral SR drug delivery system.[34] Diffusibility In many control or sustained release system drug must diffuse through plyometric membrane or matrix. The ability of a drug to diffuse through plyometric membrane or matrix called diffusibility (diffusibility coefficient D), is a function of its molecular weight (molecular size). [35] LogD=-Svlog u + kv =-SM log M+km Where, V=molecular volume M=molecular weight Sv, Sm, kv, km=constant For drug with a molecular weight greater than 500 Dalton, the diffusion coefficient in many polymer are frequently so small that they are difficulty to quantify (i.e. less than 1012cm2/sec).thus high molecular weight drugs should be slow release in extend release using diffusion through plyometric membrane.[36] Duration of action Duration of action is the time period for which the blood levels remains above the MEC and below MSC levels. Drug acting for long duration are unsuitable candidates for formulation in to SR/CR forms.tisue binding, partition coefficient, half-life, metabolism, irreversible binding to cells are some parameters which are responsible for long duration of action of drug.[37] www.wjpr.net Vol 4, Issue 08, 2015 879 Bhatt et al. World Journal of Pharmaceutical Research Partition coefficient Partition coefficient is defined as the fraction of drug in an oil phase to that of an adjust aqueous phase. Drug that have higher partition coefficient that means very oil soluble and drug that have lower partition coefficient that means low lipid solubility.in both the cases that type of dosage form are not suitable for sustained release preparation.[38] K = C0 / C w Where, C0 = equilibrium concentration of all forms of the drug in an organic phase at equilibrium Cw = equilibrium concentration at all forms in an aqueous phase. CONCLUSION Sustained release system include any drug delivery system that achieve slow release of drug over extend time and maintain therapeutic concentration of drug. If it is unsuccessful maintain the concentration of drug but maintain the time period. It is considered prolong release system. The above discussion concludes that the matrix or coating system are helpful for formulating sustained release drug delivery system by various approaches. And discussed about the types and formulating factors that are necessary to know before the formulating drug as sustained release. REFERENCE 1. Aulton ME, Modified release per oral dosage forms, Pharmaceutics- The science of Dosage Form Design, 2nd edition, Churchill Livingstone, New York, 2005: 290-291. 2. Girish K Jani, Dhiren P Shah, Vipul D Prajapati, Vineet C Jain. Gums and Mucilage’s, AJPS, 2009; 4(5): 309-323. 3. Lee VHL, Controlled Drug Delivery Fundamentals and Applications: Introduction, Marcel Dekker, (2nded) INC, New York. 1987: 28-29 4. Chugh I, Seth N, Rana AC. Oral sustained release drug delivery system: An overview. IRJP 2012; 3(5): 57-62. 5. Bhalla N, Deep A, Goswami M. An Overview on various approaches to oral controlled drug delivery system via Gastro retentive Drug Delivery System. IRJP. 2012; 3(4): 128133. 6. Dusane RA, Gaikwad PD, Bankar VH, Pawar SP. A Review on: Sustained release technology. IJRAP. 2011; 2(6): 1701-1708. 7. Jain KK, Drug delivery system, Methods in molecular biology, Humana Press, 2008: 218. www.wjpr.net Vol 4, Issue 08, 2015 880 Bhatt et al. 8. Wani World Journal of Pharmaceutical Research MS, Controlled Release System-A Review, 2008, 6 (1),www.pharmainfo.net/review. 9. Bechgaard H, Nielson G H. Controlled release multiple units and single unit dosage. Drug Dev. & Ind. Pharm. 1978; 4(1): 53-67. 10. Chien YW, Rate controlled drug delivery system. marcel dekker ,New York revised and expanded. 2009. 11. Chauhan MJ, Patel SA, A concise review on sustained release drug delivery system and its opportunities Am.J. Pharmaceutical research. 2012; 2(2): 227-238. 12. Navin Dixit, Sheo Dutt Maurya, Bhanu P.S.Sagar.sustained release drug delivery system. Indian Journal of Research in Pharmacy and Biotechnology. 2013; 1(3): 305-310. 