Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
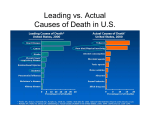
State Epidemiological Profile Alcohol, Tobacco, and Other Drugs Consumption and Consequences March 2006 Bureau of Prevention Services Division of Public Health Services New Hampshire Department of Health and Human Services Strategic Prevention Framework - Assessment Page 1 Contents Section I: State Epidemiological Profile 3 Across the Life-Span Consumption of Alcohol, Tobacco, and Other Drugs in New Hampshire and Northern New England States according to the National Survey of Drug Use and Health Section II: State Epidemiological Profile 8 Adult Consumption of Alcohol, Tobacco, and Other Drugs in New Hampshire according to the Behavior Risk Factor Surveillance Survey (BRFSS) Section III: State Epidemiological Profile 18 New Hampshire SEDs Consequence Data for Alcohol, Tobacco and Other Drugs Section IV: State Epidemiological Profile 31 High School Youth Consumption of Alcohol, Tobacco, and Other Drugs in New Hampshire using the Youth Risk Behavior Survey Strategic Prevention Framework - Assessment Page 2 Section I: State Epidemiological Profile Across the Life-Span Consumption of Alcohol, Tobacco, and Other Drugs in New Hampshire and Northern New England States according to the National Survey of Drug Use and Health In this section data are presented to profile the consumption patterns in New Hampshire, Vermont, and Maine. The data were obtained across the lifespan using the 2002-2003 National Survey on Drug Use and Health (NSDUH), Substance Abuse and Mental Health Services Administration (SAMHSA), and the U.S. Department of Health and Human Services (DHHS). The NSDUH is the only national source that currently provides prevalence of use estimates for both adolescents and adults for every state. Like most national surveys, the NSDUH has limitations. For example, estimates for New Hampshire are based on relatively small samples. Although augmented by model-based estimation procedures, estimates for specific age groups have relatively low precision (i.e., large confidence intervals). Also, the estimates are subject to bias due to self-report and non-response (refusal/no answer). (Note: the NSDUH employs an interview methodology and the SEDs database reports life-span age groups somewhat differently than similar measurements reported elsewhere). Alcohol Consumption Nearly 100,000 deaths each year in the U.S. are attributed to alcohol use or misuse. Research has shown that youth who begin drinking at an early age are at increased risk of problem drinking later in life. In addition, purchase and consumption of alcohol by persons under the age of 21 is illegal. Current Use of Alcohol by Persons Aged 12 and Older. Current use of alcohol is defined as the percent of persons reporting any use of alcohol within the past 30 days. As shown in Figure 1-4, the populations reporting alcohol use in the last 30 days shows similar patterns across Northern New England with the 18-25 year age group showing the most consumption, eclipsing the 12-17 age group by nearly 50%. Strategic Prevention Framework - Assessment Figure 1-4 Page 3 Current Binge Drinking by Persons 12 and Older. Binge drinking is defined as the percent of persons reporting having five or more drinks at least once within the past 30 days. The consumption of five drinks or more within a short time span is commonly referred to as binge drinking. Binge drinking is strongly associated with injuries, motor vehicle crashes, violence, fetal alcohol spectrum disorder, chronic liver disease, and a number of other chronic and acute conditions. As shown in Figure 1-5 below, the three Northern New England states, including New Hampshire, show high rates (40% or more) of binge drinking. In New Hampshire, nearly half of adults aged 18-25 report binge drinking in the past 30 days. Figure 1-5 Tobacco Consumption Each year in the United States, more than 400,000 deaths are attributed to cigarette smoking, making it the leading preventable cause of death. Research has shown that smoking increases the risk of heart disease, cancer, stroke, and chronic lung disease. Environmental tobacco smoke has also been shown to increase the risk for heart disease and lung cancer among nonsmokers. Careless smoking is the leading cause of fatal fires in the United States. Strategic Prevention Framework - Assessment Page 4 Current