Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Wernicke–Korsakoff syndrome wikipedia , lookup
Comorbidity wikipedia , lookup
Retrograde amnesia wikipedia , lookup
Conversion disorder wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
History of mental disorders wikipedia , lookup
Diagnosis of Asperger syndrome wikipedia , lookup
Transient epileptic amnesia wikipedia , lookup
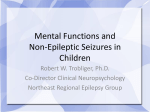
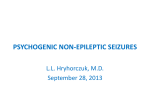
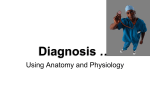
Psychogenic Nonepileptic Seizures Table of Contents Author Information 1 Introduction 2 DEFINITION 2 DIAGNOSIS 4 EPIDEMIOLOGY 4 COMORBID EPILEPSY 7 ASSOCIATED FACTORS 7 POTENTIAL NEUROBIOLOGICAL ORIGIN 8 TREATMENT 10 OUTCOMES 13 Health Care Costs 14 CASE PRESENTATION 15 CONCLUSION 16 BOARD REVIEW QUESTIONS 17 References 17 Hospital Physician Board Review Manual www.turner-white.com Author Information Epilepsy Board Review Manual Contributor: Ali A. Asadi-Pooya, MD Associate Professor, Jefferson Comprehensive Epilepsy Center, Department of Neurology, Thomas Jefferson University, Philadelphia, PA; Neurosciences Research Center, Shiraz Medical School, Shiraz University of Medical Sciences, Shiraz, Iran. Statement of Editorial Purpose The Epilepsy Board Review Manual is a study guide for trainees and practicing physicians preparing for board examinations in epilepsy. Each manual reviews a topic essential to the current management of patients with epilepsy. Note from the Publisher This publication has been developed without involvement of or review by the American Board of Psychiatry and Neurology. Publishing Staff PRESIDENT, Group PUBLISHER Bruce M. White Senior EDITOR Robert Litchkofski executive vice president Barbara T. White executive director of operations Jean M. Gaul Copyright 2015, Turner White Communications, Inc., Strafford Avenue, Suite 220, Wayne, PA 19087-3391, www.turner-white.com. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, electronic, photocopying, recording, or otherwise, without the prior written permission of Turner White Communications. The preparation and distribution of this publication are supported by sponsorship subject to written agreements that stipulate and ensure the editorial independence of Turner White Communications. Turner White Communications retains full control over the design and production of all published materials, including selection of topics and preparation of editorial content. The authors are solely responsible for substantive content. Statements expressed reflect the views of the authors and not necessarily the opinions or policies of Turner White Communications. Turner White Communications accepts no responsibility for statements made by authors and will not be liable for any errors of omission or inaccuracies. Information contained within this publication should not be used as a substitute for clinical judgment. www.turner-white.comEpilepsy Volume 3, Part 3 1 Psychogenic Nonepileptic Seizures Epilepsy Board Review Manual Psychogenic Nonepileptic Seizures Ali A. Asadi-Pooya, MD Introduction Psychogenic nonepileptic seizures (PNES) are relatively common occurrences in epilepsy centers.1,2 The International League Against Epilepsy (ILAE) has identified PNES as 1 of the 10 key neuropsychiatric conditions associated with epilepsy.3 PNES can significantly affect an individual’s quality of life and functioning, their families, the health care system, and even society. Although PNES are the most common and the most important differential diagnosis of epilepsy, they are not well characterized and therefore are often not well diagnosed and treated. Diagnostic delay, mistreatment of PNES as epilepsy, and poor communication between physicians and patients are common in practice.3 Several different terms have been used to describe PNES in the literature.4 This article reviews the current literature about the definition, recruitment criteria, occurrence, clinical characteristics, treatment, and prognosis of PNES. It concludes with a case presentation that highlights key points in the diagnosis and management of PNES. DEFINITION PNES consist of paroxysmal changes in responsiveness, movements, or behavior that superficially resemble epileptic seizures, but lack a neurobiological origin similar to epileptic seizures and are not associated with electrophysiological epileptic changes.5–7 The terms used to describe this condi2 Hospital Physician Board Review Manual tion reflect the prevailing etiological assumptions of their times; hysterical seizures, conversion seizures or disorder, functional seizures, functional neurological symptom disorder, pseudoseizures, psychogenic seizures, nonepileptic attacks or episodes, and finally, psychogenic nonepileptic seizures (PNES) are some of the terms used to describe this disorder.4 Interestingly, PNES is a condition made unique by having largely been defined in terms of what it is not, rather than what it is. Even the newest criteria in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), for conversion disorder with attacks or seizures, in which the emphasis is “incompatibility” with a known neurological disorder, does little to help define PNES clearly and explicitly.8 Based on DSM-5 criteria, PNES is a conversion disorder, which falls under the diagnostic category of somatic symptom disorders (Table 1).8 The differential diagnoses of PNES include epilepsy and movement disorders, among other possibilities (eg, syncope). Epilepsy and PNES have a variety of differing symptoms and signs. For example, asynchronous limb movements, out-ofphase clonic activity, wax and wane movements (intermittent shaking movements with episodes of inactivity), side-to-side head movements, pelvic movements (especially forward thrusting), dystonic posturing (including opisthotonos), eyes closed during the event and resisted eyelid opening, and nonstereotypical seizure patterns are more often seen with PNES; however, none of them is pathognomonic for PNES. On the other hand, auras, urine www.turner-white.com Psychogenic Nonepileptic Seizures Table 1. Diagnostic Criteria (DSM-5) for Psychogenic Nonepileptic Seizures (PNES) The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) categorizes PNES as a conversion disorder, which is included in the diagnostic category of somatic symptom disorders. According to the DSM-5 classification, neurological symptoms that are determined to be incompatible with neurological pathophysiology, after appropriate neurological assessment, can be considered conversion disorder, factitious disorder, or malingering. DSM-5 criteria for conversion disorder: 1 or more symptoms of altered voluntary motor or sensory function. • Clinical findings provide evidence of incompatibility between the symptom and recognized neurological or medical conditions. • The symptom or deficit is not better explained by another medical or mental disorder. • The symptom or deficit causes clinically significant distress or impairment in social, occupational, or other important areas of functioning or warrants medical evaluation. PNES falls under the symptom subtype of “with attacks or seizures.” Adapted from Benbadis SR. Psychogenic nonepileptic seizures. Medscape. http://emedicine.medscape.com/article/1184694-overview. incontinence, nocturnal seizures, and ictal injury are often associated with epileptic seizures; however, none of them is pathognomonic for epilepsy. Thus, sometimes clinical differentiation of PNES from epilepsy proves to be difficult.9–11 Prolonged videoelectroencephalography (video-EEG) monitoring with ictal recording is considered the optimal test for the diagnosis of PNES and a definitive diagnosis is made when typical seizures lack accompanying electroencephalography (EEG) abnormalities. However, there are patients with epilepsy (eg, frontal lobe epilepsy) and abnormal movements during their epileptic seizures with no visible change in their scalp EEG.9 Frontal lobe seizures are challenging to diagnose and can be mistaken for nonepileptic events. Scalp EEG recording is sometimes helpful in localization but can be misleading in frontal lobe epilepsy. Studies in patients with refractory frontal lobe epilepsy have shown few patients have localized interictal epileptiform discharges. Unlike temporal lobe complex partial seizures, the scalp ictal recording may not be associated with a clear EEG correlate in 30% of patients.9 The term psychogenic movement disorders (PMD) has been applied to disorders that manifest with physical symptoms, specifically abnormal movements, which cannot be attributed to any known underlying neurological disorders.12 However, the distinction between PNES and PMD is not always easy. One retrospective study of comparison of PMD and PNES revealed more similarities than differences between these 2 conditions.13 In another study, despite the different physical manifestations of the 2 conditions, the authors found no differences between the psychiatric profiles, health-related quality of life, or self-efficacy for self-management of disease among patients with PNES and PMD.14 In another study, the authors observed that patients with motor conversion disorder had IQ levels in the average range and intact general cognitive functioning, suggesting possible mechanistic differences from patients with PNES.15 Because of the challenges of characterizing PNES, misdiagnosis is common, and symptoms may be attributed to more than one condition in a single patient, or different physicians may offer different diagnoses to the same patient. In a previous study of 350 adult patients with uncontrolled seizures who were taking antiepileptic drugs (AEDs), 9% were proved to have PNES.10 In another similar www.turner-white.comEpilepsy Volume 3, Part 3 3 Psychogenic Nonepileptic Seizures Table 2. Overview of Proposed Diagnostic Levels of Certainty for Psychogenic Nonepileptic Seizures Diagnostic Level History Witnessed Event Electroencephalography Possible + By witness or self-report/description Probable + Clinically established + By clinician, who reviewed video recording or observed event in person, showing semiology typical of PNES By clinician experienced in diagnosis of seizure disorders (on video or in person), showing semiology typical of PNES while not on EEG No epileptiform activity in routine or sleep-deprived interictal EEG No epileptiform activity in routine or sleep-deprived interictal EEG Documented + By clinician experienced in diagnosis of seizure disorders, showing semiology typical of PNES while on video-EEG No epileptiform activity in routine or ambulatory ictal EEG during a typical ictus/event in which the semiology would make ictal epileptiform EEG activity expectable during equivalent epileptic seizures No epileptiform activity immediately before, during, or after ictus captured on ictal video-EEG with typical PNES semiology EEG = electroencephalography; PNES = psychogenic nonepileptic seizures; + = history characteristics consistent with PNES. Adapted with permission from LaFrance WC, Baker GA, Duncan R, et al. Minimum requirements for the diagnosis of psychogenic nonepileptic seizures: A staged approach. A report from the International League Against Epilepsy Nonepileptic Seizures Task Force. Epilepsia 2013;54:2005–18. study in 198 children, this figure was 1.5%.11 As a result, patients with PNES are at risk of iatrogenic harm, as they are more likely to receive unnecessary medications (eg, AEDs), emergency treatments, and even hospital admissions. diagnosis The diagnosis of PNES may be based on different combinations of data. The combination of patient history, witness reports, clinician observations, and ictal and interictal EEG and ictal video is used for diagnostic determination. Four categories of diagnostic levels of certainty for PNES have been suggested based on common scenarios and the combination of data (Table 2).16 In a systematic review of the sensitivity and specificity of procedures for the differential diagnosis of epileptic from nonepileptic seizures, multiple methods including seizure induction procedures, Minnesota Multiphasic Personality Inventory, prolactin levels, and ictal and postictal symptoms were reviewed; 4 Hospital Physician Board Review Manual no procedure emerged with both high sensitivity and specificity and adequately replicated findings.17 However, this review suggested that video-EEG monitoring has as yet no reliable equivalent among the range of procedures and observations which have been investigated. The range of symptoms presented in PNES suggests that a multi-method approach may be required.17 EPIDEMIOLOGY Occurrence PNES are relatively common. It has been reported that from 5% to 10% of outpatients in epilepsy clinics and 20% to 40% of inpatients in epilepsy monitoring units have PNES.1,2,18 In a populationbased prospective study from Scotland, the authors identified first presentations of PNES from a population of 367,566 persons over 3 years. PNES were diagnosed in 68 people, in 54 of whom the diagnosis was confirmed by video-EEG recording, indicating an incidence of 4.9 per 100,000 per www.turner-white.com Psychogenic Nonepileptic Seizures 40 Mean = 22.9011 Standard deviation = 10.13033 N = 188 Number of patients 30 20 10 0 0 20 40 60 Age of onset (years) Figure 1. Age at onset in patients with psychogenic nonepileptic seizures. (Adapted with permission from Asadi-Pooya AA, Emami M. Juvenile and adult-onset psychogenic non-epileptic seizures. Clin Neurol Neurosurg 2013;115:1697–1700.) year.19 In another study, the incidence of PNES was estimated to be 1.4 per 100,000 per year in Iceland.20 In a retrospective study of patients referred to a specialist center, the incidence of PNES in Hamilton County, Ohio, between 1995 and 1998 was determined. The mean incidence of PNES was 3.03 per 100,000 per year.21 Prevalence data of PNES is scarce, with just 1 study in the literature focusing on this question. The authors of the study tried to provide an estimate based on a calculation using the following data as the basis of their calculation: a prevalence of epilepsy of 0.5% to 1%; a proportion of intracta- ble epilepsy of 20% to 30%; a percentage of these referred to epilepsy centers of 20% to 50%; and a percentage of patients referred to epilepsy centers that have PNES of 10% to 20%. They concluded that the prevalence of PNES is somewhere between 1 per 50,000 and 1 per 3000, or 2 to 33 per 100,000, making it a significant psychoneurological condition.22 Age at onset PNES tend to begin in adolescence and young adulthood (Figure 1), although the seizures can begin at any age.23–33 There are reports about www.turner-white.comEpilepsy Volume 3, Part 3 5 Psychogenic Nonepileptic Seizures Table 3. Demographic Characteristics of Patients with Psychogenic Nonepileptic Seizures North America (New Hampshire, USA) North America (Arizona, USA) South America (Brazil) South America (Argentine) Europe (Scotland) Europe (UK) Asia (Iran) Asia (India) Africa (South Africa) Australia Mean Age at Onset (yr) Mean Time to Confirmed Diagnosis (yr) 33.4 NS 27.85 NS 30.9 31.55 23.2 21.8 NS 32.7 6.51 NS 7.89 11.18 0.6 7.1 5.5 7.4 NS 5.6 Female/Male (ratio) 59/27 (2.18) 142/42 (3.38) 78/24 (3.25) 27/8 (3.37) 44/10 (4.4) 117/43 (2.72) 141/70 (2.01) 44/38 (1.15) 17/5 (3.4) 156/65 (2.4) NS = not specified. Adapted with permission from Asadi-Pooya AA, Sperling MR. Epidemiology of psychogenic nonepileptic seizures. Epilepsy Behav 2015;46:60–5. PNES in young children (as young as 5 years of age),23,24 and some studies reported PNES in the elderly (even above 70 years of age).23,25,32 Age at onset in most