Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
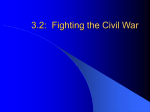
BATTLE FATIGUE, WAR NEUROSES / SHELL SHOCK Meaning #1: a mental disorder caused by stress of active warfare Synonyms: battle fatigue, combat neurosis, shell shock. Wikipedia"Shell shock" redirects here. For other uses, see Shell Shock (disambiguation).Image from World War I taken in an Australian Dressing Station near Ypres in 1917. The wounded soldier in the lower left of the photo has a dazed thousand yard stare, a frequent symptom of "shell-shock".Combat stress reaction, in the past commonly known as shell shock or battle fatigue, is a military term used to categorize a range of behaviours resulting from the stress of battle which decrease the combatant's fighting efficiency. The most common symptoms are fatigue, slower reaction times, indecision, disconnection from one's surroundings, and inability to prioritize. Combat stress reaction is generally short-term and should not be confused with acute stress disorder, post-traumatic stress disorder, or other long-term disorders attributable to combat stress although any of these may commence as a combat stress reaction. The ratio of stress casualties to battle casualties varies with the intensity of the fighting, but with intense fighting it can be as high as 1:1. In low-level conflicts it can drop to 1:10 (or less). In World War I, shell shock was considered a psychiatric illness resulting from injury to the nerves during combat. The horrors of trench warfare meant that about 10% of the fighting soldiers were killed (compared to 4.5% during World War II) and the total proportion of troops who became casualties (killed or wounded) was 56%. Whether a shell-shock sufferer was considered "wounded" or "sick" depended on the circumstances. The large proportion of World War I veterans in the European population meant that the symptoms were common to the culture, although it may not have become popularly known in the US. HISTORY: The history of Combat Stress Reactions (CSRs) has shown a remarkable variation and subvariation in the interest and knowledge of those whose tasks it has been to deal with them. Kardiner and Spiegel writing in 1947 stated: “The subject of neurotic disturbances consequent upon war has, in the past 25 years, been submitted to a good deal of capriciousness in public interest and psychiatric whims. The public does not sustain its interest, which was very great after World War I, and neither does psychiatry. Hence these conditions are not subject to continuous study...but only to periodic efforts which cannot be characterised as very diligent... Though not true in psychiatry generally, it is a deplorable fact that each investigator who undertakes to study these conditions considers it his sacred obligation to start from scratch and work at the problem as if no one had ever done anything with it before.” During the American Civil War two conditions, “soldier's heart” and “nostalgia”, were basically CSRs. Various epidemics of psychological disorders (e.g. passengers with railway spine) were recognised in the 1800s. The Russians in the Russo-Japanese War (1904-1905) were the first to specifically diagnose mental disease as a result of war stress and try to treat it. It was not until World War I that the high level of cases with "shell shock" (also referred to as traumatic war neurosis and neurasthenia) really surprised commanders and doctors. WORLD WAR I: In 1915 The British Army in France was instructed that: “Shell-shock and shell concussion cases should have the letter 'W' prefixed to the report of the casualty, if it were due to the enemy; in that case the patient would be entitled to rank as 'wounded' and to wear on his arm a 'wound stripe'. If, however, the man’s breakdown did not follow a shell explosion, it was not thought to be “due to the enemy”, and he was to [be] labeled 'Shell-shock' or 'S' (for sickness) and was not entitled to a wound stripe or a pension.” In August 1916 Charles Myers was made Consulting Psychologist to the Army. He hammered home the notion that it was necessary to create special centres near the line using treatment based on: Promptness of action. Suitable environment. Psychotherapeutic measures. He also used hypnosis with limited success. In December 1916 Gordon Holmes was put in charge of the northern, and more important, part of the western front. He had much more of the tough attitudes of the Army and suited the prevailing military mindset and so his view prevailed. By June 1917 all British cases of “Shell-shock” were evacuated to a nearby neurological centre and were labelled as NYDN “Not Yet Diagnosed Nervous”. "But, because of the Adjutant-General’s distrust of doctors, no patient could receive that specialist attention until Form AF 3436 had been sent off to the manâ_s unit and filled in by his commanding officer." This created significant delays but demonstrated that between 4-10% of Shell-shock W cases were "commotional" (due to physical causes) and the rest were "emotional". This killed off shell-shock as a valid disease and it was abolished in September 1918. During the war, 306 British soldiers were executed for cowardice, many of them victims of shell shock. On 7 November 2006 the government of the United Kingdom gave them all a posthumous conditional pardon.