Cigarette Smoking by Persons Aged 12 and Older. Cigarette smoking is defined as the percent of persons who reported smoking a cigarette on one or more days within the past 30 days. Limitations on this measure include the fact that it does not convey the lifetime or current number of cigarettes smoked. As in the alcohol consumption data reported above, the Northern New England States show similar patterns of tobacco consumption, with the 18-25 age group showing over 40% cigarette use (Fig. 1-6). Figure 1-6 Marijuana Consumption Marijuana use is associated with adverse physical, mental, emotional, and behavioral changes. Sustained use can lead to addiction. The types of negative health impact include respiratory illnesses, memory impairment, and weakening of the immune system. Current Use of Marijuana by Persons Aged 12 and Older. Marijuana use is defined as the percent of persons aged 12 and older reporting any use of marijuana within the past 30 days. As shown in Figure 1-7, marijuana use in the past 30 days is relatively common in New Hampshire and Northern New England with approximately one in four persons in the 1825 age group reporting use. Note that marijuana use drops off to approximately 5% in the older population in NH. Strategic Prevention Framework - Assessment Page 5 Figure 1-7 Drug Consumption Illicit drugs have varying degrees of negative physical and psychological effects depending on the class of drugs used. Dependence and serious medical conditions can result from chronic use of such drugs. Serious medical conditions can stem from the chronic and occasional use of a drug itself, but can also follow from the method of drug administration or the use of contaminated equipment. Figure 1-8 Strategic Prevention Framework - Assessment Page 6 Current Use of Illicit Drugs Other Than Marijuana by Persons Aged 12 and Older. This indicator categorizes the percent of persons aged 12 and older reporting use of any illicit drug other than marijuana, or an abusable product that may be obtained legally, on one or more days within the past 30 days. Drug categories may include cocaine, heroin, and hallucinogens such as LSD, PCP, peyote, mescaline, mushrooms, and ecstasy. They may also include prescription drugs and inhalants such as amyl nitrate, cleaning fluids, gasoline, paint, and glue. Northern New England states exhibit similar patterns and abuse rates across age groups (Figure 1-8). New Hampshire shows a nearly 12% abuse rate in the 18-25 age group, nearly double the rate of teens under 18 and four times that of older adults. Strategic Prevention Framework - Assessment Page 7 Section II: State Epidemiological Profile Adult Consumption of Alcohol, Tobacco, and Other Drugs in New Hampshire according to the Behavior Risk Factor Surveillance Survey (BRFSS) The Behavioral Risk Factor Surveillance System (BRFSS) is an ongoing telephoneadministered adult level survey that is supported by the Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, and the Centers for Disease Control and Prevention (CDC). The BRFSS was developed and conducted by the CDC to monitor state-level prevalence of behavioral risks among adults that are associated with premature morbidity and mortality. The survey collects data on actual behaviors that would be especially useful for planning, initiating, supporting, and evaluating health promotion and disease prevention programs. The BRFSS provides prevalence estimates of adult use for every state. State-level estimates may be further broken down by age, gender, and race/ethnicity. In this section, data are presented to profile the consumption patterns using four alcohol indicators and two tobacco indicators for adults in New Hampshire according to the BRFSS. The data are first presented for 2003 across three age groups (18-34, 35-54, 55+). The indicators are then presented with gender breakdowns over a multiple year time period. Similar to the NSDUH and other national surveys, the BRFSS has limitations. For example, the BRFSS is a telephone survey subject to potential bias due to self-report, non-coverage (households without phones), and non-response (refusal/no answer). In addition, estimates for subgroups may have relatively low precision. For example, estimates for New Hampshire are based on relatively small sample sizes. Alcohol Consumption Indicators In the previous section it was noted that alcohol use or misuse is