patients appears to be in young adulthood, but there is often a significant delay to have a confirmed diagnosis, and patients often receive unnecessary treatments (eg, AEDs) for years before a correct diagnosis is made (Table 3).18 In one study, the authors dichotomized the patients into 2 groups: those with age at onset below 18 years (juvenile), and those with age at onset at 18 to 55 years (adult-onset). Age at onset of PNES did not correlate with clinical manifestations, although factors potentially predisposing to PNES were quite different in patients with juvenile-onset compared to those with adult-onset PNES. History of being abused, academic failure, epilepsy or family history of epilepsy were more frequently observed in juvenile PNES, while medical comorbidities were more frequent among patients with adult-onset PNES.23 In another study, the authors compared patients with onset of PNES after age 6 Hospital Physician Board Review Manual 55 years (n = 26) to those with onset of the disease at earlier ages (n = 241). They observed that patients with late-onset PNES were more likely to be male and to have severe physical health problems, while they were less likely to report antecedent sexual abuse.25 Gender There is a predominance of female gender among patients with PNES.33–37 The female:male ratio in one study from China was reported to be 1,35 but studies from 5 continents generally note PNES to be far more common in females (Table 3). Lesser examined the sex distribution in 21 studies and found descriptions of 734 women and 250 men who had PNES (female:male ratio = 2.94).36 However, most studies are not specifically designed to determine the demographic characteristics of patients with PNES. PNES are not only less common in men, but also more challenging to recognize in the clinic, and even when suspected, more difficult to confirm with video-EEG monitoring.34 However, no specific www.turner-white.com Psychogenic Nonepileptic Seizures or consistent difference in the underlying psychopathology between men and women with PNES has been reported. In one study (129 women and 59 men), there were no significant demographic differences between women and men with PNES. Likewise, seizure characteristics and semiology were similar among both genders.37 Another study also tried to determine if gender-specific differences exist in PNES predictors and PNES semiology. The authors investigated 59 women and 27 men, retrospectively. They found significantly lower rates of reported physical and sexual abuse, lower rates of previous psychiatric diagnoses, and lower rates of chronic pain in male patients. However, they found no difference in PNES semiology between men and women. They concluded that distinct risk factor criteria but similar semiologic criteria should be used for the diagnosis of probable PNES in the outpatient clinic in men and women.33 Comorbid epilepsy The proportion of patients with PNES who also have epilepsy has been reported to vary from 5% to 50%.18,22,26,38–41 Criteria for concomitant diagnosis of epilepsy have not been consistent in literature reports. Having interictal spikes, as most studies defined their epilepsy cases, does not necessarily mean that epilepsy is also present. Interictal epileptiform abnormalities have been reported in nonepileptic conditions42 and even in normal people.43 The key step in making a correct diagnosis of epilepsy is having a standardized approach, particularly with regard to taking a detailed clinical history. If the diagnosis of epilepsy (vs PNES) cannot be established by taking history alone, one should obtain further testing and diagnostic information (eg, prolonged video-EEG monitoring). In a study of 176 patients with PNES, 103 patients had PNES, without any evidence for epilepsy or family history of epilepsy; 19 patients had PNES and concomitant epilepsy, but they did not have family history of epilepsy; 54 patients had PNES and family history of epilepsy, but they did not have concomitant epilepsy. Demographic and clinical characteristics and associated factors of patients with PNES with co-existing epilepsy were similar to those in patients with PNES without co-existing epilepsy.38 It has been speculated that epilepsy may contribute to the risk for developing PNES not only through biologic mechanisms, but also because the experience or observation of epileptic seizures may provide an opportunity for model learning.44 Associated factors PNES occur in a heterogeneous patient population. No single mechanism or contributing factor has been identified that is necessary and sufficient to explain PNES in all patients.44 The most commonly reported PNES associated factors include sexual abuse, physical abuse or neglect, traumatic brain injury, medical comorbidities, and psychiatric comorbidities.2,45–52 The relationship between childhood sexual abuse and PNES has received particular attention in the literature. In a study comparing childhood abuse in patients who had PNES (71 patients) and those who had epilepsy (140 patients), significantly higher rates of both sexual (24.0% versus 7.1%) and physical (15.5% versus 2.9%) abuse were found in those who had PNES (P < 0.001).52 In a recent study comparing patients with PNES only (324 patients) with those who had epilepsy only (281 patients), history of abuse (physical or sexual) was more frequent among those with PNES (odds ratio 3.35, 95% confidence interval 1.23 to 9.10; P = 0.018).53 However, there www.turner-white.comEpilepsy Volume 3, Part 3 7 Psychogenic Nonepileptic Seizures are discrepancies and inconsistencies among studies with regard to the interaction between childhood sexual or physical abuse and PNES depending on the study and the design. In one study from Iran, the authors observed that history of childhood abuse (12.8%), physical abuse (11.8%), and sexual abuse (8.1%) were not as common in patients with PNES, compared to Western patients.2,52 The wide variety of methods used for assessment of abuse (sexual and physical) and lack of control populations in most of the published studies make it difficult to establish a cause and effect relationship between PNES and abuse. Another commonly reported PNES-associated factor is traumatic brain injury (TBI). In a study of 92 patients with PNES, 41 (44.6%) had a history of TBI. Patients with TBI had more mood disorder diagnoses, were more likely to receive disability, and had lower global functioning than non-TBI patients with PNES, after adjusting for age and sex. Patients with TBI and PNES had significantly increased odds for having major depression, behavioral impulsivity, posttraumatic stress disorder diagnosis, and a trauma/abuse history. The authors concluded that TBI is a significant risk factor in patients with PNES, being associated with increased psychiatric diagnostic comorbidity, symptom severity, poorer functioning, and increased disability.47 Clinical experience suggests that PNES commonly start in association with or during a period of exacerbation of another mental disorder. A lifetime history of other somatoform or dissociative disorders is found in more than 50% of patients who have PNES. Anxiety or psychotic and bipolar disorders are less common but are found more frequently in patients who have PNES than in the general population. Many patients with PNES have features of posttraumatic stress disorder (PTSD).44 I should emphasize that an agreed upon distinc8 Hospital Physician Board Review Manual tion between PNES associated factors and comorbidities is not apparent in the literature and a complete discussion of psychiatric comorbidities (eg, depression, anxiety) is too broad to be covered in this review. Often and in most patients with PNES, several potential interacting factors may be identified.44 Reuber in his review concluded that