[3] Proximity by circumstance: Because of the delays AF 3436 was producing, medical officers started keeping their men in their units. This was perhaps the practical beginning of the concept of proximity. Col. Rogers, RMO 4/Black Watch wrote, “You must send your emotional cases down the line. But when you get these emotional cases, unless they are very bad, if you have a hold of the men and they know you and you know them (and there is a good deal more in the man knowing you than in you knowing the man), you are able to explain to him that there is really nothing wrong with him, give him a rest at the aid post if necessary and a day or two’s sleep, go up with him to the front line, and, when there, see him often, sit down beside him and talk to him about the war and look through his periscope and let the man see you are taking an interest in him.” PIE principles The PIE principles were now in place for the "not yet diagnosed nervous" (NYDN) cases: Proximity - treat the casualties close to the front and within sound of the fighting Immediacy - treat them without delay and not wait till the wounded were all dealt with Expectancy - ensure that everyone had the expectation of their return to the front after a rest and replenishment United States medical officer Thomas W. Salmon is often quoted as the originator of these PIE principles. However, his real strength came from going to Europe and learning from the Allies and then instituting the lessons. By the end of the War, Salmon had set up a complete system of units and procedures that was then the “world’s best practice”.[citation needed] After the war he maintained his efforts in educating society and the military. He was awarded the Distinguished Service Medal for his contributions. Effectiveness of PIE approach has not been confirmed by studies of CSR, and there is some evidence that it is not effective in preventing PTSD. The US services now use the more recently developed BICEPS principles: Brevity Immediacy Centrality or Contact Expectancy Proximity Simplicity BETWEEN THE WORLD WARS: The British government produced a Report of the War Office Committee of Enquiry into "Shell-Shock" which was published in 1922. Recommendations from this included: In forward areas: No soldier should be allowed to think that loss of nervous or mental control provides an honourable avenue of escape from the battlefield, and every endeavor should be made to prevent slight cases leaving the battalion or divisional area, where treatment should be confined to provision of rest and comfort for those who need it and to heartening them for return to the front line. In neurological centres: When cases are sufficiently severe to necessitate more scientific and elaborate treatment they should be sent to special Neurological Centres as near the front as possible, to be under the care of an expert in nervous disorders. No such case should, however, be so labeled on evacuation as to fix the idea of nervous breakdown in the patient’s mind. In base hospitals: When evacuation to the base hospital is necessary, cases should be treated in a separate hospital or separate sections of a hospital, and not with the ordinary sick and wounded patients. Only in exceptional circumstances should cases be sent to the United Kingdom, as, for instance, men likely to be unfit for further service of any kind with the forces in the field. This policy should be widely known throughout the Force. Forms of treatment: The establishment of an atmosphere of cure is the basis of all successful treatment, the personality of the physician is, therefore, of the greatest importance. While recognising that each individual case of war neurosis must be treated on its merits, the Committee are of opinion that good results will be obtained in the majority by the simplest forms of psycho-therapy, i.e., explanation, persuasion and suggestion, aided by such physical methods as baths, electricity and massage. Rest of mind and body is essential in all cases. The committee are of opinion that the production of hypnoidal state and deep hypnotic sleep, while beneficial as a means of conveying suggestions or eliciting forgotten experiences are useful in selected cases, but in the majority they are unnecessary and may even aggravate the symptoms for a time. They do not recommend psycho-analysis in the Freudian sense. In the state of convalescence, re-education and suitable occupation of an interesting nature are of great importance. If the patient is unfit for further military service, it is considered that every endeavour should be made to obtain for him suitable employment on his return to active life. Return to the fighting line: Soldiers should not be returned to the fighting line under the following conditions:(1) If the symptoms of neurosis are of such a character that the soldier cannot be treated overseas with a view to subsequent useful employment. (2) If the breakdown is of such severity as to necessitate a long period of rest and treatment in the United Kingdom. (3) If the disability is anxiety neurosis of a severe type. (4) If the disability is a mental breakdown or psychosis requiring treatment in a mental hospital. It is, however, considered that many of such cases could, after