Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
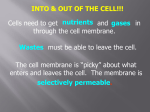
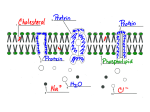
Basic Pharmacology Basic concepts in pharmacology, drug action and pharmacokinetics Part 3: The pharmacokinetic processes of absorption and distribution Gustav Schellack, BCur, AdvUnivDiplNursSc(HSM), HonsBSc(Pharmacology) Training specialist in the pharmaceutical industry, specialising in clinical research and applied pharmacology Correspondence to: Gustav Schellack, e-mail: [email protected] Keywords: pharmacokinetics, biological barriers, cell membrane, diffusion, active transport Application Made Easy for Nurses and Allied Health Professionals The second edition of Pharmacology in Clinical Practice (formerly known as Pharmacology in Clinical Nursing Practice) has been extensively revised and updated. The authors are specialists in the fields of clinical research, health sciences education, clinical pharmacy and applied pharmacology. They have endeavoured once again to provide a simplified approach to this complex subject. By illustrating how pharmacological principles apply to clinical practice, they successfully present nurses and allied health professionals with the fundamentals of drug science as well as the basics of pharmacodynamics and pharmacokinetics. The authors have, where applicable, included suitable cross-references to the latest edition of the Standard Treatment Guidelines and Essential Medicines List (EML) for South Africa: Primary Health Care Level, 2008 edition. The principal author and editor, Gustav Schellack, is a clinical research associate in the pharmaceutical industry and specialises in applied pharmacology. Formerly, he lectured in the Department of Nursing Science at the University of Pretoria. Access the Mobi site for this book 2nd edition Pharmacology in Clinical Practice Application Made Easy for Nurses and Allied Health Professionals Gustav Schellack New and revised features include: • A chapter on the nursing management of drug preparations and treatment • Information on the latest legal framework for dispensing and prescribing drugs • Numerous graphics and line drawings • Contemporary trends and developments in the pharmaceutical industry, such as novel concepts in drug research and development, and the use of biotechnology • A guide to accessing and interpreting drug information • Two useful appendices: Appendix A links the South African EML for Primary Health Care to the relevant sections and listings in the text; Appendix B contains notes on patient adherence to, or compliance with prescribed drug therapy • A glossary to explain problematic terminology. 2nd edition Pharmacology in Clinical Practice Pharmacology in Clinical Practice 2nd edition Application Made Easy for Nurses and Allied Health Professionals This is the third in a series of articles on the basics of pharmacology, drug action and pharmacokinetics, in which interactive explanations are used to illustrate the first two of the four basic pharmacokinetic processes, namely absorption and distribution (i.e. the ‘A’ and ‘D’ of the “ADME” processes). This series uses excerpts and diagrams with permission from the 2nd edition of Pharmacology in Clinical Practice: Application Made Easy for Nurses and Allied Health Professionals, and is compiled and expanded upon by the author. ISBN:978-0-702-18656-1 from your WAP-enabled cellphone on Gustav Schellack pharmacology.indd 1 SA Pharmacist’s Assistant [ Spring 2011 ] Introduction 4 In Part 2, a basic overview was given of the four fundamental pharmacokinetic processes, namely absorption, distribution, metabolism and elimination (i.e. the so-called ADME processes). In terms of the first two of these processes, namely absorption and distribution, we focused on defining each process, explaining how the physicochemical characteristics of drug molecules determine the rate (i.e. “speed”) and extent (i.e. “how many of them”) of their movement across biological membranes, as well as describing additional factors such as dissolvability, the nature of various absorptive surfaces, tissue and organ perfusion, and the characteristics of certain, special biological barriers. We also considered the fact that drug distribution is concerned with the movement of drug molecules from the blood stream to various organs and tissue sites in the body. Now, in Part 3, we will focus on the nature of the plasma membrane, and how drug molecules are able to cross this barrier, as well as the interplay between absorption and distribution as pharmacokinetic processes. Can you still remember the different physicochemical properties of drug molecules that allow for their passage across the plasma membrane, either via simple, 04/05/10 16:38:23 In the case of simple, passive diffusion, drugs should preferably have:2 • • • Small molecules (especially in the case of aqueous diffusion) A high degree of lipid-solubility Molecules that do not carry charges (i.e. unionised molecules) In the case of facilitated and exchange diffusion and active transport drugs must:2 • • Resemble the original substrates that are usually transported by the carriers involved in these processes Bind to the actual carrier proteins