predisposing factors (eg, abuse, neglect) increase vulnerability to the development of PNES. Precipitating factors may occur over days to months before the onset of seizures and seem to cause PNES to start, but these are far from universal. Factors that have been described as precipitating PNES include rape, injury, death of or separation from family members or friends, job loss, accidents, giving birth, surgical procedures, natural disasters (eg, earthquakes), relationship difficulties, and legal action.44 In older people, medical comorbidity is a common identifiable precipitant.23,37,44 Finally, perpetuating factors (eg, isolation, anger, anxiety, depression, misdiagnosis, mistreatment) make it harder for patients to regain control of seizures or aggravate the problem once seizures have started (Figure 2). Even if one factor seems to play a predominant role in a particular patient, other factors are likely to have contributed and should not be ignored.44 Potential neurobiological origin Organic brain dysfunction is associated with PNES. The neurobiology of PNES is still poorly understood. Obviously, PNES lack a neurobiological origin similar to epileptic seizures, but emerging evidences suggest that there is a neurobiological basis for these events.54 In one study of functional connectivity networks from resting-state functional magnetic resonance imaging signal correlations and structural connectivity networks from diffusion www.turner-white.com Psychogenic Nonepileptic Seizures Figure 2. Etiology of psychogenic nonepileptic seizures (PNES): a multifactorial model. (Adapted with permission from Reuber M. The etiology of psychogenic non-epileptic seizures: Toward a biopsychosocial model. Neurol Clin 2009;27:909–24.) tensor imaging tractography in 17 PNES patients and 20 healthy controls,55 it was observed that patients with PNES exhibited altered functional and structural networks. This study showed that the coupling strength of functional-structural connectivity was decreased and exhibited high sensitivity and specificity to differentiate patients with PNES from healthy controls.55 In another study of functional connectivity density mapping, the authors found that patients with PNES had abnormal functional connectivity density regions mainly in the frontal cortex, sensorimotor cortex, cingulate gyrus, insula, and occipital cortex. Seed-voxel correlation analyses also showed disrupted functional connectivity between these regions.56 In a recent study, 18FDG-PET was performed in 16 patients with PNES and 16 healthy controls. A voxel-byvoxel intergroup analysis was performed to look for significant differences in interictal resting state cerebral metabolism. In addition, metabolic connectivity was studied using voxel-wise inter-regional correlation analysis. In comparison to healthy participants, patients with PNES exhibited significant PET hypometabolism within right inferior parietal and central regions and within bilateral anterior cingulate cortices. The authors concluded that regions with hypometabolism might relate to 2 pathophysiological mechanisms that may be involved in PNES: emotional dysregulation (anterior cingulate hypometabolism) and dysfunctional processes underlying the consciousness of the self and the environment (right parietal hypometabolism).57 Models explaining the pathogenic mechanisms leading to PNES are limited. A hypothetical pathophysiological mechanism was proposed in 2011 by Baslet.51 This pathophysiological model suggested an alteration in the influence and connection of brain areas involved in emotion processing onto other brain areas responsible for sensorimotor and cognitive processes (Figure 358). PNES were conceptualized as brief episodes facilitated by an unstable cognitive-emotional-attention system.51 www.turner-white.comEpilepsy Volume 3, Part 3 9 Psychogenic Nonepileptic Seizures Figure 3. Schematic overview of the circuitry involved in cognitive-emotional-executive control. There is significantly higher functional connectivity strengths between regions involved in emotion (eg, insula) and motor planning (eg, precentral sulcus) in patients with psychogenic nonepileptic seizures (PNES). It appears that healthy controls can control their motor functions without strong influence of emotions, whereas in patients with PNES emotions can bypass executive control and cause involuntary movement. (Adapted with permission from van der Kruijs SJ, Bodde NM, Vaessen MJ, et al. Functional connectivity of dissociation in patients with psychogenic non-epileptic seizures. J Neurol Neurosurg Psychiatry 2012;83:239–47.) This model is very well supported by the recent findings discussed above. PNES could be the result of neurobiological dysfunctions at specific brain networks. Treatment Many professionals diagnosing patients with PNES refer them to mental health professionals for treatment.59 At the same time, continued involvement of the neurologist who established the diagnosis is desirable to allow a safe taper of AEDs, prevent inappropriate treatment, evaluate the development of any new neurological symptoms, and treat any comorbid neurological condition.60 Once 10 Hospital Physician Board Review Manual patients enter mental health treatment, no guidelines exist on the type or duration of treatment that will help them achieve symptom improvement and functional recovery.61 PNES comprise a heterogeneous population,44 and ideally different treatment protocols should exist for different PNES subgroups. In the absence of such guidelines, treatment of PNES could be conceptualized in 4 phases (Figure 4).61 The initial phase of treatment is diagnosis delivery. In most cases the diagnosis is likely to be communicated by a neurologist. No research has been undertaken to establish whether it is effective to involve the patients’ family members in the discussion of the diagnosis. However, having family www.turner-white.com Psychogenic Nonepileptic Seizures Symptom Diagnosis Delivery Engagement Acute Treatment Long-term Followup Figure 4. Treatment phases in psychogenic nonepileptic seizures (PNES). (Adapted with permission from Baslet G, Dworetzky B, Perez DL, Oser M. Treatment of psychogenic nonepileptic seizures: updated review and findings from a mindfulness-based intervention case series. Clin EEG Neurosci 2015;46:54–64.) members present during the presentation may facilitate understanding of the condition.62 There is increasing evidence that the process of communicating the diagnosis is a very important and potentially effective therapeutic step in the management pathway of patients with PNES 62 (See Prognosis). Table 3 describes the strategies used for the communication of the diagnosis of PNES by some experts in the field. The second phase of treatment is engagement. Engagement is a pivotal phase of treatment in PNES. While some patients may be ready to become active participants in mental health treatment immediately after the diagnosis is delivered to them, other patients will take longer to accept such referrals or to meaningfully engage in the treatment process. Use of clinician skills to enhance behavioral change in the patients may have the potential to help them move through their treatment course. Ideally, by the end of this phase, patients understand their diagnosis, do not seek further diagnostic evaluations elsewhere, establish contact with a mental health provider, and start to actively participate in treatment.61 The third phase of treatment involves an acute intervention. Formal psychiatric assessment should be arranged and performed. Predisposing, precipitating, and perpetuating factors should be investigated. Individualized psychotherapeutic and psychopharmacological treatment plans should be formulated. This phase has a primary goal of reduction of event frequency. But, improvement