Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
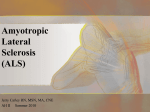
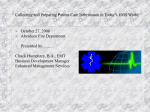
Assessment and Management of Swallowing in Patients with ALS Insights from SLPs at Hospital For Special Care’s Neuromuscular Clinic Kim Winter, M.A., CCC-SLP & Jennifer Chapin, M.S., CCC-SLP ASHA Convention – Nov. 17, 2011 – San Diego, CA Disclosure We do not have any financial relationship with a commercial interest whose products or services are discussed in this presentation. No funding was provided to support this presentation. HFSC’s Neuromuscular Clinic Multidisciplinary Team MDA and ALSA Certified Support Group Clinical Trials EMG Lab Muscle & Nerve Pathology Lab (in collaboration w/UCONN) What is ALS? A Review. Lou Gehrig’s Disease Progressive Degenerative Upper and Lower Motor Neuron Disease • Heterogeneous presentations • No known cause • No known cure • • • • ALS Epidemiology • Worldwide Incidence 0.86 to 2.4 per 100,000 per year (McGuire, V. & Nelson, L. M., 2006) • US Incidence 2 per 100,000 per year • Median survival rate: 3 years resulting in a prevalence rate of 6 per 100,000 per year. • Onset typically between 30-60 years of age • Male to Female Ratio of 1.6:1 What is ALS? Project ALS Video http://projectals.org/what-is-als/index.html ALS Neuroanatomy • UMN – neurons that have cell bodies in the brain and synapse on lower motor neurons. • LMN – neurons that have cell bodies in the cranial nerve nuclei or the anterior horn of the spinal cord and synapse on muscle. (ALS Society of Ontario, n.d.) Motor Neuron Damage • • • • • • Upper Motor Neurons Spasticity or Increased Tone Weakness (mildmoderate) Clumsiness or Loss of Dexterity Hyperreflexia Pathological Reflexes Pseudobulbar Affect (Emotional Lability) • • • • • • Lower Motor Neurons Weakness of Skeletal & Bulbar Muscles (moderate – severe) Hypotonia Hyporeflexia Fasciculations Muscle Atrophy or Wasting Cramps Bulbar vs. Spinal Muscle Innervation Shoesmith, C.L., & Strong, M.J. (2006) Spectrum of Motor Neuron Diseases fALS UMN onset LMN onset ALS PLS PMA ALS-plus syndrome Comparison of Motor Neuron Diseases Motor Neuron Neurologic Signs Muscle Involvement Primary Lateral Sclerosis (PLS) UMN only Bulbar & Spinal Pseudobulbar Palsy UMN only Bulbar only ALS UMN & LMN Bulbar & Spinal Median survival 4.32 yrs. (Czaplinski, et. al., 2006). Spinal-onset ALS UMN & LMN Spinal onset Median duration 21 mos. (del Aguila, et al., 2003). Bulbar-onset ALS UMN & LMN Bulbar onset Median duration 12 mos. (del Aguila, et al., 2003) Progressive Bulbar Palsy UMN & LMN Bulbar only Median survival 2-3 yrs. (Leigh, et. al., 2003). Progressive Muscular Atrophy (PMA) LMN only Spinal (Rarely Bulbar) Type Prognosis Mean duration 18.67 years (Norris, F., et al., 1993) Several years. Mean survival 13.25 years. (Norris, F., et. al., 1993). ALS • The most common MND. Sporadic ALS = 90-95% of all diagnosed cases (Qureshi et al., 2006) • Selective death of motor neurons in the brain and spinal cord that innervate skeletal (voluntary) muscles. • “No single biologic marker or investigative test to diagnosis ALS.” (Cwik, V.A., 2006, p. 99) • Diagnosis is heavily reliant on clinical recognition of combination of UMN & LMN signs and symptoms. Bulbar-Onset ALS • 25% of patients develop dysarthria & dysphagia first • LMN-predominant bulbar ALS: lingual weakness, atrophy & fasciculations. Often tongue affected first • UMN-predominant bulbar ALS: strained-spastic vocal quality, hyperreflexia, slow speech rate, pseudobulbar affect (Murray, B. & Mitsumoto, H., 2006) • May be incorrectly diagnosed initially or referred late to Neurologist by PCPs • Faster disease progression than Spinal-Onset • Shorter survival than Spinal-Onset (del Aguila, 2003) Normal Tongue Bulk Vs. Atrophied Tongue due to ALS Tongue Atrophy - ALS Normal Tongue Bulk Tongue Fasciculations in ALS Arm/hand Speech and swallowing Trunk and neck Legs/mobility ALS Prognostic Indicators • Age: Disease duration in sporadic ALS significantly greater under age 45 than over 55. (Norris, et al., 1993) • Gender: No significant difference (Murray, B., 2006) • Malnutrition: (low body mass) increased risk of death by 7.4 times (Desport, J.C., et al., 1999) • Occurrence of malnutrition equal spinal- vs. bulbar-onset ALS ALS Prognostic Indicators • Specialist Care: Mean survival longer in specialized ALS clinics (1080 days) than in general neurology clinics (775 days) (Chio, 2006) • Multidisciplinary care: 1. An independent predictor of survival & 2. Reduced risk of death by 47% in a 5 year study (Traynor, 2003) ALS-Functional Rating Scale - Revised (ALS-FRSr) http://www.outcomes-massmed.org/ALS/alsscale.aspx • Fine Motor, Gross Motor, Respiratory, Bulbar scores • Initial visit total ALS-FRSr score strongly predicts survival time • 267 ALS Clinic patients • Adjusted for age at baseline, sex and symptom duration. • Respiratory subscore was strongest predictor of survival time (Kaufman, P. et al. (2005) Terminal Stage of ALS • Usual cause of death: Progressive respiratory failure • Death usually within 3-5 years of diagnosis • Respiratory status is an important predictor of survival duration (Forced Vital Capacity = FVC, or Maximal Inspiratory Pressure = MIP) • Palliative/hospice care usually involved in preterminal and terminal stages