Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
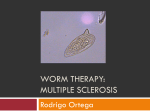
Case Report Scleredema of Buschke: A Rare Post-Streptococcal Complication S Majumder*, SK Mandal**, S Roy Chowdhury*, D Bandyopadhyay**, R Bandyopadhyay**, PP Chakraborty*** Abstract A 19-year male presented with acute onset, gradually progressive symmetric indurations involving the skin over the face, neck, shoulders and upper part of chest following an upper respiratory tract infection. Detailed history and examination did not reveal evidence of Raynauds’ phenomenon, nail changes, digital ulcers, pigmentation or any systemic involvement. Autoantibodies for systemic sclerosis were absent. Histopathology of skin biopsy documented scleredema. Antistreptolysin O (ASO) titer was elevated. We diagnosed a case of Scleredema adultorum of Buschke following a streptococcal throat infection. We report this case to highlight the importance of clinically differentiating this relatively benign, self-limiting disorder from systemic sclerosis. © INTRODUCTION S treptococcal throat infection is common. We report a case of scleredema adultorum of Buschke, a rare complication of streptococcal infection. It closely resembles systemic sclerosis. CASE REPORT A 19 year male presented in January 2006 with difficulty in opening his mouth, turning his head and raising his arms above the shoulders due to a gradually progressive stiffening of the skin over the last six weeks. The skin indurations were painless and began from the region of the neck and gradually progressed to involve the face, upper part of the trunk and the upper part of both arms. There was no involvement of the distal parts of the upper limbs or the lower extremities. There was no history suggestive of Raynaud's phenomenon or swelling of hands or feet. He specifically denied dysphagia, dyspnea, easy fatigability, weight loss or joint pains. There was no history of prolonged drug intake or toxin exposure. He was not a known diabetic and had not undergone organ transplantation. He gave a history of a febrile illness preceding the onset of his symptoms by two weeks. The fever was associated with a sore throat that lasted for about a week before it subsided with drug therapy. Examination revealed the presence of painless induration of the skin over his face (Fig. 1), neck, upper trunk and the upper part of both arms. No acral involvement (Fig. 2), digital ulcers, infarcts, plaques or pigmentation or nail changes were observed. *Post Graduate Trainee; **Assistant Professor; ***R.M.O. cum Clinical Tutor, Department of Medicine, Medical College, Kolkat. Received : 14.5.2007; Revised : 13.7.2007; Accepted : 29.8.2007 © JAPI • VOL. 55 • OCTOBER 2007 Anemia and lymphadenopathy were absent. Pulse was 84/ minute, regular and equally palpable in all four limbs. His blood pressure was 124/76 mm Hg. Systemic examination revealed no specific abnormality. Investigations revealed hemoglobin 14.5gm/dl, total white cell count 6800/cmm with normal differentials, platelet count 190 x 109/L and ESR 12mm. The fasting and postprandial plasma glucose levels were 74mg/dl and 100 mg/dl. The serum urea, creatinine, electrolytes and liver function tests were within normal limits. Urinalalysis was normal. Total serum protein was 7.2 gm/dl of which globulin was 2.9gm/dl. Ultrasonography of the abdomen and chest radiograph were within normal limits. Assays for antinuclear antibody, anticentromere antibody and anti Scl-70 were negative. Skin biopsy from involved sites revealed normal epidermal lining with short rete ridges. The mid and reticular dermis showed relatively dense eosinophilic collagen as compared with papillary dermis indicating dermal sclerosis. There was some separation of collagen fibers in reticular dermis (Fig. 3). Special stains for amyloid were negative. Histology was compatible with scleredema. Serum and urine immunofixation electrophoresis were within normal limits. The ASO titer was elevated (800IU/ml). Throat swab cultures revealed the presence of streptococcus. He was diagnosed to be a case of scleredema adultorum of Buschke following streptococcal infection. The patient was put on three-weekly intramuscular long acting penicillin therapy. He was on regular follow-up and has completely recovered over a period of four months and is leading a normal life. DISCUSSION Scleredema is a connective tissue disorder characterized by widespread induration and thickening of the skin resulting www.japi.org 737 Fig. 3 : Histopathology of skin showing dense eosinophilic collagen in the dermis. Fig. 1 : Skin induration over face. dermatological manifestation of diabetes mellitus3 and association with plasma cell dyscrasias has been reported.4 It has been reported occasionally following trauma and tubercular lymphadenitis. Streptococcal hypersensitivity injury of lymph channels, alteration of pituitary function and peripheral nerve abnormalities have all been proposed but none have been substantiated. An autoimmune pathophysiology of the disease related to streptococcal infection has also been proposed. There is no effective treatment. Most cases are self resolving within a period of six months to two years. Significant improvement has been reported recently with the use of electron beam therapy. The patient showed gradual marked improvement and has now completely recovered from his skin lesion. Therein lies the importance of distinguishing this relatively benign selflimiting condition from systemic sclerosis. Fig. 2 : Relative sparing of distal extremities. from the accumulation of collagen and proteoglycan in the dermis.1 It is characterized by stiffening and hardening of subcutaneous tissue as if infiltrated with paraffin. The onset is frequently sudden and consists of marked nonpitting symmetric induration of the skin usually affecting the posterior and lateral aspects of the neck and spreading to the face, shoulders, back, arms and thorax.2 The disease usually reaches maximum involvement in one to two weeks. The induration is of wooden-like consistency, waxy white or shiny in appearance and rather diffuse so that there is no sharp line of demarcation between involved and non-involved regions. Involvement of the neck with acral progression, sparing of hands and feet, absence of Raynaud’s phenomenon and visceral involvement permit clinical differentiation of this rare disease from systemic sclerosis. A few days to six weeks before the onset, 65% of patients develop an infection, usually of streptococcal origin.2 Most laboratory tests are within normal limits. Autoantibodies associated with both the systemic and limited forms of scleroderma are absent. Histopathology shows minimal epidermal changes with markedly thickened dermis due to collagen deposits separated by spaces of hyaluronic acid deposition. The cause of scleredema is unknown Insidious onset. Scleredema is a well recognized 738 REFERENCES 1. 2. 3. 4. 5. 6. www.japi.org Seibold JR. Scleroderma. In: Harris ED, Budd RC, Firestein GS, et al (Eds). Kelley’s Textbook of Rheumatology, 7th Edition. Philadelphia: Elsevier Saunders; 2005: 1279-1308. Fleischmajer R. Scleredema. In: Freedberg IM, Eisen AZ, Wolff K, et al (Eds). Fitzpatrick’s Dermatology in General Medicine, 5th Edition. New York: McGraw Hill; 1999: 2127-8. Ahmed I, Goldstein B. Diabetes mellitus. Clin Dermatol 2006;24:23746. Dziadzio M, Anastassiades CP, Hawkins PN, et al. From scleredema to AL amyloidosis: disease progression or coincidence? Review of the literature. Clin Rheumatol 2006;25:3-15. Alp H, Orbak Z, Aktas A. Scleredema adultorum due to streptococcal infection. Pediatr Int 2003;45:101-3. Cron RQ, Swetter SM. Scleredema revisited. A poststreptococcal complication. Clin Pediatr (Phila) 1994;33:606-10. © JAPI • VOL. 55 • OCTOBER 2007