in secondary measures such as severity of psychiatric comorbidities, quality of life, functional recovery, and medical resource utilization is also desired.61 In one pilot randomized clinical trial at 3 academic medical centers with mental health clinicians trained to administer psychotherapy or psychopharmacology to outpatients with PNES, 34 patients were randomized in a blocked schedule among 3 sites to 1 of 4 treatment arms and were followed up for 16 weeks.63 The treatment arms included medication (flexible-dose sertraline) only, cognitive behavioral therapy informed www.turner-white.comEpilepsy Volume 3, Part 3 11 Psychogenic Nonepileptic Seizures Table 3. Strategies Used for the Communication of the Diagnosis of Psychogenic Nonepileptic Seizures The Expert The Communication Strategy Shen Good news: these seizures are not caused by epilepsy, explain video-EEG findings. Bad news: we do not know the precise cause of the seizures, but they are nonepileptic—AEDs do not work. AEDs may cause serious side effects. “We may never know what these seizures are but can work together on the problems.” In most cases seizures are eventually related to upsetting emotions of which patients are unaware. This may be best addressed by a psychiatrist, a psychologist or a counselor. You are not crazy, the seizures occur at a subconscious level. Counseling may not control seizures immediately, but seizures can improve as treatment progresses. Neurologic follow-up will continue. A history of sexual abuse is discovered in many cases. The seizures may stop spontaneously. Although they are subconscious, a conscious effort can sometimes stop them. More seizures may occur before complete control is achieved. Cover reasons for concluding they do not have epilepsy. Relay what they do have. Emphasize they are not suspected of “putting on” the events. They are not “mad”; the problem is common, and seizures are disabling. Events are stress related, but stresses may be difficult to identify. Triggering “stresses” may not be immediately apparent. Explain relevance of etiologic factors in their case. Discuss maintaining factors. Worry about seizures may make them worse/more frequent. Avoidant behavior may make seizures worse. May improve after correct diagnosis. Caution that AED withdrawal should be gradual. Describe psychological treatment. Include patients' caregivers when delivering this explanation. Explain how video-EEG works and how it has helped with the diagnosis. Seizures are emotional/psychological, due to past/present issues, not a medical condition. List possible predisposing factors as “specimen causes” not directly linked to the patient. Seizures are not under conscious control, but patients can learn to control them with help from a therapist. Patients may have anxiety or low mood, but are otherwise not mentally ill or “mad.” AED treatment does not work, psychological treatment can work, no other treatment is available. Describe psychological intervention. Ask whether patients want psychological intervention. Explain that the symptoms are genuine. Real events; can be frightening or disabling. Label. Give a name for the condition. Give alternative names they may hear. Reassure that this is a common and recognized condition. Cause and maintaining factors: not epilepsy, predisposing factors difficult to identify, precipitating factors can be related to stress/emotions, perpetuating factors. Provide a model for the events (eg, brain becomes overloaded and shuts down). Treatment. AEDs are not effective. Evidence that psychological treatment is effective. Talk about referral to a treatment specialist. Expectations. Can resolve, can expect improvement. Mellers Duncan Hall-Patch AED = antiepileptic drug; EEG = encephalography. Adapted with permission from LaFrance WC Jr, Reuber M, Goldstein LH. Management of psychogenic nonepileptic seizures. Epilepsia 2013;54 Suppl 1:53–67. 12 Hospital Physician Board Review Manual www.turner-white.com Psychogenic Nonepileptic Seizures psychotherapy (CBT-ip) only, CBT-ip with medication (sertraline), or treatment as usual. The CBT-ip arm showed a 51.4% seizure reduction (P = 0.01) and significant improvement from baseline in secondary measures including depression, anxiety, quality of life, and global functioning (P < 0.001). The combined arm (CBT-ip with sertraline) showed a 59.3% seizure reduction (P = 0.008) and significant improvements in some secondary measures, including global functioning (P = 0.007). The sertraline-only arm did not show a reduction in seizures (P = 0.08). The treatmentas-usual group showed no significant seizure reduction or improvement in secondary outcome measures (P = 0.19). Participants in the CBT-ip condition reported significantly fewer visits to the emergency department during the trial relative to baseline.63 Other potential psychotherapeutic interventions include psychodynamic therapy and group therapies (eg, family therapy if family system dysfunction is present).62 The pharmacologic treatment plan of patients should include early tapering and discontinuation of AEDs, unless a specific AED has a documented beneficial psychopharmacologic effect in an individual patient (eg, lamotrigine for depression or valproate for bipolar disorder). In people with comorbid epileptic seizures, reduce high doses of AEDs or polytherapy if possible. Finally, use psychopharmacologic agents (eg, sertraline, venlafaxine) to treat comorbid mood, anxiety, or psychotic disorders, and possibly to treat somatoform symptoms directly.62 The final phase of treatment is composed of long-term interventions. This is particularly relevant for the subgroup of PNES patients who remain symptomatic after the acute intervention phase and who will need ongoing care to optimize the use of resources and functional recovery. This may include long-term psychotherapy, case manage- ment, and ongoing psychotropic management of psychiatric comorbidities among other individualized interventions.61,62 OUTCOMES Prognosis Definitive diagnosis of PNES can lead to appropriate therapy and even cessation of the events.64 In one study, seizure frequency during inpatient video-EEG monitoring was examined before and after the diagnosis of PNES being presented to 22 patients. A control group of 10 patients with epilepsy was also followed from pre- to post-diagnosis. The number of nonepileptic seizures (in patients with PNES) or epileptic seizures (in those with epilepsy) within the 24-hour period prior to diagnosis was compared with the number of events that occurred within the 24-hour period after presentation of the diagnosis. Their findings indicated that patients with PNES had a significant decrease in the frequency of events after diagnosis, while those with epilepsy showed no change in event frequency after diagnosis. Eighteen of 22 patients with PNES had no further events during an acute follow-up period.64 However, in a previous review the authors concluded that communicating to the patient that the seizures are not epileptic may stop PNES in short-term, but does little to improve associated psychological morbidity, distress, or health-related quality of life. Without dedicated further treatments, PNES are likely to restart in the majority of patients.62 Unfortunately, longer-term studies suggest that many patients with PNES will continue to experience seizures despite neurological and psychotherapeutic care.65 Clinical and personality factors should be used to provide an individualized prognosis in patients with PNES. In one study, 164 adult patients with PNES were investigated a mean www.turner-white.comEpilepsy Volume 3, Part 3 13 Psychogenic Nonepileptic Seizures of 11.9 years after manifestation and 4.1 years after diagnosis of PNES. The responses showed that 71.2% of patients continued to have