Dysphagia Management In ALS : Current Research • No efficacy studies available on instrumental vs. clinical assessment approaches to diagnose and to monitor progression of dysphagia in ALS nor QOL outcomes and symptom management. • No efficacy studies available on the use of oral or pharyngeal exercises on maintaining duration of swallow function in ALS or whether they are harmful. • No evidence to support or refute the use of thickened fluids in patients with dysphagia due to ALS. One Approach to Management Philadelphia ALS Clinic • Assessment: Use rating scales (ALS-FRS-R, ALS Swallowing Severity scale), cervical auscultation, FEES & VFSS • Management: Diet modification, thickened fluids, preparatory sets, bolus size, slow rate, cold temperature fluids, carbonated liquids, supraglottic swallow, supersupraglottic swallow, Mendelsson maneuvers & chin tuck, modify method of intake (straw vs. cup vs. spoon, etc.) • Acknowledged paucity of supporting research Palovcak, Mancinelli, Elman & McCluskey (2007) HFSC Approach • Assessment: Use ALS-FRS-R, emphasis on clinical dysphagia eval, limited use of MBS/FEES • Management (Problem-solvers, not prescribers): Diet modification, rare use of commercial thickeners to prevent aspiration (patient choice - comfort), naturally thick beverages, reasonable bolus sizes, slow rate, energy conservation, early oral care emphasis, consider patient end-of-life wishes/QOL/comfort, rare use of maneuvers, no exercises, cough/choke response education, pill management, saliva management, alternative nutrition/hydration, counseling • Paucity of supporting research (We’re working on it!) HFSC Dysphagia Assessment • Screen patients every 3 months at scheduled clinic team visits • Clinical Dysphagia Evaluations with functional status changes – Nutrition/hydration management, comfort, strategy development, patient/family education & decision-making • Limited use of MBS or FEES Clinical Dysphagia Evals at HFSC • Thorough history & chart review • Review of medications & relevant side effects • Cranial Nerve Exam – Determine nerves/muscles involved & extent of impairment, hypothesize presence & severity of physiologic breakdown in swallow function • Respiratory Assessment - RT & MD input, patient complaints, FVC or MIP scores & rate of decline, respiratory rate • Oral Assessment – dentition (visible decay, biofilm, missing teeth), xerostomia, oral tissues, oral secretions, oral hygiene • Functional Assessment – Independence in performing oral care & self feeding, mobility, overall strength, conditioning & cognitive/language status. • Nutrition & Immune System – RD/MD input, recent illness, wounds, infections, immunocompromising meds or conditions, unintended weight loss, hydration status. Clinical Dysphagia Evals at HFSC • Feeding trials – Does this match hypothesis from cranial nerve exam? • Aspiration is not our primary concern. Consider comfort, adequate oral nutrition and hydration, QOL & patient end-of-life wishes. The AAN Practice Parameters (1999) • The American Academy of Neurology Practice Parameters in ALS (1999) indicates that a careful history should be conducted to identify dysphagia signs and symptoms. Asking the patient specific questions about their chewing and swallowing can be extremely revealing. • “There is no single test to detect dysphagia in patients with ALS” (p. 7). Instrumental Evaluations • Not objective – high degree in variability in interpretation among experienced SLPs. • Only one piece of the puzzle. • What are your clinical questions to determine management of dysphagia that you are unable to answer from a thorough clinical evaluation? **Should not just be +/- aspiration** • Will it change my plan of care? How? • Will it change the patient’s functional outcome? Additional Instrumental Considerations • Many patients feel like pin-cushions: EMGs, blood work, MRI/CT scans, DNA tests • Once diagnosis/prognosis is known, some do not want more tests • Maintain quality of life & comfort - Keep it simple • Is elimination of aspiration really possible? Modify a diet all you want, saliva is still being aspirated Pt/Family Involvement • Concern/clinical question after comprehensive clinical dysphagia evaluation Discuss options of instrumental exam. Candid discussion. • Pt/family involved in medical decision-making – Right to choose & decline. • Discuss pros & cons & your reasoning for considering an instrumental exam. • Document your education, their indication of understanding, their decision & changes to POC. Dysphagia Management in ALS • • • • • • • • • • Pneumonia Research Oral Care Saliva Management Liquids Solids Education on Responses to Coughing/Choking Use of Maneuvers Energy Conservation Exercise PEGs Aspiration Pneumonia In ALS Sorenson, E.J., Crum, B. & Stevens, J.C. (2007) • 40 ALS cases in Olmsted County, MN (Mayo Clinic), 1990-2005 (15 yrs.) • 23 males, 17 females. (1.3:1) • 12 Bulbar-onset, 28 Limb-onset • Mean survival = 26 mo., Median = 18 mo. • Aspiration pneumonia = 5/40 patients (13%). Less than the 21% in Langmore et al. (1998) • All with AP had prominent dysphagia and chronic compensated respiratory failure. Aspiration Pneumonia In ALS Sorenson, E.J., Crum, B. & Stevens, J.C. (2007) • PEG placed in 12 of 40 patients. • PEG placement more likely in Bulbar-onset patients (8 vs. 4 Limb-onset) • Mean time for placement: Bulbar-onset = 13 mo. vs. 17 mo. = Limb-onset • 6/12 underwent PEG placement with FVC >50% of predicted. 