recovery, be usefully employed in some form of auxiliary military duty. Part of the concern was that many British veterans were receiving pensions and had long-term disabilities. By 1939, some 120,000 British ex-servicemen had received final awards for primary psychiatric disability or were still drawing pensions; about 15% of all pensioned disabilities. and another 44,000 or so. were getting pensions for “soldier’s heart” or Effort Syndrome. There is, though, much that statistics do not show, because in terms of psychiatric effects, pensioners were just the tip of a huge iceberg. War correspondent Philip Gibbs wrote: “Something was wrong. They put on civilian clothes again and looked to their mothers and wives very much like the young men who had gone to business in the peaceful days before August 1914. But they had not come back the same men. Something had altered in them. They were subject to sudden moods, and queer tempers, fits of profound depression alternating with a restless desire for pleasure. Many were easily moved to passion where they lost control of themselves, many were bitter in their speech, violent in opinion, frightening.” One British writer between the wars wrote:” There should be no excuse given for the establishment of a belief that a functional nervous disability constitutes a right to compensation. This is hard saying. It may seem cruel that those whose sufferings are real, whose illness has been brought on by enemy action and very likely in the course of patriotic service, should be treated with such apparent callousness. But there can be no doubt that in an overwhelming proportion of cases, these patients succumb to “shock” because they get something out of it. To give them this reward is not ultimately a benefit to them because it encourages the weaker tendencies in their character. The nation cannot call on its citizens for courage and sacrifice and, at the same time, state by implication that an unconscious cowardice or an unconscious dishonesty will be rewarded.” AMERICANS AND THE BRITISH IN WORLD WAR II: At the outbreak of World War II most in the United States military had forgotten the treatment lessons of World War I. Screening of applicants was initially rigorous but experience eventually showed it to not have great predictive power. December 194:1USA enters the war November 1943: A psychiatrist is added to the table of organization of each division. March 1944: This policy is finally implemented in the Mediterranean Theater. By 1943 the US Army was using the term "exhaustion" as the initial diagnosis of psychiatric cases and the general principles of military psychiatry were being used. General Patton's slapping incident was in part the spur to institute forward treatment for the Italian invasion of September 1943. The importance of unit cohesion and membership of a group as a protective factor emerged. Unlike the Americans, the lessons of WWI were firmly in British Governmental minds. It was estimated aerial bombardment would kill up to 35,000 a day but the entire Blitz killed 40,000. The expected torrent of civilian mental breakdown did not occur. The Government turned to the WWI doctors for advice on those who did have problems. The PIE principles were used generally. However, in the British Army, since most of the WWI doctors were too old for the job, young, analytically trained psychiatrists were employed. Army doctors “appeared to have no conception of breakdown in war and its treatment, though many of them had served in the 1914-1918 war.” The first Middle East Force psychiatric hospital was set up in 1942. With D-Day for the first month there was a policy of holding casualties for only 48 hours before they were sent back over the Channel. This went firmly against the expectancy principle of PIE. Germans in WWII: In a personal interview, Dr Rudolf Brickenstein stated that “... he believed that there were no important problems due to stress breakdown since it was prevented by the high quality of leadership. But, he added, that if a soldier did break down and could not continue fighting, it was a leadership problem, not one for medical personnel or psychiatrists. Breakdown (he said) usually took the form of unwillingness to fight or cowardice.” However as the war progressed there was a profound rise in stress casualties from 1% of hospitalisations in 1935 to 6% in 1942.[citation needed] Another German psychiatrist reported after the war that during the last two years, about a third of all hospitalisations at Ensen were due to war neurosis. It is probable that there was both less of a true problem and less perception of a problem. German soldiers often became victims of shell shock in the Eastern front, as the Red Army's infamous BM-13 rocket system "were often massed in very large numbers to create a shock effect on enemy forces." (text was taken from this article) Finns in WWII: The Finnish attitudes to "war neurosis" were especially tough. Psychiatrist Harry Federley, who was the head of the Military Medicine, considered shell shock as a sign of weak character and lack of moral fibre. His treatment for war neurosis was simple: the patients were to be bullied and harassed as long as they were unwilling to return to front line service. Several soldiers suffering from