related to scores of deaths each year and to many other negative individual, family, and community consequences. Alcohol consumption indicators are listed below: Current Use of Alcohol by Persons Aged 18 and Older. Current use of alcohol is defined as percent of persons aged 18 and older reporting any use of alcohol within the past 30 days. Current Binge-Drinking by Adults Aged 18 and Older. Binge drinking is defined as percent of persons aged 18 and older reporting having five or more drinks on at least one occasion within the past 30 days. Current Heavy Use of Alcohol by Adults Aged 18 and Older. Heavy use is defined as the percent of women aged 18 and older reporting a average daily alcohol consumption greater than one drink per day and the percent of men aged 18 and older reporting an average daily alcohol consumption greater than two drinks per day. Strategic Prevention Framework - Assessment Page 8 Drinking and Driving Among Adults 18 and Older. Drinking and driving is defined by percent of adults aged 18 and older reporting driving one or more times in the past 30 days when they “have perhaps had too much to drink.” 18-34 Age Group Alcohol Consumption Indicators in 2003 Figure 2-1 Figure 2-1 indicates an alcohol use rate in this age group of approximately 70 % and a binge-drinking rate of 44% Strategic Prevention Framework - Assessment Page 9 35-54 Age Group Alcohol Consumption Indicators in 2003 Figure 2-2 Figure 2-2 indicates that the alcohol use rate in this age group is comparable to the younger age strata, but the binge-drinking rate of 21% is almost half the younger group. 55+ Age Assessment 55+ Group Alcohol Consumption Indicators in 2003 Figure 2-3 Figure 2-3 indicates that the alcohol use rate in this age group is somewhat lower than younger age groups and similar prior age comparisons. The binge-drinking rate of 10% is almost half the next younger age strata. Capacity Page 10 Tobacco Consumption Indicators Previous discussions on smoking indicated hundreds of thousands of deaths each year attributed to cigarette smoking. The SEDs data with BRFSS indicators features two smoking measures as follows. Current Use of Cigarettes by Adults Aged 18 and Older. Reported as a percent, use of cigarettes is when persons aged 18 and older report smoking 100 or more cigarettes in their lifetime and also now smoke cigarettes either every day or on “some days.” Current Daily Use of Cigarettes Among Adults. Daily use is the percent of adults aged 18 and older who report smoking 100 or more cigarettes in their lifetime and also now smoke cigarettes every day. Figures 2-4, 2-5, and 2-6 show how smoking related behavior decreases across age categories. However, the decrease is only about 10% in current daily use from the youngest to oldest adult age groups. Whereas nearly 22% of the 18-34 year age group reports daily smoking, 12% of the 55+ age group continue the practice into middle age and beyond. 18-34 Age Group Tobacco Consumption Indicators in 2003 Figure 2-4 Assessment Capacity Page 11 35-54 Age Group Tobacco Consumption Indicators in 2003 55+ Age Group Tobacco Consumption Indicators in 2003 Figure2-5 Figure 2-6 Assessment Capacity Page 12 Alcohol and Tobacco Consumption Indicators over Year by Gender The SEDs version of the BRFSS breaks out the alcohol and tobacco indicators by year and gender. The figures that follow note differences in BRFSS data by gender. (Note that the data as reported below omits certain indicators in selected years.) Alcohol Consumption Indicators by Gender and Year Figures 2-7 and 2-8 indicate that males show slightly higher rates for current alcohol use and higher rates for binge drinking (as defined on page 18). For males, the rate of binge drinking is double the rate for females. The differences in the rates for heavy alcohol use or driving after drinking (Figure 2-10) are not large enough to make a distinction based on gender for these indicators. NH Current Alcohol Use by Sex and Year Figure 2-7 Assessment Capacity Page 13 NH Binge Drinking by Sex and Year NH Heavy Alcohol Use by Sex and Year Figure 2-8 Figure 2-9 Assessment Capacity Page 14 NH Driving After Drinking by Sex and Year Figure 2-10 Tobacco Consumption Indicators by Gender and Year Figures 2-11 and 2-12 show parity between males and females over time in cigarette consumption. Although the rates appear slightly higher for males, the relatively