seizures and 56.4% were dependent on social security. Outcome was better in patients with greater educational attainments, younger onset and diagnosis, attacks with less dramatic features, fewer additional somatoform complaints, and lower dissociation scores.65 In a systematic review published in 2011, the authors concluded that the prognosis of PNES in adults is poor. From their reviewed data, fewer than 4 in 10 newly diagnosed adults could be expected to become seizure-free within 5 years after diagnosis. In children the figure of patients achieving seizure remission appeared to be around 70%, which indicates a more favorable result.66 Mortality Scattered evidence suggests that PNES are associated with increased mortality. In one study, the authors obtained death certificate information in a cohort of 260 patients who presented with PNES between 1999 and 2004 from West of Scotland Regional Epilepsy Service, Southern General Hospital, Glasgow, UK. The follow-up period averaged 7.92 years, during which 17 patients died. Twelve out of 17 patients who died were under the age of 75 years, giving a premature mortality rate of 0.58% per year, compared with a Scottish mortality rate for the 40–75 year age-group of 0.41% per year. These results suggest that a diagnosis of PNES may be associated with a modest increase in mortality.67 Serious physical illness is prevalent in patients with PNES with an onset of their attacks after the age of 55 years. The development of physical illness (especially where this has been frightening to the patient) may be an important triggering factor for PNES, at least in a subset of patients.25 This means that the medical comorbidities 14 Hospital Physician Board Review Manual are probably responsible for increased mortality seen in patients with PNES and not the disease itself (ie, PNES). Besides, in the Scottish study mentioned above, patients came from a population that was deprived relative to the general Scottish population; the authors concluded that some excess mortality might be expected secondary to socioeconomic factors.67 On the other hand, in one study of 43 patients with PNES, 23% reported suicide attempts.68 This may also contribute to the increased mortality among patients with PNES. Health care costs PNES place a heavy demand on emergency and nonemergency health care services.69 It has been observed that most patients who have PNES diagnosed with video-EEG monitoring experience substantial subsequent reductions in health care utilization and costs.69–71 In one study, it was reported that in patients with a new diagnosis of PNES documented, pre-diagnosis medical costs exceeded $15,000 per patient and loss of work costs exceeded $22,000 per patient.72 In another study in 2013, overall costs dropped from the 12-month period preceding PNES diagnosis (mean costs: $4567) to the 12-month period following PNES diagnosis (mean costs: $2783). This equated to a cost reduction of nearly $1800 per person.71 In another study in 1998, there was an 84% average reduction in total seizure related medical charges in the 6 months following PNES diagnosis. Average diagnostic testing charges declined 76%, average medication charges decreased 69%, outpatient clinic visits declined 80%, and emergency room visits declined 97%.69 In a more recent study, the authors performed a 1-year prospective audit of use of a group of PNES-related health care items in www.turner-white.com Psychogenic Nonepileptic Seizures patients with newly diagnosed PNES, from PNES onset to diagnosis and from diagnosis to 6 months post-diagnosis. Before diagnosis, 28 patients were responsible for 14 general practitioner home visits, 31 ambulance calls, 34 emergency department visits, 21 hospital admissions, 2 standard EEGs, 28 short video-EEG recordings, and 5 ambulatory EEG recordings. In the 6 months following diagnosis, there were 2 emergency department visits (94.1% reduction), no hospital admissions (100% reduction), 2 ambulance calls (93.5% reduction), no general practitioner visits (100% reduction), and no EEGs (100% reduction).70 Overall, the burden of PNES is significant, particularly if it remains undiagnosed. Early diagnosis of PNES may save money and reduce the service utilization burden for patients and the health care system.69–72 Case presentation A 32-year-old single woman is referred for assessment of drug-resistant seizures. Her seizures started at age 16. She was at home with her parents at the time of her first seizure, which was early in the morning after she woke up; she has no recall of the event. The patient’s mother reported that she slumped over, became stiff, and began to shake; the event lasted about 2 minutes. A second similar episode occurred 1 month later. She has never experienced this seizure type again. She also mentions that she has experienced hand and body jerks in the morning since she was 15 years of age. At age 23 she developed new episodes of loss of awareness and responsiveness, stiffening and curving of her body, and intermittent pedaling for rather long periods, sometimes up to about 30 minutes. She was visited by a handful of neurologists and has tried 4 different antiepileptic drugs (ie, levetiracetam, lamotrigine, valproate, and zonisamide) with no difference in her current seizure frequency. Currently, she is taking lamotrigine 300 mg/day and levetiracetam 2000 mg/day. She has a very high health care utilization pattern. Within the past year she has consulted 3 different neurologists, has been to the emergency department 3 times, and has had 2 hospital admissions. Review of past history reveals that she has had irritable bowel syndrome since age 15. She also complains of chronic fatigue since she was 16 years of age. From grades 10 through 12, she missed about 10% of the school days due to health complaints. At age 22, she was diagnosed with “severe anxiety” and dropped out of college. Various psychiatric medications were given, but she had a number of intolerable side effects. Family history is significant for a 20-year-old brother with epilepsy. Her mother suffers from major depression. On neuropsychological testing, she has a normal IQ and memory, and no formal neurocognitive impairments. On the Beck Depression Inventory, she scores in the moderately depressed range. Her Beck Anxiety Inventory score is in the severely anxious range. During her 7-day admission at the inpatient video-EEG monitoring unit, she has 3 of her typical clinical seizures, none of which are associated with abnormal EEG activity, and all occur with normal awake posterior dominant rhythm. Her parents agree that the recorded episodes are typical events. However, her interictal EEG shows 4-Hz generalized spike-wave complexes. She leaves the hospital with a diagnosis of both epilepsy (ie, juvenile myoclonic epilepsy) and PNES. The health care team delivers the diagnosis to the patient and her family and also tries to persuade her to be actively engaged in her treatment www.turner-white.comEpilepsy Volume 3, Part 3 15 Psychogenic Nonepileptic Seizures plan. It is decided to slowly taper her levetiracetam (it has adverse psychiatric effects73) and keep her on lamotrigine (it is an AED and also a psychotropic agent with positive effects in depression). Referrals to a psychiatrist and also to a psychotherapist are also arranged. Discussion Epilepsy is not rare among patients with PNES. It is generally accepted that the prevalence of epilepsy is greater among patients with PNES than in the general population. These 2 disorders have a variety of differing symptoms and signs; however, none of them is pathognomonic to PNES. Thus, clinical differentiation of PNES from epilepsy sometimes proves to be difficult. Video-EEG monitoring with ictal recording is considered the gold standard test for the diagnosis of