4 were <50% predicted. 2 unknown. • 2/12 with PEG died within 1 week of PEG. Both had FVC <50%. Aspiration Pneumonia In ALS Sorenson, E.J., Crum, B. & Stevens, J.C. (2007) • ALS patients in SNFs >7 times more likely to develop AP. Significant risk factor • No apparent association with continued oral intake or with medications. • AP was not more common in bulbar-onset patients, nor was PEG tube placement protective (3 patients with PEG tubes, 2 patients without). • Survival of those with AP was not significantly different than those without AP (26 months for both). Langmore et. al. (1998), Predictors of Aspiration Pneumonia: How Important is Dysphagia? • Prospective study, 189 elderly patients: acute care, outpatient & ECFs followed 4 yrs. for aspiration pneumonia (AP). • 41 of the 189 patients (21.7%) developed AP, consistent with US prevalence data. • 81% of patients who developed AP had oral-pharyngeal dysphagia. • 47% of patients who did not develop AP had oralpharyngeal dysphagia. • Of the documented aspirators, only about 38% developed AP. • 27% of those with AP were tube fed (NPO). Langmore et. al. (1998) Significant predictors of AP were: • Dependent for oral care • Tube fed before AP • Dependent for feeding • Number of medications • Smoking • Multiple medical diagnoses • Number of decayed teeth “dysphagia by itself is not sufficient to cause pneumonia” (p. 76). Langmore et. al. (1998) “This role of dysphagia and aspiration in the pathogenesis of pneumonia may be better understood by considering the contributions of colonization and host resistance to the process. Aspiration must occur, but aspiration will only lead to pneumonia if the material aspirated is pathogenic to the lungs and if the host resistance to the inoculum is compromised” (p. 76). Pathogenesis of Bacterial Respiratory Infection Respiratory tract below the larynx is sterile in normal, healthy adults. Infection occurs with one or more of the following conditions: • Deficient host defenses • Highly virulent pathogen • Overwhelming inoculum (high bacteria load) (Scannapieco, 1999) Pathogenesis of Bacterial Respiratory Infection Contamination of lower airway by 1. Inhaled aerosolized droplets 2. Aspiration of oral secretions containing microorganisms First, oral and pharyngeal surfaces must be colonized by oral and respiratory pathogens which are shed into secretions that then contaminate the pulmonary tree. (Scannapieco, 1999) Langmore et. al. (1998) Bacterial flora in the oral cavity and pharynx can be altered by: • Severe underlying disease • Inactivity • Malnutrition • Presence of oral & dental disease • Medications Sialorrhea – Excessive Salivation • True or pure sialorrhea is rare. • In ALS - inability to manage normal salivation weakness of oral & pharyngeal muscles. • ~50% of ALS patients experience it. • Drooling is embarrassing, causes social stigma, leads to difficult social integration, depression, exacerbates difficulty eating, speaking & breathing, causes oral tissue breakdown & chapping. Treatments for Sialorrhea in ALS • Tricyclic antidepressants (amytriptyline) • Atropine sulfate • Glycopyrrolate • Hyoscyamine • Scopolamine • Tissues • Portable suction device • Botox injections to salivary glands (temporary) • Irradiation of salivary glands (permanent) (Andrews, J., 2009) When Saliva is Too Thick • Maintain adequate hydration with oral water/ice chips • Use a cool mist humidifier • Make sure there is a humidifier on non-invasive ventilation • Frequent oral care, use of oral moisturizers • Oral suction • Avoid over-use of drying medications or procedures. Hyposalivation Affects QOL and oral health • Xerostomia = dry mouth feeling • Frequent thirst • Difficulty swallowing • Difficulty speaking • Difficulty eating dry foods • Need to drink water frequently • Difficulty wearing dentures • Pain and irritation of oral mucosa • Burning feeling in the tongue • Dysgeusia = distortion of taste sensation (Llena-Puy, 2006) Hyposalivation Signs to watch for: • Loss of glossiness of oral mucosa • Dryness of oral mucosa • Thin, cracked oral mucosa • Fissures in the tongue dorsum • Thick saliva • Angular cheilitis (sore, reddened, swollen cracks or fissures in the corner of the mouth) • Increased frequency of oral infection, especially Candida sps. • Presence of dental caries in atypical locations • Increased size of major salivary glands (Llena-Puy, 2006) Xerostomia Xerostomia • May increase risk of bacterial colonization in oral cavity & pharynx • Which may increase the risk of pneumonia • Reduced salivary flow results in poor clearance of oral bacteria • Increases the potential for aspiration of a much larger bacterial load. • Makes oral care all that more important! (Limeback, 1998) Oral Hygiene Recommendations 3 Major Components Shared with Hand-Washing • Friction – loosen bacteria, plaque and debris Toothettes do not provide enough! • Antiseptic – kill bacteria. Be careful of antibiotics resulting in increasingly resistant strains of bacteria. Avoid alcohol based antiseptics. • Time – minimum of 2 minutes Oral Hygiene Recommendations • • • • Friction Soft bristled or electric toothbrush is the best. Electric or child-sized may work