small sample size does not justify making a reliable statement about gender differences in the BRFSS. NH Cigarette Use by Sex and Year Figure 2-11 Assessment Capacity Page 15 NH Daily Cigarette Use by Sex and Year Figure 2-12 Assessment Capacity Page 16 Section III: State Epidemiological Profile New Hampshire SEDs Consequence Data for Alcohol, Tobacco and Other Drugs New Hampshire SEDs consequence data for alcohol, tobacco, and other drugs are found in tables related to Mortality, Fatality Analysis Reporting System (FARS), Uniform Crime Reporting System (UCRS), and the National Survey for Drug Use and Health (NHDUH). See below for definitions of systems and surveys. Mortality. The Mortality tables contain age, race, and gender data for mortalities from 1990-2001. The tables maintain an aggregation of individual-level data that were obtained from the National Center for Health Statistics (NCHS) Multiple Cause of Death Public-Use Files. NCHS used the International Classification of Disease-9th revision (ICD-9) system for classifying mortality data to record the underlying cause of death for years 1990-1998. The International Classification of Disease-10th revision (ICD-10) system for classifying mortality data was used to record the underlying cause of death for years 1999-2001. Fatality Analysis Reporting System (FARS). In the SEDs, the Fatality Analysis Reporting System indicator variables are calculated from 1990-2003 crash level and person-level that was downloaded from the National Highway Traffic Safety Administration’s (NHTSA) Fatal Accident Reporting System (FARS), U.S. Department of Transportation, and (numerator). Population estimates from the U.S. Bureau of the Census (denominator). Uniform Crime Reporting (UCR). In SEDs, the UCR of reported crime data were downloaded from the National Archive of Criminal Justice Data website http://www.icpsr.umich.edu/NACJD/ucr.html). The detailed Arrest and Offense Data, 1994-2002, is provide via the United States Department of Justice, Federal Bureau of Investigation. National Survey on Drug Use and Health (NSDUH) The NSDUH is administered by the Substance Abuse and Mental Health Services Administration (SAMHSA), U.S. Department of Health and Human Services (DHHS). The NSDUH is the only national source that currently provides prevalence of use estimates for both adolescents and adults for every state. The indicators and data listed below pertain to certain SAMHSA consequence indicators whose data are found in the tables provided in SEDs. Assessment Capacity Page 17 Alcohol and Illicit Drug Consequences Alcohol Abuse or Dependence. Alcohol Abuse or Dependence is defined as the percent of person’s aged 12 and older meeting DSM-IV criteria for alcohol abuse or dependence. Abuse and dependence are clinical terms used to characterize patterns of alcohol use associated with significant social, psychological, and physical problems for the user and/or others that may be negatively impacted by the user. The data source is the National Survey on Drug Use and Health (NSDUH). Some limitations are evident for this type of data. Some have raised concerns regarding the accuracy of assessing clinical conditions through survey methodology. In defense of the method, however, SAMHSA notes that responses are shown to be consistent with information obtained from peers, parents, and archival records. Figure 3-1 provides data from the National Survey on Drug Use and Health showing Northern New England consequences across the life span. The survey data show similar rates across the states with similar age patterns. As in other consequence data, the 18-25age category stands out for prevalence of illicit drug abuse or dependence. Figure 3-1 Assessment Capacity Page 18 Drug Abuse or Dependence. Drug Abuse or Dependence is defined as percent of person’s aged 12 and older meeting DSM-IV criteria for drug abuse or dependence. Similar caveats and limitations as those made regarding alcohol abuse or dependence also apply to this indicator. Figure 3-2 provides data from the National Survey on Drug Use and Health showing Northern New England consequences across the life span. The survey data show similar rates across the states with similar age patterns. As in other consequence data, the 18-25age category stands out for prevalence of illicit drug abuse or dependence. Figure 3-2 Assessment Capacity Page 19 Chronic Liver Disease