PNES. Diagnosis is achieved when a patient is observed having typical seizures without accompanying EEG abnormalities. Family members or witnesses who are familiar with the patient’s habitual seizures must agree that the recorded episodes are typical events.38 However, it is not always easy to distinguish between these 2 disorders, particularly if a patient is affected by both conditions. Treatment of PNES is not always an easy task either. The co-existence of these 2 conditions makes their treatment even more difficult and more challenging. Collaboration with mental health professionals should ideally start as soon as possible in the management process of patients with PNES. Mental health services are best utilized at 3 stages during the management of PNES: (1) while the diagnosis is being investigated to identify vulnerability traits, psychosocial factors, and psychiatric comorbidities; (2) during the delivery of the diagnosis, which also aims to engage patients in treatment; and (3) for the delivery of treatment.61 16 Hospital Physician Board Review Manual Conclusion PNES consist of paroxysmal changes in responsiveness, movements, or behavior that superficially resemble epileptic seizures, but lack a neurobiological origin similar to epileptic seizures and are not associated with electrophysiological epileptic changes. They are commonly diagnosed at epilepsy centers. One should have a high index of suspicion when a patient presents with atypical epileptic seizure and a high number of PNES risk factors. The diagnosis of PNES relies on a multidisciplinary evaluation and is usually based on different combinations of data. The combination of patient history, witness reports, clinician observations, and ictal and interictal EEG and ictal video is used for diagnostic determination. Recording a seizure, while under video-EEG monitoring, is the most reliable diagnostic test. The incidence of PNES was estimated to be 1.4 to 4.9 per 100,000 per year and the prevalence is calculated to be somewhere between 2 and 33 per 100,000, making it a significant psychoneurological condition. PNES tend to begin in adolescence and young adulthood, although the seizures can begin at any age. There is a predominance of female gender among patients with PNES. The proportion of patients with PNES who also have epilepsy has been reported to vary from 5% to 50%. PNES occur in a heterogeneous patient population. No single mechanism or contributing factor has been identified that is necessary and sufficient to explain PNES in all patients. The most commonly reported PNES associated factors include sexual abuse, physical abuse or neglect, traumatic brain injury, medical comorbidities, and psychiatric comorbidities. Even if one factor seems to play a predominant role in a particular patient, other factors are likely to have contributed and should not be ignored. www.turner-white.com Psychogenic Nonepileptic Seizures The neurobiology of PNES is still poorly understood. Obviously, PNES lack a neurobiological origin similar to epileptic seizures, but emerging evidence suggest that there is a neurobiological basis for these events. They could be the result of neurobiological dysfunction at specific brain networks. The initial phase of treatment is diagnosis delivery, the second phase is engagement, and the third phase involves an acute intervention. At the third phase, individualized psychotherapeutic and psychopharmacological treatment plans should be formulated. This phase has a primary goal of reduction of event frequency, but improvement in secondary measures such as severity of psychiatric comorbidities, quality of life, functional recovery, and medical resource utilization is also desired. The final phase of treatment is composed of long-term interventions. Fewer than 40% of newly diagnosed adults could be expected to become seizure-free within 5-years after diagnosis. In children, the figure of patients achieving seizure remission appears to be around 70%, which indicates a more favorable result. Scattered evidence suggests that PNES are associated with increased mortality. Overall, the burden of PNES is significant, particularly if it remains undiagnosed. Early diagnosis of PNES may save money and reduce the service utilization burden for patients and the health care system. Click to test your knowledge of this topic with Epilepsy Board Review Questions. References 1. Asadi-Pooya AA, Emami Y, Emami M. Psychogenic nonepileptic seizures in Iran. Seizure 2014;23:175–7. 2. Alsaadi TM, Marquez AV. Psychogenic non-epileptic sei- zures. Am Fam Physician 2005;72:849–56. 3. Kerr MP, Mensah S, Besag F, et al. International consensus clinical practice statements for the treatment of neuropsychiatric conditions associated with epilepsy. Epilepsia 2011;52:2133–8. 4. Brigo F, Igwe SC, Ausserer H, et al. Terminology of psychogenic nonepileptic seizures. Epilepsia 2015;56:e21–5. 5.O’Sullivan SS, Spillane JE, McMahon EM, et al. Clinical characteristics and outcome of patients diagnosed with psychogenic non-epileptic seizures: A 5-year review. Epilepsy Behav 2007;11:77 –84. 6. Hubsch C, Baumann C, Hingray C, et al. Clinical classification of psychogenic non-epileptic seizures based on videoEEG analysis and automatic clustering. J Neurol Neurosurg Psychiatry 2011;82:955–60. 7. Bodde NM, Brooks JL, Baker GA, et al. Psychogenic nonepileptic seizures-definition, etiology, treatment and prognostic issues: a critical review. Seizure 2009; 18: 543 –553. 8. Benbadis SR. Psychogenic nonepileptic seizures. Medscape. http://emedicine.medscape.com/article/1184694-overview. Accessed October 16, 2015. 9. Bagla R, Skidmore CT. Frontal lobe seizures. Neurologist 2011;17:125–35. 10. Asadi-Pooya AA, Emami M, Ashjazadeh N, et al. Reasons for uncontrolled seizures in adults; the impact of pseudointractability. Seizure 2013;22:271–4. 11. Asadi-Pooya AA, Emami M. Reasons for uncontrolled seizures in children; the impact of pseudointractability. Epilepsy Behav 2012;25:341–4. 12. Ricciardi L, Edwards MJ. Treatment of functional (psychogenic) movement disorders. Neurotherapeutics 2014;11:201–7. 13. Driver-Dunckley E, Stonnington CM, Locke DE, et al. Comparison of psychogenic movement disorders and psychogenic non-epileptic seizures: is phenotype clinically important? Psychosomatics 2011;52:337–45. 14.Hopp JL, Anderson KE, Krumholz A, et al. Psychogenic seizures and psychogenic movement disorders: are they the same patients? Epilepsy Behav 2012;25:666–9. 15.Voon V, Ekanayake V, Wiggs E, et al. Response inhibition in motor conversion disorder. Mov Disord 2013;28:612–8. 16.LaFrance WC, Baker GA, Duncan R, et al. Minimum requirements for the diagnosis of psychogenic nonepileptic seizures: A staged approach; A report from the International League Against Epilepsy Nonepileptic Seizures Task Force. Epilepsia 2013;54:2005–18. 17.Cuthill FM, Espie CA. Sensitivity and specificity of procedures for the differential diagnosis of epileptic and nonepileptic seizures: a systematic review. Seizure 2005;14: 293–303. 18.Asadi-Pooya AA, Sperling MR. Epidemiology of psychogenic nonepileptic seizures. Epilepsy Behav 2015;46:60–5. www.turner-white.comEpilepsy Volume 3, Part 3 17 Psychogenic Nonepileptic Seizures 19. Duncan R, Razvi S, Mulhern S. Newly presenting psychogenic nonepileptic seizures: Incidence, population characteristics, and early outcome from a prospective audit of a first seizure clinic. Epilepsy Behav 2011;20:308–11. 20.Sigurdardottir KR, Olafsson E. Incidence of psychogenic seizures in adults: a population-based study in Iceland. Epilepsia 1998;39:749–52. 21.Szaflarski JP, Ficker DM, Cahill WT, et al. Four-year incidence of psychogenic nonepileptic seizures in adults in Hamilton County, OH. Neurology 2000;55:1561–3. 22.Benbadis SR, Allen-Hauser W. An estimate of the prevalence of psychogenic non-epileptic seizures. Seizure 2000;9:280–1. 