passive diffusion or facilitated and exchange diffusion and active transport. (ICF). The opposite is true of potassium ions (K+).1-5 Drug molecules move into the bloodstream from their site of administration through the kinetic process of absorption. The plasma membrane is composed of two layers of phospholipid molecules, interspersed with cholesterol molecules and globular membrane proteins. Carbohydrate molecules protrude outward from the membrane surface. This bimolecular layer (i.e. two layers of molecules) is a mere 10 nm thick. Phospholipid molecules have a characteristic “head-and-double-tail” configuration. A polar, hydrophilic (water-soluble) phosphate group forms part of the head, while the double tail is made up of two nonpolar, hydrophobic (lipid-soluble) fatty acid chains. The two layers of phospholipid molecules, due to their specific physicochemical characteristics, are orientated in such a way as to allow for heads to border the two water phases (i.e. the ICF and ECF). This means that the hydrophobic tails are orientated towards one another Absorption, plasma membranes and how drugs cross them Dynamic, flexible and thin membranes that separate their internal and external environments envelop cells and their intracellular organelles. Plasma membranes provide barriers between the intracellular and extracellular fluid compartments of tissue cells. The selective permeability of the membrane allows for the differences in composition of the intracellular and extracellular fluid. Sodium ions (Na+), for example, are found in much higher concentrations in the extracellular fluid (ECF) than in the intracellular fluid Basic Pharmacology and constitute the lipid phase of the membrane (Figure 1).1-5 Membrane proteins fall into one of two groups: integral proteins or peripheral proteins. Transmembrane proteins are integral proteins that span the entire thickness of the membrane. They may be further divided into carrier proteins and channel proteins. Peripheral proteins are found either on the inner or on the outer surface of the membrane. On the inner surface, these proteins are usually attached to integral proteins and are involved in signal transduction and the regulation and control of intracellular functions.1-5 Some membrane proteins also act as catalytic enzymes. Catalysts increase the rate of chemical reactions without taking part in the actual reaction or being present in any of its products. These enzymes catalyse various cellular reactions. Channel proteins form small aqueous pores or channels in the membrane. These channels serve as passageways for selected polar molecules and ions to cross the membrane. These molecules, however, need to be extremely small (i.e. to have a molecular mass of 100 Da or less). Channels that allow specific cations and anions to pass through the membrane are called ion channels. These channels may be gated (either voltage-gated or ligandgated) to regulate the ion movement through them. Water molecules also cross the membrane through these channels or pores. On the other hand, carrier proteins are involved in the active transport of molecules or ions, or in the facilitated and exchange diffusion of particles. Carbohydrate molecules on the cell surface may be bound to lipids, in the form of glycolipids, or to proteins, in the form of glycoproteins and proteoglycans. Proteins, with their carbohydrate constituents, give the membrane an outwardly negative charge and also provide the unique, three-dimensional receptor sites to which hormones, neurotransmitters and autacoids are able to bind.1-5 The unique characteristics of the plasma membrane explain its selective permeability. Drug molecules, which are foreign to the human body, need to utilise available transport processes to enable them to cross these membranes. Ways in which drug molecules may cross the plasma membrane, therefore, include diffusion (which may be passive or facilitated) and active transport.1-5 (A) Diagram of a prototypical cell (B) Close-up of a segment of the cell’s plasma membrane showing the two layers of phospholipid molecules Simple passive diffusion This transport process does not require cellular energy since molecules possess inherent kinetic energy that moves them along their concentration gradients from an area of higher concentration to an area of lower concentration. Small, nonpolar, lipid-soluble molecules, such as the respiratory gases oxygen (O2) and carbon dioxide (CO2), cross the lipid phase with ease by utilising simple, passive, lipid diffusion. Gated ion channels allow selected cations and anions to diffuse through them, along their electrochemical gradients. Polar, water-soluble molecules, which are small enough, can therefore readily move through the channels or pores in the membrane by passive diffusion as well, although this is referred to as aqueous diffusion. A CO2 molecule has a relative molecular mass of 44 Da, while water (H2O) has a molecular mass of only 18 Da. For comparison, a glucose molecule has a molecular mass of 180 Da, haemoglobin 68 000 Da and the plasma protein albumin 69 000 daltons, or 69 kDa.1-5 Facilitated diffusion Carriers are involved in moving larger molecules that are incapable