Death Rate. The Chronic Liver Disease Death Rate is defined as number of deaths from chronic liver disease per 1,000 people. SAMHSA recognizes that long term, heavy alcohol consumption is the leading cause of chronic liver disease, in particular cirrhosis, the foremost alcohol associated chronic liver disease and is one of the 12 leading causes of death. Although approximately 15,000 people in the U.S. die from cirrhosis each year, the Chronic Liver Disease Death Rate is only based on deaths; cases of cirrhosis morbidity are not reflected in this indicator. In addition, alcohol-related cirrhosis may have a long latency; there may be a lag of several years between changes in behavior and population mortality. The stability of this indicator is directly related to the size of the population in which these deaths occur. Figure 3-3 shows New Hampshire death rates over time by age group. As expected, the highest rates occur for the 55 and over population and vary widely from approximately 0.1/ 1000 to 0.25 / 1000 in a given age group for any given year. Age 55-64 Age 65+ Age 35-54 Age 21-29 Age 30-34 Figure 3-3 Assessment Capacity Page 20 Homicide Death Rate. The Homicide Death Rate is the number of deaths from homicide per 1,000 people. Homicide includes injuries inflicted by others that result in death. The Homicide Death Rate does not involve a direct assessment of alcohol involvement, but rather is justified by the assumption that 30 percent of all homicides are attributable to alcohol. This attributable fraction (30%) could vary substantially across geographic areas and subgroups. Figure 3-4 shows the mean homicide rate for 1995-2001. The graphs indicate that males in the 18-34 age group are at the greatest risk of homicide and males in general are at greater risk than females. Among women, those in the 18-34 age group are at greater risk than those in other groups. Figure 3-4 Figure 3-4 Assessment Capacity Page 21 Suicide Death Rate. The Suicide Death Rate is the number of deaths from suicide per 1,000 people. Suicide includes all means of self-inflicted injuries that result in death. According to SEDs, the association between alcohol use and suicide has been well documented. Suicidal individuals have high rates of alcohol use and abuse and alcohol abusers have high rates of suicidal behavior. Although associated with alcohol consumption, this indicator does not involve a direct assessment of alcohol involvement, but rather is justified by the assumption that 20 percent of all suicides are attributable to alcohol. This attributable fraction (20%) could vary substantially across geographic areas and subgroups, however. Figure 3-5 shows the mean suicide rate from 1995-2001 by age group and gender. Males in the 18-34-age category show the highest rates. Males older than 17 years show higher suicide rates than females in general. Figure 3-5 Assessment Capacity Page 22 Deaths from Illicit Drug Use. Deaths from illicit drug use is defined as the number of deaths directly attributable to illicit drug use per 1,000 people. Deaths that are directly attributable to illicit drug use include drug psychoses, drug dependence, nondependent abuse of drugs, and polyneuropathy due to drug use. The indicator only includes deaths; illicit drug-related morbidity is not reflected. Deaths in which drugs may have been a contributing but not primary cause are not included. Figure 3-5 provides a Northern New England comparison of the above mentioned alcohol related mortality indicators in 2001. Neither homicide nor drug abuse death rate stand out in New Hampshire among other Northern New England States, especially when compared to alcohol related cirrhosis or suicide. Alcoholic cirrhosis death rates are considerably higher in NH (.54) than in either Maine (.43) or Vermont (.31). New Hampshire suicide rates (1.32) are also higher than either Maine (1.26) or Vermont (1.18). Figures 3-4 and 3-5 show age and sex breakdowns in greater detail of homicide and suicide respectively. Percent of Fatal Motor Vehicle Crashes that are Alcohol Related. Of the millions of crashes in the U.S. each year, approximately 41 percent of traffic fatalities are the result of drinking and driving. Alcohol-related traffic crashes remain the single greatest cause of death among youth and young adults. This indicator is defined as percent of motor Figure 3-5 Assessment Capacity Page 23 vehicle