23. Asadi-Pooya AA, Emami M. Juvenile and adult-onset psychogenic non-epileptic seizures. Clin Neurol Neurosurg 2013;115:1697–1700. 24.Szabó L, Siegler Z, Zubek L, et al. A detailed semiologic analysis of childhood psychogenic non-epileptic seizures. Epilepsia 2012;53:565–70. 25. Duncan R, Oto M, Martin E, Pelosi A. Late onset psychogenic non-epileptic attacks. Neurology 2006;66:1644–7. 26. Alessi R, Valente KD. Psychogenic non-epileptic seizures at a tertiary care center in Brazil. Epilepsy Behav 2013;26:91–5. 27. Scévola L, Teitelbaum J, Oddo S, et al. Psychiatric disorders in patients with psychogenic non-epileptic seizures and drug-resistant epilepsy: a study of an Argentine population. Epilepsy Behav 2013;29:155–60. 28.Oto M, Conway P, McGonigal A, et al. Gender differences in psychogenic non-epileptic seizures. Seizure 2005;14:33–9. 29. Dhiman V, Sinha S, Rawat VS, et al. Semiological characteristics of adults with psychogenic non-epileptic seizures (PNESs): an attempt towards a new classification. Epilepsy Behav 2013;27:427–32. 30. Cronje G, Pretorius C. The coping styles and health-related quality of life of South African patients with psychogenic non-epileptic seizures. Epilepsy Behav 2013;29:581–4. 31. Jones SG, O’ Brien TJ, Adams SJ, et al. Clinical characteristics and outcome in patients with psychogenic non-epileptic seizures. Psychosom Med 2010;72:487–97. 32. Abubakr A, Wambacq I. Seizures in the elderly: Video/EEG monitoring analysis. Epilepsy Behav 2005;7:447–50. 33. Thomas AA, Preston J, Scott RC, Bujarski KA. Diagnosis of probable psychogenic nonepileptic seizures in the outpatient clinic: does gender matter? Epilepsy Behav 2013;29:295–7. 34. Noe KH, Grade M, Stonnington CM, et al. Confirming psychogenic non-epileptic seizures with video-EEG: sex matters. Epilepsy Behav 2012;23:220–3. 35. An D, Wu X, Yan B, et al. Clinical features of psychogenic non-epileptic seizures: A study of 64 cases in southwest China. Epilepsy Behav 2010;17:408–11. 18 Hospital Physician Board Review Manual 36.Lesser RP. Psychogenic seizures. Neurology 1996;46: 1499–1507. 37. Asadi-Pooya AA, Emami M, Emami Y. Gender differences in manifestations of psychogenic non-epileptic seizures in Iran. J Neurol Sci 2013;332:66–8. 38. Asadi-Pooya AA, Emami M. Demographic and clinical manifestations of psychogenic non-epileptic seizures: The impact of co-existing epilepsy in patients or their family members. Epilepsy Behav 2013;27:1–3. 39.Benbadis SR, Agrawal V, Tatum WO. How many patients with psychogenic nonepileptic seizures also have epilepsy? Neurology 2001;57:915–7. 40. Marchetti RL, Kurcgant D, Gallucci-Neto J, et al. Epilepsy in patients with psychogenic non-epileptic seizures. Arq Neuropsiquiatr 2010;68:168–73. 41. Martin R, Burneo JG, Prasad A, et al. Frequency of epilepsy in patients with psychogenic seizures monitored by videoEEG. Neurology 2003;61:1791–2. 42. Kollar B, Carnicka Z, Siarnik P, et al. The importance of interictal electroencephalography in paroxysmal states. Bratisl Lek Listy 2014;115:168–70. 43.Binnie CD, Stefan H. Modern electroencephalography: its role in epilepsy management. Clin Neurophysiol 1999;110: 1671–97. 44.Reuber M. The etiology of psychogenic non-epileptic seizures: Toward a biopsychosocial model. Neurol Clin 2009;27: 909–24. 45. Selkirk M, Duncan R, Oto M, Pelosi A. Clinical differences between patients with nonepileptic seizures who report antecedent sexual abuse and those who do not. Epilepsia 2008;49:1446–50. 46. Duncan R, Oto M. Predictors of antecedent factors in psychogenic nonepileptic attacks: multivariate analysis. Neurology 2008;71:1000–5. 47. LaFrance WC Jr, Deluca M, Machan JT, Fava JL. Traumatic brain injury and psychogenic nonepileptic seizures yield worse outcomes. Epilepsia 2013;54:718–25. 48. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry 1996;153:57–63. 49. Westbrook LE, Devinsky O, Geocadin R. Nonepileptic seizures after head injury. Epilepsia 1998;39:978–82. 50. Barry E, Krumholz A, Bergey GK, et al. Nonepileptic posttraumatic seizures. Epilepsia 1998;39:427–31. 51.Baslet G. Psychogenic non-epileptic seizures: A model of their pathogenic mechanism. Seizure 2011;20:1–13. 52.Alper K, Devinsky O, Perrine K, et al. Nonepileptic seizures and childhood sexual and physical abuse. Neurology 1993;43:1950–3. 53.Elliott JO, Charyton C. Biopsychosocial predictors of psychogenic non-epileptic seizures. Epilepsy Res 2014;108: www.turner-white.com Psychogenic Nonepileptic Seizures 1543–53. 54.Xue Q, Wang ZY, Xiong XC, et al. Altered brain connectivity in patients with psychogenic non-epileptic seizures: A scalp electroencephalography study. J Int Med Res 2013;41:1682–90. 55. Ding JR, An D, Liao W, et al. Altered functional and structural connectivity networks in psychogenic non-epileptic seizures. PLoS ONE 2013;8:e63850. 56. Ding J, An D, Liao W, et al. Abnormal functional connectivity density in psychogenic non-epileptic seizures. Epilepsy Res 2014;108:1184–94. 57. Arthuis M, Micoulaud-Franchi JA, Bartolomei F, et al. Resting cortical PET metabolic changes in psychogenic nonepileptic seizures (PNES). J Neurol Neurosurg Psychiatry 2015;86:1106–12. 58.van der Kruijs SJ, Bodde NM, Vaessen MJ, et al. Functional connectivity of dissociation in patients with psychogenic non-epileptic seizures. J Neurol Neurosurg Psychiatry 2012;83:239–47. 59.LaFrance W, Rusch M, Machan J. What is “treatment as usual” for nonepileptic seizures? Epilepsy Behav 2008;12: 388–94. 60. Kanner AM. Is the neurologist’s role over once the diagnosis of psychogenic nonepileptic seizures is made? No! Epilepsy Behav 2008;12:1–2. 61.Baslet G, Dworetzky B, Perez DL, Oser M. Treatment of psychogenic nonepileptic seizures: updated review and findings from a mindfulness-based intervention case series. Clin EEG Neurosci 2015;46:54–64. 62. LaFrance WC Jr, Reuber M, Goldstein LH. Management of psychogenic nonepileptic seizures. Epilepsia 2013;54 Suppl 1:53–67. 63. LaFrance WC Jr, Baird GL, Barry JJ, et al; NES Treatment Trial (NEST-T) Consortium. Multicenter pilot treatment trial for psychogenic nonepileptic seizures: a randomized clinical trial. JAMA Psychiatry 2014;71:997–1005. 64.Farias ST, Thieman C, Alsaadi TM. Psychogenic nonepileptic seizures: Acute change in event frequency after presentation of the diagnosis. Epilepsy Behav 2003;4: 424–9. 65.Reuber M, Pukrop R, Bauer J, et al. Outcome in psychogenic nonepileptic seizures: 1 to 10-year follow-up in 164 patients. Ann Neurol 2003;53:305–11. 66.Durrant J, Rickards H, Cavanna AE. Prognosis and outcome predictors in psychogenic nonepileptic seizures. Epilepsy Res Treat 2011;2011:274736. 67. Duncan R, Oto M, Wainman-Lefley. Mortality in a cohort of patients with psychogenic non-epileptic seizures. J Neurol Neurosurg Psychiatry 2012;83:761–2. 68. D’Alessio L, Giagante B, Oddo S, et al. Psychiatric disorders in patients with psychogenic non-epileptic seizures, with and without comorbid epilepsy. Seizure 2006;15:333–9. 69.Martin RC, Gilliam FG, Kilgore M, et al. Improved health care resource utilization following video-EEG-confirmed diagnosis of nonepileptic psychogenic seizures. Seizure 1998;7:385–90. 70. Razvi S, Mulhern S, Duncan R. Newly diagnosed psychogenic nonepileptic seizures: Health care demand prior to and following diagnosis at a first seizure clinic. Epilepsy Behav 2012;23:7–9. 71.Ahmedani BK, Osborne J, Nerenz DR, et al. Diagnosis, costs, and utilization for psychogenic non-epileptic seizures in a US health care setting. Psychosomatics 2013;54: 28–34. 72.Binder LM, Salinsky MC. Psychogenic nonepileptic seizures. Neuropsychol Rev 2007;17:405–12. 73. Kaufman KR. Antiepileptic drugs in the treatment of psychiatric disorders. Epilepsy Behav 2011;21:1–11. www.turner-white.comEpilepsy Volume 3, Part 3 19