of simply diffusing through the lipid phase across the membrane. This process does not require cellular energy. Active transport ECF ICF + ↑[Na ] Lipid phase Integral protein Water phase Nucleus Plasma membrane ↑[Na+] ECF Two layers of phospholipid molecules Cytoplasm ↑[K+] ICF ‘Head’ and ‘double tail’ Legend: ECF: ICF: ↑[Na+]: ↑[K+]: Water phase Peripheral proteins Extracellular fluid Intracellular fluid High sodium ion concentration High potassium ion concentration : Na+-K +-ATPase pump Figure 1. A segment of the plasma membrane of a prototypical cell, showing the arrangement of phospholipid and protein molecules.2 SA Pharmacist’s Assistant [ Spring 2011 ] ↑[K+] Some molecules require transport across the plasma membrane against their concentration gradient. Energy and carrier proteins are required to achieve this. The Na+-K+ adenosine triphosphatase (ATPase) pump is an excellent example of an active transport process. It directly utilises adenosine triphosphate (ATP). ATPase is a membrane-bound enzyme that acts as the carrier. This pump helps to maintain the high intracellular potassium ion concentration and the high extracellular sodium ion concentration by sequentially moving three sodium ions (Na+) into the ECF for every two potassium ions (K+) that is pumped into the cell.1-5 5 Basic Pharmacology Carrier proteins exhibit specificity for their particular substrates (the substances that they usually carry) and may actually become saturated. Drugs that utilise transport carriers need to resemble the natural substrate, and will compete with these for the binding sites of the carrier protein. The number of drugs that meet the structural requirements for carrier transport is very limited.1-5 From the above-mentioned explanation it is clear that certain physicochemical properties of drug molecules will also determine their ability to cross plasma membranes (or other more specialised biological barriers). These characteristics are:2-5 Lipid-solubility Drugs that are more lipid-soluble tend to penetrate plasma membranes more readily. This physicochemical property is called the lipid-water partition coefficient of a drug. This expresses relative solubility in lipids as opposed to water. Drugs with high partition coefficients are referred to as lipidsoluble. Those with a coefficient that is markedly lower than 0.1 are said to be water-soluble. However, most lipidsoluble drugs can still readily dissolve in water. Only unionised molecules are lipid-soluble. Water-soluble drug molecules that are small enough can cross plasma membranes through aqueous diffusion via channels or pores in the membrane. For example, ethanol has a molecular mass of less than 50 Da. SA Pharmacist’s Assistant [ Spring 2011 ] Molecular size 6 Most drugs have very low relative molecular masses (less than 1 500 Da, with the majority actually having molecular masses of less than 500 Da). Even in the case of lipid-soluble drugs, the higher the molecular mass, the more difficult it will be for the molecules to cross the plasma membrane. Thus, the smaller their molecular size, the more readily drugs cross plasma membranes. Ionisation Charged molecules, or highly polar ones, may carry charges that are complementary to the glycoprotein surface of the plasma membrane, making it difficult for them to cross from the extracellular to the intracellular fluid compartment. Molecules that carry similar charges to the ones on the cell surface may be repelled from it. Molecules that do not carry electrical charges or exhibit polarity are said to be unionised or nonpolar molecules. These molecules are able to cross membranes much more readily than the charged ones. For example, liquid paraffin is composed of large organic molecules that carry hydrophobic groups. Even though it is a highly lipid-soluble substance, it is not absorbed from the gastrointestinal tract because the hydrophilic groups found on the surface of the plasma membranes repel its large hydrophobic molecules. Intracellular pH (7.0) is lower than the pH of the extracellular fluid (7.35). More hydrogen ions (H+-ions or protons) are therefore found inside the cells. The pH of the surrounding medium determines the extent to which drug molecules within the medium are ionised. Most drugs are weak acids or bases. Acids are proton donors and ionise by giving off hydrogen ions, that is, acids ionise through dissociation: HA = A- + H+. Bases ionise through association because they are proton acceptors: BH+ = B + H+. Drugs will accumulate where they ionise (a phenomenon known as “ion trapping”). Therefore, acidic drugs tend to stay in the extracellular fluid, whereas basic drugs tend to accumulate in the intracellular compartment. The degree of ionisation of drug molecules is determined by the pH of the surrounding medium and the pKa of the drug (the pH at which half of the drug molecules are ionised).2-5 Distribution may be regarded as the second of the four kinetic processes. Once drug molecules reach the systemic blood circulation they are transported to other parts of the body. At capillary level these molecules then leave the bloodstream to enter the other fluid compartments of the body. Distribution As already mentioned, the