crashes in which at least one person died and for which at least one driver, pedestrian, or cyclist had been drinking (Blood Alcohol Concentration >0.00). The limitations on these data are quite evident. Although efforts are made to obtain the BAC values for all drivers involved in fatal crashes; these data are not complete. Therefore, the National Highway Safety Transportation Association has estimated driver BAC for cases missing data. Figure 3-6 shows that in New Hampshire from 1991 to 2003 the percent of fatal crashes due to alcohol has been trending downward by nearly 7.5% in 6 years. Figure 3-6 Alcohol related crash data are displayed in two primary ways in the Fatality Analysis Reporting System (FARS). One indicator is the Alcohol-Related Vehicle Death rate that is defined as the number of vehicle deaths in which at least one driver, pedestrian, or cyclist had been drinking (Blood Alcohol Concentration >0.00) per 1000 people. The second indicator is Alcohol-Involved Drivers Among All Drivers in Fatal Crashes defined as percent of drivers involved in fatal crashes (i.e., in which at least one person died) who were found to have Blood Alcohol Concentrations >0.00. Alcohol-Related Vehicle Death Rate. Figure 3-7 shows rate of death for alcohol versus non-alcohol related car crashes from 1990-2003. The rate of alcohol related deaths tracks lower than non-alcohol deaths and has been trending downward since 1999. Assessment Capacity Page 24 Figure 3-7 Figure 3-8 shows alcohol involved crash deaths in terms of numbers of deaths (as opposed to rates) from 1995 – 2003 separated out by age and gender. The graph shows that most vehicle deaths occur with males, especially those in the 18-34-age range. Figure 3-8 Figure 3-9 also shows alcohol involved crash deaths, but in terms of rate per 1000 between 1995 – 2003 separated out by age and gender. This graph emphasizes the fact that most vehicle deaths in New Hampshire are occurring in men aged 18-34. Assessment Capacity Page 25 Figure 3-9 Figures 3 -10 and 3 –11 show that New Hampshire ranks below the mean in 2003 and 2004 when compared to other states and territories in terms of alcohol-related fatalities in crashes. The histogram shows that in 2003 New Hampshire exhibited at fatal crash rate of 0.40 / 1000 compared with an across state average of 0.41 / 1000 and in 2004 New Hampshire fared even better with the death rate dropping to 0.35 / 1000 compared to an across state average of 0.39 / 1000. Figure 3-10 Assessment Capacity Page 26 Figure 3-11 Alcohol-Involved Drivers (Among All Fatal Crashes). The Alcohol-Involved Drivers Among All Fatal Crashes indicator measures the drivers involved in fatal crashes (i.e., a crash in which at least one person died) who were found to have Blood Alcohol Concentrations >0.00. Figure 3-12 Figure 3-12 shows alcohol involved crash deaths in terms of numbers of driver deaths between 1995 – 2003 separated out by age and gender. Since the data in this chart are not mutually exclusive with the above data (i.e., deaths of drivers also counts in the vehicle death statistics), it is not surprising that most drivers in vehicle deaths are males, especially those in the 18-34-age range. Assessment Capacity Page 27 Figure 3-13 Figure 3-13 shows alcohol involved crash deaths in terms of rate per 1000 of driver deaths between 1995 – 2003 separated out by age and gender. Data in this chart match the previous chart (Figure 3-12) on Alcohol-Related Vehicle Death Rate. Males in the 18-34-age category appear most at risk. Tobacco Consequences Deaths from Lung Cancer. Deaths from lung cancer are defined as the number of deaths from lung cancer per 1,000 populations. Lung cancer often results from long-term tobacco use and is the most common form of cancer mortality in the U.S. Eighty to 90 percent of all lung cancer is attributable to cigarette smoking. In 1998, there were slightly more than 125,000 smoking-attributable lung cancer deaths. In 2001 598 New Hampshire residents died from lung cancer. The rate per 1000 was 0.52, slightly less than rates in other Northern New England States (see Figure 3-14). Deaths from Cardiovascular Diseases. Deaths from Cardiovascular Diseases are an indicator that SAMHSA recommends with reservations. The definition of the indicator is the number of deaths from cardiovascular disease per 1,000 populations. The reservations relate to the fact