13. Lee VHL. Controlled Drug Delivery Fundamentals and Applications: Influence of drug properties on design, (2nded) Marcel Dekker, INC, New York.1987:16-25. 14. 6. Ho WH and Lee HLV. Controlled Drug Delivery Fundamentals and Applications: Design and fabrication of oral controlled release drug delivery system, (2nded) MarcelDekker, INC, New York. 1987: 373-420. 15. . Janos B, Klara P, Odon P, Geza RJ, Rok D, Stane S and Istvan E. Film coating as a method to enhance the preparation of tablets from dimenhydrinate crystals. Int J Pharm. 2004; 269: 393-401. 16. Patrick JS. Martin’s Physical Pharmacy and Pharmaceutical Sciences, (3rded) Varghesem Publishing House, Bombay. 1991: 512-519. 17. Kumar S, Gupta V, Malodia K. Oral Extended Release Drug Delivery System: A Promising Approach. Asian J. Pharm. Tech. 2012; 2(2): 38-43. 18. Ho WH, and Lee VHL, Influence of drug properties on design, Controlled Drug Delivery Fundamentals and Applications, 2ndedition, Marcel Dekker, New York, 1987: 16-25. 19. Devraj, Bhatt DC. Studies on enteric coated sustained timed-release tablets of Metronidazole. J. Chem. Pharm. Res. 2010; 2(2): 226-232. 20. Pogula M, Nazeer S. Extended Release Formulation. IJPT. Dec 2010; 2(4): 625- 684. 21. Modi SA, Gaikwad PD, Bankar VH, Pawar SP. Sustained Release Drug Delivery System: A Review, IJPRD. 2011; 2: 147-160. 22. Kar RK, Mohapatra S, Barik BB. Design and characterization of controlled release matrix tablets of Zidovudine. Asian J Pharm Cli Res. 2009; 2 :54-61. 23. Ratnaparkhi M.P., Gupta J.P., Sustained Release Oral Drug Delivery System – An Overview International Journal of Pharma Research & Review. 2013; 2(3): 11-21. www.wjpr.net Vol 4, Issue 08, 2015 881 Bhatt et al. World Journal of Pharmaceutical Research 24. Vyas S.P, Khar R.K.,Controlled drug delivery concept and advances, 2nd Edn Delhi:153,(2012) 25. Robinson J.R, Lee V. L, Controlled Drug Delivery:Fundamentals and Applications, 2nd Edn Published by Informa healthcare USA:373-421(2009) 26. Aulton M.E., Aulton pharmaceutics the design and manufacture of medicins.3rd Edn published by Churchill Livingstone, Elsevier: 441-482(2007). 27. Jantez GM, Robinson JR, sustained or controlled release drug delivery system. Modern pharmaceutics 3rdedition New York; marcel Dekker Inc.; 1996. 28. Popli H, Sharma SN, trends in oral sustained release formulation-1, the eastern pharmacist 1989; 32; 99-103. 29. John C and Morten C. The Science of Dosage Form Design, Aulton: Modified release peroral dosage forms, (2nded) Churchill Livingstone. 2002: 290-300. 30. Brahmana DM and Jaiswal SB.Biopharmaceutics and Pharmacokinetics, (2nd ed) Vallabh Prakashan, Delhi, 2009: 399-401. 31. Ho WH, Lee HLV. Sustained Drug Delivery Fundamentals and Applications: Design and fabrication of oral controlled release drug delivery system. 2nd ed. Marcel Dekker Inc., New York: 1987; 373-420. 32. Dusan abhijit ratila, Pawar sunil P, A review on sustained release technology. International journal of Ayurveda & pharmacy, 20112; (6): 1701-1708. 33. Kar RK, Mohapatra S, Barik BB. Design and characterization of controlled release matrix tablets of Zidovudine. Asian J Pharm Cli Res. 2009; 2: 54-6. 34. Janos B, Klara P, Odon P, Geza RJ, Rok D, Stane S, Istvan E. Film coating as a method to enhance the preparation of tablets from dimenhydrinate crystals. Int. J. Pharm. 2004; 269: 393- 401. 35. Mamidala R,Ramma V,Lingam M,gannu R,review article factors influencing The design & preformulation of oral sustained release dosage form.International Joural of pharmaceutical science & nanotechnology 2009; 2(3): 549-555. 36. Robinson JR, Vincent H, Lee L., controlled drug delivery fundamentals and application. Marcel Dekker Inc 2002: 4-60. 37. Cavillo D, mullol J, Barta Comparative pharmacology of the HI anti histamines.J Investi Allergol clin Immunol 2006: 3-12. 38. Chugh Isha, Seth Nimrata, Rana A.C., Oral sustained release drug delivery system: an overview. International journal of pharmacy. 2012; 3(5): 57-62. www.wjpr.net Vol 4, Issue 08, 2015 882