well for better access. Suction toothbrushes available for vent patients or those who have severe dysphagia. Toothettes only good for removing debris. http://umanitoba.ca/dentistry/ccoh/ccoh_longTermCareFacts.html Oral Hygiene Recommendations • • • • • • • Antiseptic/Antiplaque Avoid alcohol – drying to oral mucosa. Chlorhexidine – apply to teeth and oral surfaces after brushing and suctioning (ICU, vent patients). Only for short-term use for high-risk patients. Cetylpyridium chloride – oral antiseptic and antiplaque solution (Sage products) Biotene products work well with xerostomic patients. Nystatin – effective for Candidiasis/yeast/thrush Hydrogen peroxide – oral debriding solution Avoid lemon-glycerin swabs – cariogenic and very acidic. Oral Hygiene Recommendations • Daily oral assessment is key in facilities – colonization happens quickly! • Brush teeth, tongue, palate, inside of cheeks – all oral surfaces to loosen bacteria throughout the oral cavity. • Minimum of 2x/day. • Oral hygiene must be performed even if the patient is edentulous! • Should be performed more frequently for patients who have xerostomia, mouth-breathers or those who are NPO. Oral Hygiene Recommendations • For patients with dysphagia, we recommend that they receive oral care PRIOR to PO intake. • Patients that can perform oral care themselves should be encouraged to do so and assisted as needed. Involve OT early! • Dentures need to be brushed too in order to loosen bacterial plaques. Soaking is not enough. Oral Hygiene Recommendations • Keep equipment clean & stored in a clean, dry place. • Avoid reintroducing bacteria back into cleaned oral cavity. Yankauer suction devices are notorious for this. Change them every 24 hours. • If a patient is able to expectorate secretions, have them use a tissue and throw the tissues away after each use. Liquids: To Thicken or Not To Thicken • Is there an effective alternative to thickening liquids? • Thickened liquids affect QOL & hydration. • Thick liquids require increased pressure generation vs. thin liquids require increased control/timing. • Many dislike thickened fluids decreased fluid intake. • In trying to solve a problem with aspiration or coughing with thin liquids, thickening fluids may result in new or aggravated existing problem with dehydration. • Weigh the risks to benefits. Discuss with patients. Dehydration and Thickened Fluids • No significant difference in absorption between thickened fluids and water, • BUT patients on thickened fluids have a decreased fluid intake compared to those allowed thin liquids (Sharpe et al., 2007). • Dysphagia patients on thickened liquids were found by Vivanti et al. (2009) to receive most of their fluid from food, rather than beverages. • Fluid intake is decreased if the beverages are not palatable or if there is a lack of variety. Protocol 201 – Dementia & PD • Part 1 found that honey thick liquids eliminated aspiration more than nectar, which was also more than thin liquids with chin-down posture during VFSS (all comparisons were significant statistically). (Logemann, J. A., et al., 2008) • Part 2 found that participants drinking nectar thick liquids had a decreased incidence of pneumonia compared to those drinking honey thick liquids over a period of 3 months (significant at p < 0.10). All were randomly assigned and performed equally well (no aspiration) or poor (aspirated in all conditions) on VFSS. (Robbins, J, et al., 2008) Thin Liquid Aspiration - Considerations • • • • • • You’ve identified that the patient aspirates with thins How much & how often? Do they have a strong cough for airway protection? Is their coughing uncomfortable or distressing? Ask the patient if their coughing bothers them. Do any postures eliminate the cough? Does changing the method of presentation eliminate the cough? Condition of their dentition, oral tissues and oral hygiene regimen? Hx of respiratory infection or pneumonia? HFSC Approach to Liquids • Rarely recommend commercial thickeners, offer choice for patients with uncomfortable or distressing coughing with thin liquids (supercoughers, hyperreflexive). • Suggest naturally thicker beverages like V-8, fruit nectars (Goya), smoothies, etc. for comfort & increased palatability. • We support use of unthickened water/ice chips. • Be careful about the assumption that aspiration status on MBS/FEES = status during meals throughout the day. Variable function. Alternate Liquid Delivery One-Way Straws Sip Tip Cup Provale Cup HFSC Approach to Liquids • If I have to choose between a patient aspirating small amounts of thin liquids without distress vs. thickened fluids with the risk of aspiration, I will choose thins. This is based on my own experience and comfort with a certain level of aspiration. • Recall that in the Langmore study that 38% of known aspirators developed AP…which means that 62% of known aspirators did not. Solids – Oral Prep. & Oral Dysphagia • Reduce choking risk for patients who are having difficulty with solids due to oral issues. • Specific food avoidances – patient identified. • Most patients do this themselves – They know. • Add extra moisture to aide with chewing and lubrication. • Dice solids if a patient can still chew, but has difficulty with thorough mastication or fatigue. • Food process to allow for texture when mastication