that it is only based on deaths; cases of morbidity from cardiovascular disease are not reflected in this indicator. In addition, cardiovascular disease is not a single disease, but rather numerous diseases with different causes and risk factors. Cigarette smoking is one of many behaviors that Assessment Capacity Page 28 may contribute to cardiovascular disease. In any case, cigarette smoking is considered the most preventable cause of cardiovascular disease. There were approximately 113,000 smoking-attributable cardiovascular disease deaths in 1998. In New Hampshire during 2001, 625 persons died due to cardiovascular disease. New Hampshire’s rate of 0.51 per 1000 is somewhat lower than rates in Maine (0.77) or Vermont (0.67). (See Figure 3-14). Deaths from COPD and Emphysema (Lung Disease). Lung Disease is defined as the number of deaths from COPD and emphysema per 1,000 populations. According to SAMHSA, approximately 80 percent of chronic obstructive pulmonary (COPD) and emphysema disease deaths are attributable to smoking. The limitations of this indicator include the fact that it is only based on deaths; cases of morbidity from respiratory disease are not reflected in this indicator. Death from respiratory disease reflects longterm, chronic cigarette smoking; it may be many years before changes in smoking affect population mortality. In New Hampshire and across Northern New England, Lung disease deaths occur at about the same rate as lung cancer or cardiovascular deaths (0.5 / 1000). The mortality rate for ischemic cerebrovascular death is reported in Figure 3-14, but it is not an “official” SEDs indicator. Ischemic cerebrovascular death rates are 4 to 5 times in magnitude compared to other causes of death, and a similar pattern is observed among Northern New England states. Figure 3-14 Assessment Capacity Page 29 Section IV: State Epidemiological Profile High School Youth Consumption of Alcohol, Tobacco, and Other Drugs in New Hampshire using the Youth Risk Behavior Survey The Youth Risk Behavior Survey System (YRBSS) was developed in 1991 by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention to monitor priority health risk behaviors that contribute markedly to the leading causes of death, disability, and social problems among youth and adults in the United States. The most notable weakness of the YRBSS is limited representation; students who have dropped out of school are not included. In addition, consistent with other school-based surveys, the YRBSS is subject to bias due to self-report, non-coverage (refusal by selected schools to participate), and non-response (refusal/no answer). In this Section of the New Hampshire, profile data are presented to characterize the 2005 consumption patterns of youth in New Hampshire high schools using the Youth Risk Behavior Surveillance Systems (YRBSS). The analysis is presented using two different samples. State Randomized Sample. One sample, known as the State sample, provides weighted rates from CDC's randomized administration (N=1276). The data from this sample are comparable to previous data collections and are presented as rates (%) derived from dichotomized survey items. For each of the eight indicators listed below, the results of the state sample are presented in text form as a percent followed by a breakout by gender. Local Self-selected Sample. A second self-selected sample is also reported for high schools in New Hampshire that surveyed the entire school (16,133 students). These data are reported as a histogram of 24 schools in terms of rates (%) derived from dichotomized survey items. Using this method, it is easy to visualize the variability of the indicator from school to school. For example, in the indicator Current Use of Alcohol by High School Students, the randomized sample rate was 44% for the State with a 95% confidence interval of 39.5% to 48.6%. This rate is reported in text below the indicator listed. In comparison, the histogram of the self-selected sample showed that the average rate for schools was a similar 44.7% with a standard deviation of 5.5%. Although the statistics are almost identical, the histogram shows that the range of indicator for each school is from a low of nearly 35% for the school with the lowest rate to nearly 60% for the school with the highest rate. Based on this analysis, the reader can garner a greater understanding of the underage drinking