pharmacokinetic process of distribution entails the movement of drug molecules from the bloodstream into the other fluid compartments of the body. As explained in Part 2, drug molecules are not distributed in equal quantities to all tissues and organs of the body. Also, the extent of the distribution of a drug in the body may be expressed as the apparent volume of distribution (Vd). This is the volume into which the specific drug dosage will need to be dissolved for it to reach the same concentration as it does in the plasma. Drugs that penetrate the intracellular fluid compartment therefore have larger apparent volumes of distribution, whereas drugs that are largely plasma-protein bound exhibit much smaller volumes of distribution.2-5 The same factors that determine the rate and extent of the absorption of a drug into the central blood circulation (e.g. following oral administration), will also determine the rate and extent to which the specific drug molecules will be distributed throughout the various fluid compartments, tissues and organs of the body.2-5 In Part 4, we will attempt to illustrate the interplay between absorption and distribution, as well as between these two kinetic processes and the remaining two, by making use of an example from the clinical practice setting. Be sure not to miss the final instalment… Conclusion Drug molecules need to cross a series of biological barriers to reach the central blood circulation (i.e. to be absorbed) and to be distributed to various organ and tissue sites throughout the body. Certain drug molecules may be able to do this more readily, while others may only be able to cross plasma membranes and other physiological barriers to a very limited extent. The ability to cross these membranes and other barriers is dependent upon a number Basic Pharmacology of different factors, including the actual physicochemical nature of the molecules in question, the cross-membrane transport processes involved and a variety of miscellaneous factors. In Part 4, we will conclude our discussion on the four fundamental pharmacokinetic processes, by focusing on metabolism and elimination. Test yourself Give a brief definition of active crossmembrane transport and lipid-water partition coefficient. • Active cross-membrane transport: Some molecules require transport across the plasma membrane against their concentration gradients. Energy and carrier proteins are required to achieve this. The Na+-K+ ATPase pump is an excellent example of an active transport process. • Lipid-water partition coefficient: This expresses the drug’s relative solubility in lipids as opposed to water. Drugs with high partition coefficients are referred to as lipidsoluble. Those with a coefficient that is markedly lower than 0.1 are said to be water-soluble. Briefly distinguish between simple, passive diffusion and facilitated diffusion. Describe how the degree of ionisation of drug molecules will determine their passage across plasma membranes. • Simple passive diffusion: This transport process does not require cellular energy since molecules possess inherent kinetic energy that moves them along their concentration gradients from an area of higher concentration to an area of lower concentration. • Facilitated diffusion: Carriers are involved in moving larger molecules that are incapable of simply diffusing through the lipid phase across the membrane. This process does not require cellular energy. Charged molecules, or highly polar ones, may carry charges that are complementary to the glycoprotein surface of the plasma membrane, making it difficult for them to cross from the extracellular to the intracellular fluid compartment. Molecules that carry similar charges to the ones on the cell surface may be repelled from it. Molecules that do not carry electrical charges or exhibit polarity are said to be unionised or nonpolar molecules. These molecules are able to cross membranes much more readily than the charged ones. • List the most likely factors that could determine the rate and extent of the absorption of a drug from the gastrointestinal tract (both physicochemical and other). 1. • Disintegration and dissolution • Size and nature of the absorptive surface area • Adequacy of the perfusion • Size of the molecules • Degree of ionisation • Degree of lipid-solubility References 2. 3. 4. 5. Meyer BJ, Van Papendorp DH, Meij HS, Viljoen M. Human physiology: chemical, physical and physiological principles. 3rd ed. Lansdowne: Juta and Company Ltd; 2002. Schellack G. Pharmacology in clinical practice: application made easy for nurses and allied health professionals. 2nd ed. Claremont: Juta and Company Ltd; 2010. Brenner GM, Stevens CW. Pharmacology. 3rd ed. Philadelphia: Saunders Elsevier; 2010. Katzung BG, Masters SB, Trevor AJ, editors. Basic and clinical pharmacology. 11th ed. New York: McGraw-Hill Medical Publishing Division; 2009. Buxton ILO. Pharmacokinetics and pharmacodynamics: the dynamics of drug absorption, distribution, action, and elimination. In: Brunton LL editor. Goodman and Gilman’s the pharmacological basis of therapeutics. 11th ed. New York: McGraw-Hill Medical Publishing Division; 2006. SA Pharmacist’s Assistant [ Spring 2011 ] 7