or tongue lateralization becomes an even greater problem. • Then puree if necessary. Teaching Caregiver Responses to Coughing and Choking • Teach them the difference. • Cough is the body’s natural airway defense mechanism, and it’s important. • Choking is when the airway is obstructed. • Encourage a cough. Don’t slap on the back. A hand rubbing the patients shoulder is ok. Try not to outwardly panic, as it makes the patient panic more. • Red in the face is ok. Blue in the lips and fingernails is not. • Laryngospasm common – UMN hyperreflexia • Heimlich maneuver with choking. Swallow Maneuvers – “Chin Tuck” • Literature describes different head and neck flexion postures. Hard to know what’s what. • Very clinically popular. • Physiologically should be used to reduce aspiration before the swallow due to reduced BOT retraction & delayed onset of pharyngeal swallow. • Variable rates of efficacy at reducing aspiration. Solid studies show it reduces aspiration ≤50% of the time (Ashford, et al., 2009). • Concern about patients with reduced hyolaryngeal excursion and use of chin to chest posture. Does it further limit anterior movement of the hyoid and laryngeal elevation? • Probably counterproductive for people with lip weakness. Our “Chin Tuck” Alternative • Slight chin down posture – “Look at your knees” • Chin should not drop to chest • Use gravity to keep liquids in the mouth until patient is ready to swallow in cases of weak posterior tongue with posterior bolus loss. • Seems less likely to cause pain from deep cervical flexion and interfere with hyolaryngeal excursion • No empirical evidence to support or refute, but patients prefer it (less neck pain). Other Swallow Maneuvers • Supraglottic swallow, super-supraglottic swallow, Mendelsohn maneuver. • Little sound empirical evidence that these techniques work to alter swallow physiology by eliminating aspiration or that they improve swallow function in patients with neurologically induced dysphagia. (Ashford, et al., 2009) • Some patients cannot perform them. • More concerning is the extra effort that patients need to exert to perform these maneuvers. Fatiguing in ALS. Fatigue - Energy Conservation Energy Conservation Strategies • Consider smaller, more frequent meals throughout the day rather than 3 large meals. • Make your meals calorie-dense. Adding extra sauces, gravies and condiments provide moisture and lubrication while adding extra calories, sugar and fat. • Clear pharyngeal residue with liquids (nutritive) rather than a double swallow (non-nutritive). • Have a variety of food textures and avoid having several foods that are tough to chew, orally manipulate and swallow at the same meal. • Consider 1-way straws to save energy. Use of Swallowing Exercises • Easterling & Koster (In Jones & Rosenbek, 2010) “Active therapeutic swallow exercise regimen is contraindicated, as it promotes muscle fatigue and may promote motor neuron degeneration” (p. 5) • Fatigue from exercise is rarely discussed in SLP literature. (Clark, 2003) • Until recovery occurs, muscles cannot produce or sustain forces produced before exercise. • ALS degeneration may impede muscle recovery. Use of Swallowing Exercises • Clark (2003) – Strengthening exercise in ALS may functionally decrease strength levels without any long-term benefit of increased strength. • Recommend energy conserving strategies over strengthening exercise programs. • Applies to use of compensatory strategy selection used during meals as well. Use of Swallowing Exercises • Clark (2005) described published studies looking at gross motor physical exercise in ALS showing some short term benefits. • HOWEVER, unknown whether similar benefits of specific exercise occurs with ALS patients with swallowing. • Patients with ALS come to our clinic with varied exercise programs: duration, repetitions, sets, frequency, specific exercises - all different. • We recommend discontinuing them & reach out to SLPs who are also involved in our patients’ care. Potential for Neuroplasticity? Rosenbek (2011) Swallowing and Neurodegenerative Diseases (ASHA webinar) . • Advocated for very low resistance strengthening with reduced intensity • Stretching • General exercise • Skilled treatment for swallowing “hard but not too hard” Considerations – Swallow Exercises and ALS 1. 2. 3. 4. How are you measuring benefit? How long are patients to continue the program? What are the criteria to stop the program? When do you follow-up to determine whether the patient is benefitting or not? 5. Do you tell patients this may not help and it may make things worse or that there is no evidence to support or refute? 