problem as it applies to individual schools. Assessment Capacity Page 30 Current Use of Alcohol by High School Students (Figure 4-1). Percent of students in grades 9 through 12 reporting any use of alcohol within the past 30 days. 44.0% (39.5 - 48.6) of the students had at least one drink of alcohol on one or more of the past 30 days. (43.4% males; 44.8% females)1. Figure 4-1 Current Binge Drinking by High School Students (Figure 4-2). Percent of students in grades 9 through 12 reporting having five or more drinks in a row (i.e., within a couple hours) on at least one occasion within the past 30 days. 28.4% (24.5 – 32.3) of the students had 5 or more drinks of alcohol in a row; that is, within a couple of hours, on one or more of the past 30 days. (29.4% males; 27.6% females)1 Figure 4-2 Assessment Capacity Page 31 Early Initiation of Alcohol Use (Figure 4-3). Percent of students in grades 9 through 12 who report first use of alcohol before age 13 (more than just a few sips). 19.3% (16.2 – 22.4) of the students had their first drink of alcohol other than a few sips before age 13. (20.7% males; 17.7% females)1 Figure 4-3 Current Use of Cigarettes by High School Students (Figure 4-4). Percent of students in grades 9 through 12 reporting smoking a cigarette on one or more days within the past 30 days. 20.5% (17.3 – 23.8) of the students smoked cigarettes on one or more of the past 30 days. (19.0% males; 22.5% females)1 Figure 4-4 Assessment Capacity Page 32 Early Initiation of Cigarette Use (Figure 4-5). Percent of students in grades 9 through 12 reporting that they smoked a whole cigarette for the first time before age 13. 12.6% (10.4 – 13.9) of the students smoked a whole cigarette for the first time prior to age 13. (12.5% males; 12.7% females)1 Figure 4-5 Early Initiation of Marijuana Use (Figure 4-6). Percent of students in grades 9 through 12 reporting first use of marijuana before age 13. 7.1% (5.4 – 8.9) of the students tried marijuana for the first time before age 13. (8.3% males; 5.8% females)1 Figure4-6 Assessment Capacity Page 33 Current Use of Marijuana by High School Students (Figure 4-7). Percent of students in grades 9 through 12 reporting any use of marijuana within the past 30 days. 25.9% (22.6 – 29.2) of the students used marijuana one or more times during the past 30 days. (28.8% males; 22.8% females)1 Figure 4-7 Current Use of Cocaine by High School Students (Figure 4-8). Percent of students in grades 9 through 12 reporting any use of cocaine within the past 30 days. 3.3% (2.4 – 4.2) of the students used any form of cocaine including powder, crack, or freebase, one or more times during the past 30 days. (3.3% males; 3.3% females)1 State Only. Sample The Figure 4-8 following set of indicators report only data from the state sample and pertain to use of very specific classes of drugs used during the student’s lifetime. Note that the rates for Assessment Capacity Page 34 this class of consumption do not reflect current use but focus on use during the life of the student. Percent of High School Students Reporting Any Use of Specific Classes of Illicit Drugs in Their Lifetime. Percent of students in grades 9 through 12 reporting using: • Cocaine • Inhalants • Heroin • Methamphetamine • Ecstasy (MDMA) • Steroids • any drugs via injection one or more times during the lifetime (each category assessed separately). 9.0% (7.0 – 10.9) of the students used any form of cocaine, including powder, crack, or freebase, one or more times during their life. (9.8% males; 8.2% females)1 11.3% (8.9 – 13.7) of the students sniffed glue, breathed the contents of aerosol spray cans, or inhaled any paints or sprays to get high one or more times during their life. (9.5% males; 13.1% females)1 2.1% (1.2 – 2.9) of the students used heroin one or more times during their life. (2.0% males; 2.1% females)1 5.5% (4.1 – 6.9) of the students used methamphetamines one or more times during their life. (6.8% males; 4.2% females)1 5.5% (3.8 – 7.1) of the students used ecstasy one or more times during their life. (5.1% males; 5.9% females)1 3.0% (2.0 – 4.1) of the students took steroid pills or shots without a doctor's prescription one or more times during their life. (3.4% males; 2.6% females)1 1.8% (1.0 – 2.5) of the students used a needle to inject any illegal drug into their body one or more times during their life. (1.5% males; 2.0% females)1 Appendices