war neurosis were shot for cowardice in 1944[citation needed]. Earlier, during the Winter War, several Finnish machine gun operators on the Karelian Isthmus theatre became mentally unstable after repelling several unsuccessful Soviet human wave assaults on fortified Finnish positions. DEVELOPMENTS SINCE WWII: Simplicity was added to the PIE principles by the Israelis. This principle meant that treatment should be brief and supportive and could be provided by those without sophisticated training. Peacekeeping stresses Peacekeeping provides its own stresses with its emphasis on rules of engagement providing a containment of the roles for which soldiers are trained. Causes include witnessing or experiencing the following: Constant tension and threat of conflict. Threat of landmines and boobytraps. Close contact with dead people and the severely injured. Deliberate maltreatment and atrocities, possibly involving civilians. Cultural issues, e.g. male dominant attitudes towards women in different cultures. Separation and home issues. Risk of disease including HIV. Threat of exposure to toxic agents. Mission problems. Return to service. A notable case of CSR in peacekeeping operations is that of Canadian General Roméo Dallaire, commander of the UN-run operation in Rwanda, UNAMIR. Unable to intervene to prevent the ensuing Rwandan Genocide, Major-General Dallaire was forced to watch as almost a million Tutsis (a Rwandan ethnic group) were brutally killed. On return to Canada, feeling that he had not done enough to halt the genocide, and haunted by the images of dismembered victims, Dallaire contemplated suicide; in June 2000 he was found in a public park near Ottawa's Rideau Canal, drunk and overdosing from anti-depressant medication. This very public incident highlighted the impact of difficult sub-combat operations on soldiers and awoke the public's awareness to CSR (or, as it is often referred to by the public, Post-Traumatic Stress Disorder). SYMPTOMS AND SIGNS OF COMBAT STRESS REACTION: Combat stress reaction symptoms align with the symptoms also found in psychological trauma, which is highly related to Post-Traumatic Stress Disorder. Fatigue related symptoms The most common stress reactions include: The slowing of reaction time. Slowness of thought. Difficulty prioritising tasks. Difficulty initiating routine tasks. Preoccupation with minor issues and familiar tasks. Indecision and lack of concentration. Loss of initiative with fatigue. Exhaustion. Autonomic arousal Headaches. Backaches. Inability to relax. Shaking and tremors. Sweating. Nausea and vomiting. Loss of appetite. Abdominal distress. Frequency of urination. Urinary incontinence. Heart palpitations. Hyperventilation. Dizziness. Insomnia. Nightmares. Restless sleep. Excessive sleep. Excessive startle. Hyper-vigilance. Heightened sense of threat. Anxiety. Irritability. Depression. Substance abuse. Loss of adaptability. Suicidality. Disruptive behaviour. Loss of beliefs. Mistrust of others. Confusion. Extreme feeling of losing control. Battle casualty rates: The ratio of stress casualties to battle casualties varies with the intensity of the fighting. With intense fighting it can be as high as 1:1. In low-level conflicts it can drop to 1:10 (or less). Modern warfare embodies the principles of continuous operations with an expectation of higher combat stress casualties. The WWII European Army rate of stress casualties of 101:1,000 troops per annum is biased by data from the last years of the war where the rates were low. THERAPY: In the military, therapy starts with prevention by training and providing good morale and support. Simple procedures like providing adequate rest, food and shelter are important. Relaxation exercises have a role as does critical event debriefing. Once a service member has deteriorated beyond this they are usually relieved of duty and given support, dry clothes, food and rest. When appropriate they are given supportive counseling aimed at their speedy recovery. Some are prescribed psychotropic medications and simply discharged. 7 Treatment results: Figures from the 1982 Lebanon war showed that with proximal treatment 90% of CSR casualties returned to their unit, usually within 72 hours. With rearward treatment only 40% returned to their unit. In Korea 85% of US battle fatigue casualties returned to duty within three days and 10% returned to limited duties after several weeks. Although the PIE principles were used extensively in the Vietnam War the post traumatic stress disorder lifetime rate for Vietnam veterans was 30% in a 1989 US study and 21% in a 1996 Australian study. Controversy: There is significant controversy with the PIE principles. Throughout wars but notably during the Vietnam War there has been a conflict amongst doctors about sending distressed soldiers back to combat. During the Vietnam War this reached a peak with much discussion about the ethics of this process. Proponents of the PIE principles argue that it leads to a reduction of long-term disability but opponents argue that combat stress reactions lead to long-term problems such as post-traumatic stress disorder. Recent research has caused an increasing number of scientist to believe that there may be a physical rather than psychological basis for blast trauma.