6. Are you offering false hope of recovery? Alternate Nutrition and Hydration • Per the American Academy of Neurology Practice Parameters on ALS (1999), a PEG should be recommended BEFORE the FVC drops to <50% of predicted and not in the preterminal phase of disease progression. • PEG is indicated with symptomatic dysphagia and weight loss resulting in inadequate caloric intake, dehydration or ending meals early due to fatigue or choking. Alternate Nutrition and Hydration • PEG and J tubes do NOT prevent aspiration pneumonia. Therefore, prevention of AP is NOT an indication for PEG placement in patients with ALS. • “Although a barium swallow study may provide supportive evidence for dysphagia, the indication for PEG in ALS depends on the presence of inadequate oral intake and diminished quality of life due to choking rather than the result of a swallow study” (AAN Practice Parameters, Miller, 1999, p. 7) PEG Tubes Progressing ALS AAN Practice Parameters, 1999 Possible Complications of PEG Tubes In ALS Patients Aspiration Bleeding Infection Peritonitis (Beggs, K., Choi, M. & Travlos, A., 2010) Aspiration pneumonia is the most common cause of death after PEG placement in general (Fox, K.A. et al, 1995 as cited in Plonk, W.M., 2008, ASHA Telephone Seminar) FVC Decline & PEG Placement Research!! Research Needs • Impact of oral hygiene emphasis on incidence of aspiration pneumonia in ALS. • Comparison of outcomes across ALS Centers across the U.S. and internationally. Best practice? • Use of naturally thick vs. commercial thickeners on incidence of aspiration pneumonia, hydration and QOL in ALS. • Effects of swallow exercise in early ALS – What? When? How often? How long? • Breathing exercise/training in ALS (e.g. EMST) Take Home Points • ALS patients are not all alike in terms of onset, progression, symptoms and prognosis. • Compensation approach, not remediation. • Clinical evaluations that include cranial nerve exams are crucial in guiding subsequent decisions. • Match your management to the diagnosis and etiology. ALS is different than a stroke. • Swallow exercise should be cautiously considered and closely monitored if employed. • Oral care and energy conservation are key! • Contact your closest ALS Center for guidance & support. Case Study – Bulbar-Onset ALS • 45 year old man (BD) • Former smoker of 2-3 ppd x 15 years, quit 13 years ago • Onset of slurred speech and slight right facial droop in Oct. 2008 – etiology unknown. • Referred to Brain MRI 10/08 – Normal • Labs – HSV-1 Antibodies • PCP Diagnosis 11/08 – Bell’s Palsy secondary to acute HSV-1 infection. • Speech Therapy - Exercises for dysarthria. Case Study 4/09 – Slurring is worse. Left thumb involvement. Complaint of tongue weakness and difficulty eating and drinking. 6/09 – Complaint of lost voice, non-productive cough, SOB, fever, neck cramps, problem with left thumb. PCP – Tonsillitis, Bells Palsy, DJD? 7/09 – Review tests, resolved tonsillitis 7/09 – Neurologist Diagnosis– Medullary CVA that is not visible on imaging tests. Case Study • 7/09 – Bilateral carpal tunnel syndrome with decreased strength in both hands, left greater than right; Reflex testing slightly increased. Slight asymmetry of CN IX – Palate. • Spine MRI – moderate cervical stenosis C6-C7 and DJD at same level. • 7/09 – MBS oral and pharyngeal swallow WNL, mild CP hypertrophy. • 8/09 – Spinal work-up: Atrophy left hand muscles. Case Study • 8/09 – Cervical decompression and fusion C6-C7. • Re-admitted to acute care day after D/C home – syncope likely due to drug interaction. • Head CT negative, CXR showed haziness in right base, neck CT showed post surgical changes, neck X-ray showed prevertebral soft tissue swelling at fused level Case Study • Patient complaint of globus sensation prompted SLP involvement. Per MD D/C summary, he “failed” the first MBS. NG tube placed, which patient reports he pulled. • He “passed” the second MBS: puree with nectar thick liquids. Pt reports being told his lungs were “filled with food,” however, no diagnosis of pneumonia was documented nor were antibiotics prescribed. Case Study • MD D/C Note: First mention of ALS being included in the differential. Felt it was unlikely given rapid progression. • Patient had follow-up SLP services per his report. He continued on a modified diet of puree and nectar for 6 months. • He lost 17 pounds during that period. Case Study • 11/09 – Neurology – Dysarthria, left hand atrophy and weakness persisted. Referred to SLP due to dysphagia post-op. • SLP evaluated and observed fasciculations and tongue atrophy on clinical exam. Referred the patient to HFSC SLP with ? of motor neuron disease. Case Study • 3/10 – Kim evaluated this patient: mild-mod. Flaccid dysarthria with hypernasality, lingual and labial weakness resulting in imprecise consonant production. • Clinical dysphagia eval showed mild-mod oralpreparatory and oral dysphagia due to decreased lingual and labial strength/ROM, presence of lingual fasciculations and atrophy resulting in slow mastication. Pharyngeal phase WNL. Referred to Neuromuscular Clinic. Case Study • 1 week later – NMC Eval: progressive dysarthria, dysphagia, loss of hand dexterity, cramping in UEs, neck & chest, increased emotionality, tongue atrophy & fasciculations with very slow movements, exaggerated jaw jerk, fasciculations of the UEs, weakness & atrophy of intrinsic hand muscles, intact sensation & coordination. • Working dx of Progressive Bulbar Palsy, with likely bulbar-onset ALS. 4/10 – EMG showed chronic denervation in 3 spinal areas, which confirmed ALS diagnosis. Case Study • 9/10 – SLP Consult in NMC: Progressive moderate mixed (flaccid/spastic) dysarthria characterized by slow rate, consonant imprecision, hypernasality, slightly strainedstrangled vocal quality, reduced breath support & speech intelligibility due to lingual, labial & palatal weakness, laryngeal spasticity & respiratory muscle involvement. • Progressive mild-mod. oral prep., oral & pharyngeal dysphagia due to labial and lingual weakness & reduced ROM & reduced hyolaryngeal excursion and complicated by fatigue and respiratory compromise with reduced cough force. References Amyotrophic Lateral Sclerosis Society of Ontario (n.d.). What is ALS? Retrieved from http://www.alsont.ca/about-als/ Andrews, J. (2009). Amyotrophic lateral sclerosis: Clinical management and research update. Current Neurology and Neurosciences Reports, 9, 59-68. Ashford, J. et al. (2009). Evidence-based systematic review: Oropharyngeal dysphagia behavioral treatments. Part III – Impact of dysphagia treatments on populations with neurologic disorders. Journal of Rehabilitation Research & Development, 46, 195-204. Beggs, K., Choi, M. & Travlos, A. (2010). Assessing and predicting successful tube placement outcomes in ALS patients. Amyotrophic Lateral Sclerosis, 11, 203-206. Bratland, C. V., O’Donoghue, C. R. & Rocchiccioli, J. T. (2010). Dehydration and dysphagia: Challenges in the older adult. Journal of Medical Speech-Language Pathology, 18(3), 1-10. Chio, A., et. al. (1985). A survival analysis of 155 cases of progressive muscular atrophy. Acta Neurology Scandinavia, 72, 407-413. Chio, A., et al. (2002). Piemonte and Valle d’Aosta Register for ALS (PARALS). Early symptom progression rate is related to ALS outcome: a prospective populationbased study. Neurology, 59, (12), 99-103. References Chio, A., et al. (2006). Positive effects of tertiary centres for amyotrophic lateral sclerosis on outcome and use of hospital facilities. Journal of Neurology, Neurosurgery, & Psychiatry, 77, 948-950. Clark, H. M. (2003). Neuromuscular treatments for speech and swallowing: A tutorial. American Journal of Speech-Language Pathology, 12, 400-415. Clark, H.M. (2005) Therapeutic exercise in dysphagia management: Philosophies, practices, and challenges. Perspectives on Swallowing and Swallowing Disorders, 14, 24-27. Cwik, V. A. (2006). ALS clinical motor signs and symptoms. In Mitsumoto, et al. (Eds.). Amyotrophic Lateral Sclerosis (pp. 99-115). New York, NY: Taylor & Francis Group. Czaplinski, A., et al. (2006). Slower disease progression and prolonged survival in contemporary patients with amyotrophic lateral sclerosis: Is the natural history of amyotrophic lateral sclerosis changing? Archives of Neurology, 63, 1139-1143. del Aguila, M.A., et al. (2003). Prognosis in amyotrophic lateral sclerosis: A population-based study. Neurology, 60, 813-819. Desport, J.C., et al. (1999). Nutritional status is a prognostic factor for survival in ALS patients. Neurology, 53, 1059-1063. References Easterling, C. & Koster, E. (2010). Amyotrophic lateral sclerosis (ALS). In Jones, H.N. & Rosenbek, J.C. (Eds.), Dysphagia in Rare Conditions: An Encyclopedia, (pp. 1-7). San Diego, CA: Plural Publishing, Inc. El Salvador Atlas of Gastrointestinal Video Endoscopy. (n.d.). Pill Esophagitis. Retrieved from http://www.gastrointestinalatlas.com/English/Esophagus/Pill_Esophagitis/pill_esopha gitis.html Goozée, J. V. & Murdoch, B. E. (2009). Progressive bulbar palsy (PBP). In McNeil, M. R. (Ed.), Clinicial Management of Sensorimotor Speech Disorders (2nd ed.), (pp. 380-384). New York, NY: Thieme Medical Publishers, Inc. Jackson, C.E. & Bryan, W.W. (1998). Amyotrophic lateral sclerosis. Seminars in Neurology, 18, 27-39. Kaufman, P. et al. (2005). The ALSFRSr predicts survival time in an ALS clinic population. Neurology, 64, 38-43. Langmore, S. E., et al. (1998). Predictors of aspiration pneumonia: How important is dysphagia? Dysphagia, 13(2), 69-81. References Leigh, P. N., et al. (2003). The management of motor neurone disease. Journal of Neurology, Neurosurgery and Psychiatry, 74, (Suppl 4), iv32-iv47. Marcus, J. A. & Bedlack, R. S., (2009). Primary lateral sclerosis (PLS). In Jones, H. N. & Rosenbek, J. C. (Eds.). Dysphagia In Rare Conditions: An Encyclopedia (pp. 467-472). San Diego, CA: Plural Publishing, Inc. Limeback, H. (1998). Implications of oral infections on systemic diseases in the institutionalized elderly with a special focus on pneumonia. Annals of Periodontology, 3, 262-275. Llena-Puy , C. (2006). The rôle of saliva in maintaining oral health and as an aid to diagnosis. Medicina oral, patología oral y cirugía bucal, 11, E449-455. Logemann, J. A. et al. (2008). A randomized study of three interventions for aspiration of thin liquids in patients with dementia or Parkinson’s disease. Journal of Speech, Language, and Hearing Research, 51, 173-183. McGuire, V. & Nelson, L. M. (2006). Epidemiology in ALS. In Mitsumoto, et al. (Eds.). Amyotrophic Lateral Sclerosis (pp. 17-41). New York, NY: Taylor & Francis Group. Miller, R. G., et al. (1999). Practice parameter: The care of the patient with amyotrophic lateral sclerosis (An evidence-based review): Report of the Quality Standards Subcommittee on the American Academy of Neurology, Neurology, 52, 1311. Retrieved June 15, 2009, from http://www.neurology.org/cgi/content/full/52/7/1311 References Miller, R.G., et al. (2009). Practice parameter update: The care of the patient with amyotrophic lateral sclerosis: Drug, nutritional, and respiratory therapies (an evidencebased review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology, 73, 1218-1226. Retrieved September 19, 2010, from www.neurology.org/cgi/content/full/73/15/1218 Miller, R. & Britton, D. (2009). Progressive bulbar palsy (PBP). In Jones, H. N. & Rosenbek, J. C. (Eds.). Dysphagia In Rare Conditions: An Encyclopedia (pp. 473-490). San Diego, CA: Plural Publishing, Inc. Motor Neurone Disease Association. (2007, February). Progressive Muscular Atrophy. Retrieved September 19, 2010 from http://www.mndassociation.org/life_with_MND/pmapls/what_is_PMA.html Murray, B. (2006). Natural history and prognosis of amyotrophic lateral sclerosis. In Mitsumoto, et. al. (Eds.). Amyotrophic Lateral Sclerosis (pp. 227-55). New York, NY: Taylor & Francis Group. Murray , B & Mitsumoto, H. (2006) The spectrum of motor neuron disorders. In Brown, R.H., Swash, M., & Pasinelli, P. (Eds.). Amyotrophic Lateral Sclerosis (2nd ed.) (pp. 3-24). Boca Raton, FL: Taylor & Francis. Norris, F., et. al. (1993). Onset, natural history and outcome in idiopathic adult motor neuron disease. Journal of Neurology Science, 118, 48-55. References Palovcak, M. Mancinelli, J.M., Elman, L. B. & McCluskey, L. (2007). Diagnostic and therapeutic methods in the management of dysphagia in the ALS population: Issues in efficacy in the out-patient setting. Neurorehabilitation, 22, 417-423. Plonk, W. M. (May 15, 2008). PEG Tubes In Adults: Use, Overuse, and the SLP’s Role. [ASHA Telephone Seminar 0809]. Retrieved from http://www.asha.org/eweb/OLSDynamicPage.aspx?title=PEG%20Tubes%20in%20A dults:%20Use,%20Overuse%20%26%20the%20SLPs%20Role&webcode=olsdetails Qureshi, M. M., et. al. (2006). Analysis of factors that modify susceptibility and rate of progression in amyotrophic lateral sclerosis. Amyotrophic Lateral Sclerosis, 7, 173182 Shoesmith, C.L., & Strong, M.J. (2006) . Amyotrophic lateral sclerosis: An update for family physicians. Canadian Family Physician, 52, 12, 1563-1569. Robbins, J., et al. (2008). Comparison of 2 interventions for liquid aspiration on pneumonia incidence: a randomized trial. Annals of Internal Medicine, 148, 509518. Scanniapieco, F.A. (1999). Role of oral bacteria in respiratory infection. Journal of Periodontology, 70, 793-802. Sharpe, K., et al. (2007). Thickened fluids and water absorption in rats and humans. Dysphagia, 22, 193-203. Siddique, T. & Dellefave, L. (2006). Familial ALS and genetic approaches to ALS. In Mitsumoto, et. al. (Eds.). Amyotrophic Lateral Sclerosis (pp. 141-166). New York, NY: Taylor & Francis Group References Singer, M. A., et. al. (2007). Primary lateral sclerosis. Muscle Nerve, 35, 291-302. Sorenson, E.J., Crum, B. & Stevens, J.C. (2007). Incidence of aspiration pneumonia in ALS in Olmstead County, MN. Amyotrophic Lateral Sclerosis, 8, 87-89. Traynor, B.J., et al. (2003). Effects of a multidisciplinary ALS clinic on survival. Journal of Neurology, Neurosurgery & Psychiatry, 74, 1258-1261. University of Manitoba Faculty of Dentistry Health Promotion Unit Centre for Community Oral Health (n.d.). Oral care health promotion fact sheets & video clips for mouth care in long term care. Retrieved at http://umanitoba.ca/dentistry/ccoh/ccoh_longTermCare.html Vivante, A. P., et al. (2009). Contribution of thickened drinks, food and enteral and parenteral fluids to fluid intake in hospitalized patients with dysphagia. Journal of Human Nutrition and Dietetics, 22, 148-155.. Yoon, M.N. & Steele, C.M. (2007). The oral care imperative: The link between oral hygiene and aspiration pneumonia. Topics in Geriatric Rehabilitation, 23, 280-288. Yorkston, K., Miller, R., & Strand, E. (2004). Management of speech and swallowing in degenerative diseases (2nd Edition). Austin, TX: PRO-ED. Cranial Nerve Exam Resources • Gertz, S. D. (2007). Liebman’s Neuroanatomy Made Easy and Understandable (7th ed.). Austin, TX: pro-ed. • Love, R.J. & Webb, W. G. (2001). Neurology for the SpeechLanguage Pathologist (4th ed.). Boston, MA: ButterworthHeinemann. • Wilson-Pauwels, L. Akesson, E.J., Stewart, P.A. & Spacey, S.D. (2002). Cranial Nerves In Health and Disease (2nd ed). Lewiston, NY: BC Decker, Inc. • http://anatomy.med.umich.edu/nervous_system/antneck_tab les.html You can also find plenty of decent videos illustrating cranial nerve examinations on You Tube! Useful Websites ALS Information ALS Association: http://www.alsa.org/ MDA Association – ALS Division: http://www.als-mda.org/ American Academy of Neurology: http://www.aan.com/ The Center for Neurologic Study: http://www.cnsonline.org/ Project ALS: http://www.projectals.org/ Patient/Caregiver Resources and Online Support Groups ALS Forums: http://www.alsforums.com Patients Like Me - ALS/MND: http://www.patientslikeme.com/als/community Useful Websites ASHA Swallowing and Feeding Disorders Technical Report: http://www.asha.org/docs/html/TR2001-00150.html ASHA Swallowing and Feeding Disorders Position Statement: http://www.asha.org/docs/html/PS2002-00109.html ASHA Swallowing and Feeding Disorders Knowledge and Skills for Service Delivery: http://www.asha.org/docs/html/KS2002-00079.html ASHA Special Interest Division 13 – Dysphagia (with paid membership includes list serve access): http://www.asha.org/Members/divs/div_13.htm International Free Dysphagia List Serve (dysphagia.com): http://lists.b9.com/mailman/listinfo/dysphagia University of Manitoba Centre for Community Oral Health – Faculty of Dentistry & School of Dental Hygiene: Oral Care Fact Sheets and Instructional Videos: http://www.umanitoba.ca/dentistry/ccoh/ccoh_longTermCare.html#PDF